Monthly Shaarli
April, 2023

A documentary of pianist Glenn Gould's 1957 tour of Soviet Russia. Several sections are muted, apparently because of copyright issues. Just perservere - the sound will resume.
I found myself responding to this with a lot of emotion. Gould seems to resonate with the Russian spirit. Something comes across that can't be expressed with words.

When I originally made this Substack, I found myself in a very frustrating position—I had something I felt was essential for the world to know (that we were repeating the disastrous smallpox vaccination campaign, its cruel mandates, and the widespread counterprotests against them by the working class). Still, I had no way to get the message out. I tried to find a way to do so for a while, and eventually, Steve Kirsch generously gave me a platform to do so.
Because of this, I have a considerable degree of empathy with people who find themselves in a similar position to mine. Thus one of my goals in building the subscriber base here has been to make that platform available to those in a similar situation to me, and I periodically publish compelling things readers share with me I believe are accurate (e.g., this citizen’s survey of blood clots amongst the vaccinated).
Recently a longtime reader contacted me to share his story. Based on my previous correspondences with him over the last year, I believe he has accurately represented himself here. I also want to note that his story shares many parallels to the treatment of other doctors attempting to do the right thing throughout COVID-19 (e.g., Paul Marik’s experience).
One of the reasons we lack doctors everyone wants to see is because those who try to do the right thing get pushed out of the system. Because there is so much corporate control of medicine, even doctors who want to do the right thing know they have no recourse if the hospital turns against them. Those doctors thus have to choose between toeing the line and doing their best within those circumstances or leaving the system entirely.
Their leaving thus leaves even fewer physicians that patients would want to see available within the corporate medical system. For many things like emergent hospital care, the patients cannot address the issue by simply opting out of the system. These problems worsened during COVID-19, particularly in the blue states, which has created the unfortunate situation where patients often have to travel out of state for the care they need, which is immensely unfair, especially to those who aren’t somewhat wealthy.
Dr. Miller’s Story
My Covid 19 Cancellation Story April 9, 2023
I am a physician who stood against the false narratives swirling around COVID and for a time, it seemed like I lost.
Before COVID became a public reality, I was working as a successful Trauma Surgeon and Surgical ICU Physician in the hospital that had the first diagnosed COVID case in America. I was working as one of the more senior surgeons of a team of 12 surgeons. The hospital and medical community had already been struggling prior to COVID with various departures from reality with narratives including ‘racism everywhere’ and ‘diversity as long as it supports deviancy,’ but it wasn’t appearing to dramatically affect patient care.
[Dr. Miller’s surgical specialty currently requires 6-7 years of grueling training after completing medical school and thus pays a high salary. Because of the investment required to obtain it, most doctors are reluctant to ever part with it].
In 2018-2019, I stumbled onto a fraud scheme perpetrated by some of the administrative doctors in our hospital that did cause patient harm, so I reported our hospital administration for fraud. I similarly observed and discovered other connected issues that caused patient harm, by various other providers, that I tried to bring to light in our hospital. I was “rewarded” with 12 complaints filed against me over a 2-week period, in retaliation. These complaints accused me of breaches of almost every aspect of professional behavior and ethics. It followed one of the administrators sending out an email asking her colleagues to ‘get rid of Dr. Miller.’ None of these allegations stood (they were all false to begin with), and I continued to do my job to the best of my abilities in this hostile situation, but it became increasingly difficult. Eventually, every single complaint was dismissed as unsubstantiated.
Then, through February and March of 2020, our hospital had a large number of COVID patients including a real upsurge of many sick patients in early March. A couple weeks later, it hit the news, but only AFTER the virus had passed its inflection point in our hospital and AFTER our healthcare system was not in any threat of having inadequate resources. Things then went completely mad with hype and fear- again, this was AFTER the real infectious surge was past.
Suddenly, our hospital outcomes and quality data became hidden and opaque to us. Prior to this, most all data was openly shared and discussed in quality assurance meetings. The hospital forced upon us a narrative that was pure lunacy and contrary to all available observations and previously available data. A chilling example is the following: I was working a shift in the ICU in late April 2020 and had basically nothing to do because greater than half our beds were empty. We were “low censusing” any nurses willing to go home because there were so few sick patients. I was having a cup of coffee, chatting with the staff and another ICU physician, who was in leadership, when the daily newspaper was delivered. Prior to the paper being delivered, we were all relaxed, jocular, and noting how little work we all had. The other ICU physician picked up the local paper where the main headline said, ‘Local ICU Overwhelmed.’ The article was referencing our ICU, as we were the only hospital in the county. He looked at me, started sweating, panicked, and said, “What are we going to do? We may not be able to handle this!” I replied with, “Pour another cup of coffee and laugh at the morons writing the paper.” He became visibly distressed and left to call the hospital administration about the situation, who confirmed they were complicit with the newspaper article. This colleague was one of the medical directors of our ICU. Our hospital and ICU were not overfull at the peak number of infections in March 2020. In fact, the ICU was never overfull, even after the horrible protocols that hurt so many patients were established. I knew we were in serious trouble as a medical community when clinical leaders started believing the words in a newspaper and hospital administrators more than their own eyes and experience.
[Mattias Desmet’s mass formation hypothesis helps explains how people can delude themselves into a reality in stark contrast to the objective evidence in front of them].
Then, I watched as every policy, practice, and quality metric that makes a trauma and surgical program have good patient outcomes be undermined or abandoned by my colleagues and hospital administration. I filed countless complaints to our quality department for disgusting breaches of care that were now becoming commonplace. I could not turn my back on my oaths taken to advocate for patients. Between mid-2020-2021, following a leak of information from the opaque administration, I learned that our unanticipated morbidity and mortality numbers had more than doubled for indexed trauma patients. It was horribly demoralizing to watch.
[This is an excellent example of a society in decline].
After the vaccine was rolled out in late 2020, it became a functional mandate in the broader community, and then definitively mandated by the late summer of 2021. The medical community in the county I was working in (Snohomish, WA) started refusing to care for unvaccinated patients, except in the hospital setting. I couldn’t believe that patients were banned from accessing basic primary care at first, but then I spoke to a man at my church who was denied both refills of his diabetic medications and treatment for a sinus infection by his primary care provider, all because of his COVID vaccination status. This was so inconceivable that I still didn’t believe it! Even when patients did make it to the hospital, I learned that the physicians and staff in the emergency room were directed to provide a lower tier of medicine to this group of patients. It was less than acceptable, and worse, less dignified, than the care given to any other patients pre and post COVID. I had to verify with physician leaders that they approved of this inhumanity. I found out that all the major healthcare systems in the county had agreed to this action, and drove the creation of the policies that demanded physicians act in direct opposition to their oaths. After discovering this, I departed from the medical community in spirit.
[My observation throughout history has been that when a malignant collective ideology takes hold, only 5-10% will be willing to go against it].
Working with my pastor, we turned our church into a free clinic to care for those ostracized from society. I obtained independent malpractice insurance, and we started seeing patients. People were desperate. We didn’t advertise, but there were so many people seeking basic healthcare that we struggled to see everyone. I did my best to see people in their time of need, but it was hard. I was still working in my full-time hospital position. I just didn’t have enough hours in the day. Most of the people I cared for were seen at the church - they were met with maskless smiles, prayer, support, and free medical care. Sometimes, people would be waiting in my driveway for me when I arrived home in the early morning after a night shift or late at night after I finished a day shift. What became obvious as the most important thing about our clinic, is that our patients needed to be treated as valuable people created in God’s image.
Prior to this experience, I was a seasoned/hardened subspecialist with the best reputation one could hope for in the hospitals I worked. When other doctors, health executives, nurses, and local politicians or their families had surgical problems, I was often the one asked to deliver their care even if I wasn’t scheduled to be working. After our health care system abandoned the oaths we took as physicians, I had an identity crisis and pivoted to putting more efforts into the free clinic, caring for the dispossessed patients.
[Throughout my career, I have tried to volunteer in free clinics because I frequently find they are the only place you can focus on helping patients rather than dotting the i’s and crossing the t’s the corporate medical system requires everyone to do].
Eventually, my work at the free clinic treating unvaccinated patients became known, and the hospital administration learned of it. Subsequently, the real pressure against me started. The hospital responded by opening an investigation of me on synthesized charges of ‘micro-aggression.’ There ended up being 2 separate and independent investigations (one by the hospital, one by my physician group leadership who were working in tandem with the hospital) into my conduct. My colleagues, who months earlier asked for my help and guidance about both professional and personal matters, would no longer return my calls, text messages, emails, or speak to me in public, for fear of being labeled as affiliated with me while in my state of political disfavor. The investigations themselves and the repercussions to my reputation were the punishment. I was treated as guilty, even when proven innocent, by the hospital administration and my colleagues. The investigations eventually exonerated me, my behavior, and my healthcare delivery, but left open the possibility for immediate suspension/termination if I committed a ‘micro-aggression’ in the future. Obviously, this was a no-win scenario for me since micro-aggressions are subjective, undefinable, unprovable, and therefore indefensible. I refused to continue working without an independent mediator, so the hospital gladly paid out my contract instead of mediation and restoration.
[One of the things that surprised me about working in hospitals was seeing things I’d previously associated with high school drama transpire inside the facility—something many of my colleagues have also observed].
Separately during this time, I was reported to the State Medical Board by an outpatient pharmacist for prescribing a 2-week course of Fluvoxamine (an anti-depressant) prescription to help a patient recovering after COVID. This prescription had been banned by the Washington State Medical Association as a treatment for COVID or its repercussions. Incidentally, the patient had a positive response and near complete recovery from her illness, but the pharmacist and WSMA didn’t seem to care about that data point but were apparently offended that I violated their protocol.
By March/April of 2022, multiple other clinics in the county began to accept care for most patients, regardless of vaccination status, and so we wound down the free clinic at my church, transitioning people’s care to physicians in established practices who would now agree to deliver appropriate care. As I had been reported to the state (although no formal charges were brought) and I was being pushed out of hospital medicine for practicing ethical medicine, I knew it was time to leave Washington State. The message to me was clear: if I stayed, I would have formal investigations that would prohibit me from obtaining a medical license in another state. My livelihood would be stripped away. So, we sold our homes and boats, liquidated our assets, and moved to South Florida in May 2022. I was, and am, bitter at the establishment of medicine that committed these crimes, so I planned to retire at age 50 with the move and have nothing further to do with the establishment.
[Dr. Miller made the correct decision. Had he not left, he likely would have been permanently barred from practicing medicine in the future. This illustrates a major issue with the current medical board system].
However, after the hurricane came through Florida in the fall of 2022, I started doing volunteer work for hurricane victims. This included some medical relief work. I realized there is still good that can be done in medicine, that people need healthcare providers, and that by nature, I am a healer.
So, in February of 2023, I returned to practicing medicine and started working as a Primary Care Physician at a holistic clinic where no patient is turned away. I discovered that I enjoy being a Family Physician, too. I lost my prestigious career and my social position, but I did not lose my ethics or integrity. I did not violate my oaths of practice. So, ultimately, I have won. And I’m happy.

Conclusion
I applaud Dr. Miller for being willing to share his story publicly. Many physicians over the years have told me that the medical profession's mistake was surrendering too much of each doctor's power to the corporate medical machine. Over the last few years, we have witnessed a direct consequence of this unchecked power grab.
In the future, I believe three concrete steps need to be taken to address this issue:
-
The first is that patients living in blue states must create the political will to have their state governments stop pushing these ridiculous actions. Doing so will likely require directly informing the public that most of the laws and policies being enacted are being done to support corporate interests rather than patients—as directly attacking specific violations of medical freedom has been largely unsuccessful thus far due to it being blended into the red vs. blue partisan dichotomy (which is very difficult to shift in either direction) rather than being portrayed as corruption affecting the entire electorate.
-
The second is that patients need to financially support services and physicians they believe in and, as much as possible, opt out of ones that don't. We are seeing a miniature version of that with Substack, as the legacy media is rapidly losing viewership (since most of what they publish is garbage). Simultaneously journalists are making more on Substack than they did at their old jobs—both of which are putting pressure on the legacy media to stop publishing garbage and making many journalists want to jump ship to Substack.
-
The third is the doctors need to be much more aggressive in taking their power back (they need to band together—potentially with the correct type of union). The corporate medical system cannot function without them, and there is a constant shortage of physicians in the United States, so that position needs to be leveraged to force the corporate medical system to behave rather than perpetuate the current corporate status quo
This is a third talk in a series that began with Relationship Based Medicine , continued with Beware of Doctors Bearing Gifts and concludes with this talk, which could called History of a Medical Psychosis, Medical Neoliberalism, Evident versus Evidence Based Medicine, A Lutheran Moment, or Does Objectivity Come from using Chance to Control Bias or Bias to Control Chance?
It is the most important talk I have ever given.
The first lecture was delivered to clinicians in New York with a Q and A afterwards.
The second was delivered to the public in Lethbridge Alberta, thanks to Jennifer Williams and Dan Johnson but owing to tech difficulties at the venue (See In Memory of Dexter Johnson), it was difficult to record the Q and A with the public. Suffice to say though between the technical difficuties, the lecture and the Q and A, we were all there for the better part of 3 hours and the discussion was great.
This third lecture was delivered to Aaron Kesselheim’s PORTAL group – Program on Regulation, Therapeutics and Law. There are two versions. The History of a Medical Psychosis was recorded by Bill James the day before in case of glitches – same day as Putin and Biden gave speeches. The second was recorded by Aaron – Faulty Evidence and Moral Hazard.
There are slight differences between them. The text and slides below add some detail to both talks but the tone of voice and gestures in the talks likely convey things not in the text.
Slide 1: Faulty Evidence and Moral Hazard
Welcome to a very conservative talk – based on a belief in the medical model and in evaluating the drugs we use thoroughly.
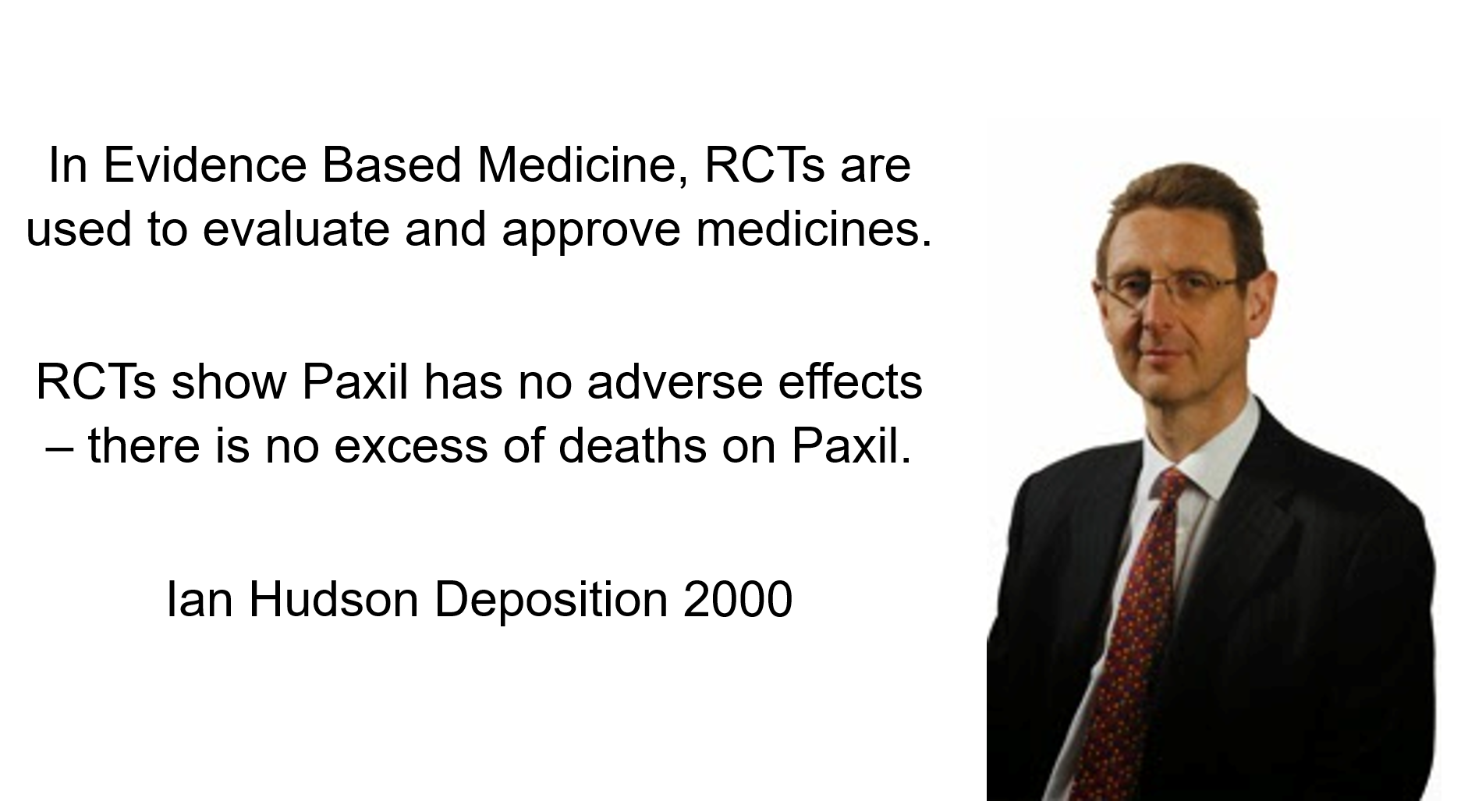
Slide 2: These quotes are a precis of key points in the deposition of Ian Hudson, Chief Safety Officer of GlaxoSmithKline (GSK) in 2000 in the Tobin v SmithKline trial.
Forty-Eight hours after starting Paxil Don Schell shot his wife, daughter and granddaughter and then himself. Hudson is being asked – Can SSRIs cause Suicide?
The jury dismissed Hudson’s Evidence Based Medicine view in favor of Evident Based Medicine and in this Civil trial found GSK guilty of negligence that resulted in the death of this family.
Hudson’s view, however, remains ensconced at the top of Britain’s drugs regulator, of which he was later the CEO – as well as FDA, EMA, TGA, Health Canada, WHO, and Boston institutions like Harvard, MRCT, and Vivli. Joe Biden and the Pope’s advisers will also endorse and tell their bosses to say – Yes RCTs are the Way the Truth and the Light.
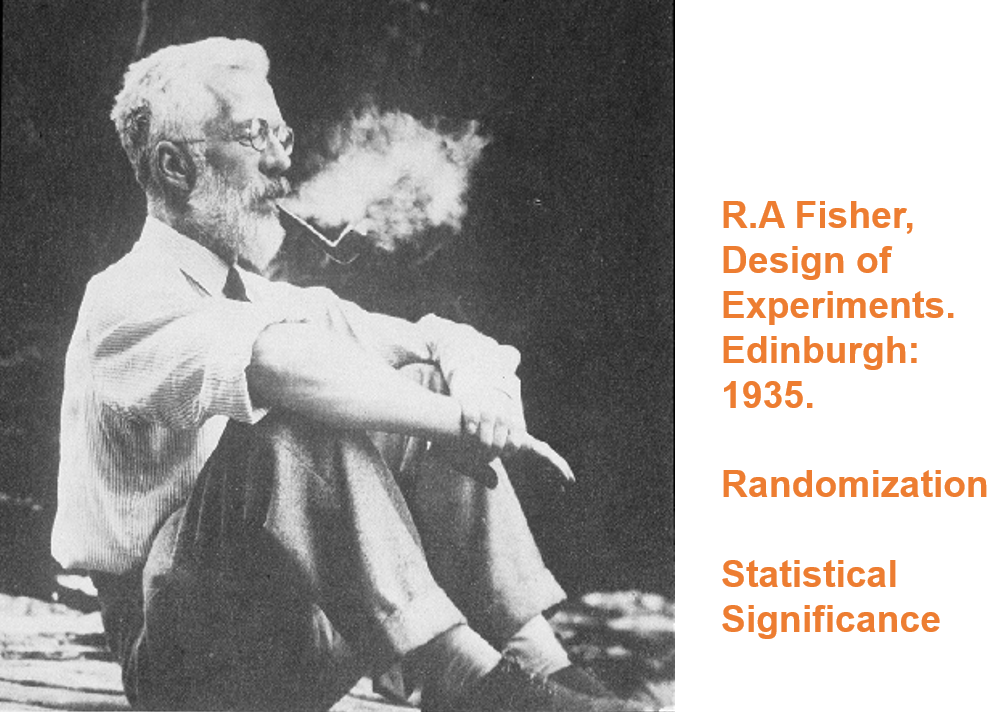
Slide 3: Hudson’s views originate 70 years earlier in the work of a strange man – Ronnie Fisher.
Here you see Fisher smoking a pipe. He dismissed the later link between smoking and lung cancer, saying personality types predisposed to both cancer and smoking. Evidence was not Fisher’s strong point.
He had nothing to do with medicine and never ran an RCT. Controlled trials and randomization were there before Fisher and were no big deal but for no clear reason his book the Design of Experiments transformed what came next.
Fisher ran a thought experiment to characterize expert knowledge. He mentioned randomization as a means to control for any trivial unknown unknowns. Randomization later became semi-mystical.
Fisher’s expert knew parachutes worked so if we set up two groups, one with parachutes and the other not, we might randomize in case there was someone with webbed feet who might behave differently when falling. Otherwise, we would expect those wearing parachutes to live and those not to die – unless a chance strong wind lands a person in snow covered trees.
If randomization eliminated webbing as a factor, the only thing that could get in the way of an expert being right was chance and this could be assigned a statistically significant value. If 1 in 20 of those without parachutes lived we wouldn’t say the expert didn’t know what he was talking about. Fisher was characterizing expertise rather than characterizing an exploration of the unknown.
Randomization can’t control for ignorance.

Slide 4: Fisher’s expert is a Robin Hood who 19 times out of 20 can split a prior arrow lodged in the Bull.

Slide 5: But the trials done to license drugs especially antidepressants look more like this. A mismatch on this scale indicates medical RCTs are nothing like what Fisher had in mind.
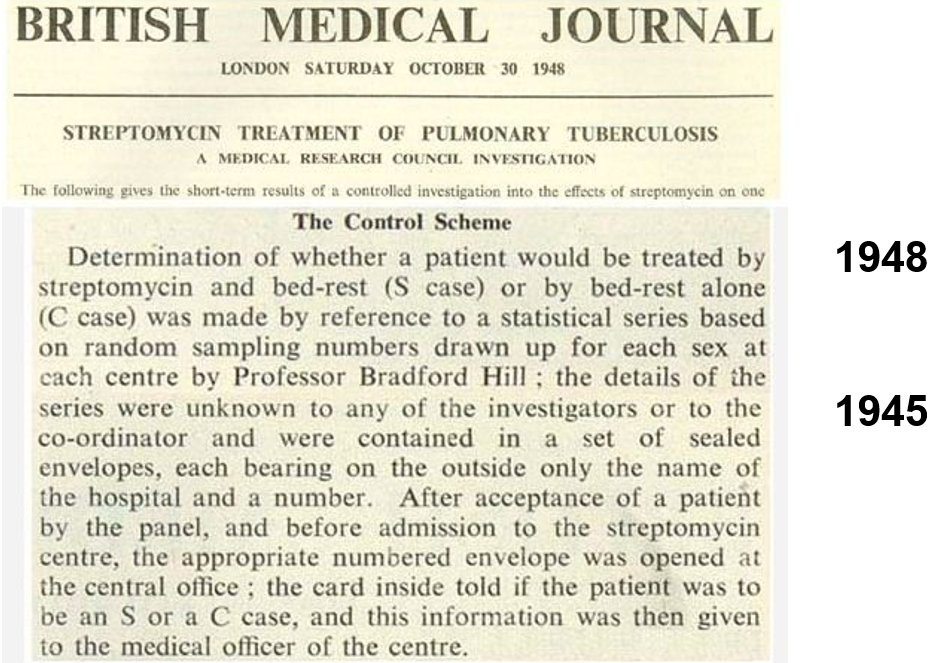
Slide 6: The first RCT in medicine was a trial of streptomycin for tuberculosis. Tony Hill used randomization as a method of fair allocation – he was not managing mystical confounders. Hill helped put the effects of smoking on the map. He had no time for Fisher. He also knew doctors were not experts. His trial was not a demonstration of expertise.
Hill’s RCT found out less about streptomycin than a prior non-randomized trial in the Mayo Clinic, which showed it can cause deafness and tolerance develops rapidly.
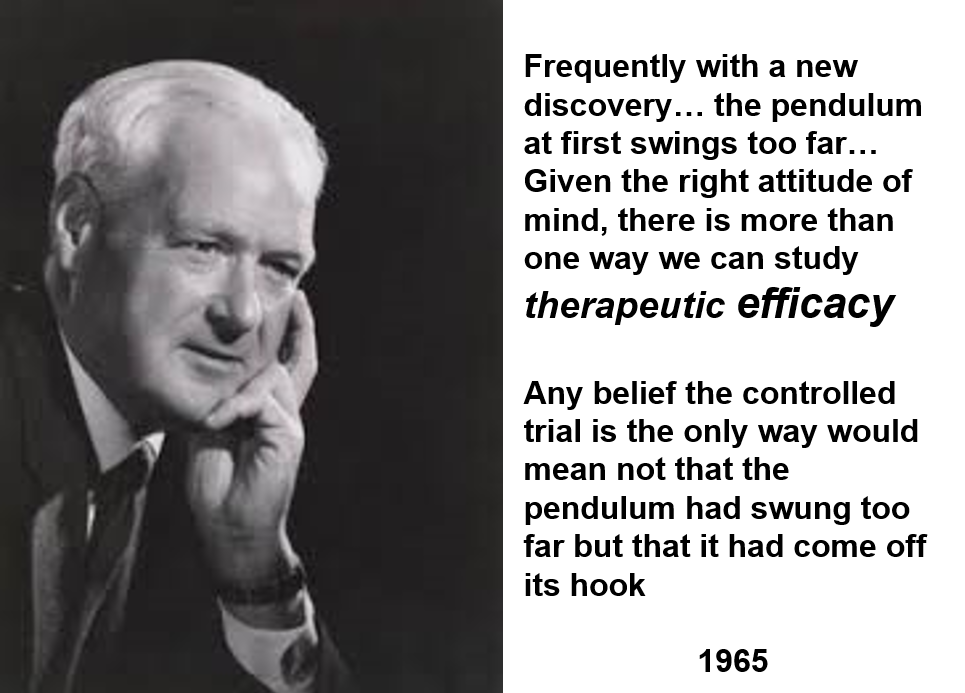
Slide 7: Twenty years later, here is Tony Hill taking stock of controlled trials. In this 1965 lecture, he mentions that it is interesting that the people who are most heavily now promoting controlled trials are pharmaceutical companies.
Hill didn’t think trials had to be randomized. He thought double-blinds could get in the way of doctors evaluating a drug. He was a believer in Evident Based rather than Evidence Based Medicine.
Hill said we needed RCTs around 1950 to work out if anything worked. By 1960 he figured we had lots of things that worked – none of which had been brought on the market through an RCT – and he thought the need was to find out which drug worked best. This is not something RCTs can do – there is no such thing as a best drug. RCTs have instead become a way for companies to get weaker drugs on the market.
He said that RCTs produce average effects which are not much good in telling a doctor what to do for the patient in front of them.
All drugs do 3000 + things – one of which might be useful for treatment purposes. In focusing on one element, by default, Hill is saying RCTs are not a good way to evaluate a drug. All RCTs generate ignorance. But we can bring good out of this harm if we remain on top of what we are doing. Hill never saw RCTs replacing clinical judgement.

Slide 8: This 1960 RCT run by Louis Lasagna makes Hill’s point well. Thalidomide has therapeutic efficacy as a sleeping pill but the trial missed the SSRI-like sexual dysfunction, suicidality, agitation, nausea and peripheral neuropathy it causes.
Two years later, Lasagna was responsible for incorporating RCTs in the 1962 Food and Drugs Act Amendments – in order to minimise the chance of another thalidomide. By doing this, more than anyone else, Lasagna was the man who got us using RCTs
This trial would have licensed thalidomide today. The 1938 Act had no requirement for RCTs.
Slide 9: Many claim RCTs demonstrate cause and effect in a way no other study design can.
The 1950s was a golden age of new drugs that gave us the best antihypertensives, hypoglycemics, antibiotics and psychotropic drugs we have ever had without RCT input into any discoveries.
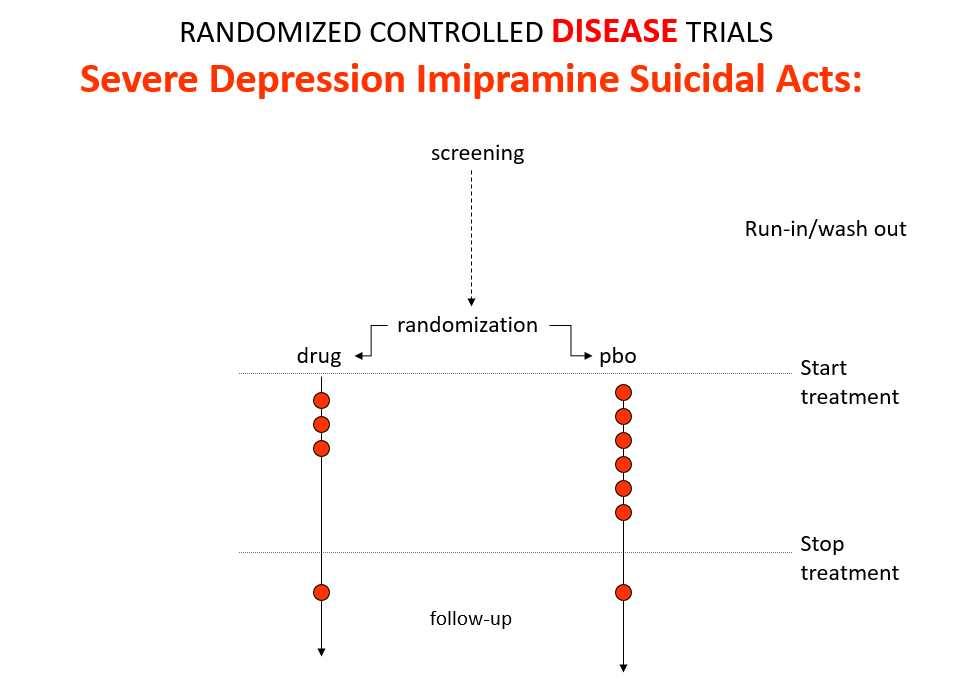
Imipramine was the first antidepressant. It and other antidepressants beat SSRIs in later RCTs. It can treat melancholia – SSRIs can’t. Melancholia comes with a high risk of suicide.
Imipramine was launched in 1958. At a meeting in 1959, European experts made clear that while it was a wonderful treatment imipramine made some people suicidal. Stop the drug and it clears. Re-introduce and it comes back. This was Evident Based Medicine showing this drug can cause suicide.
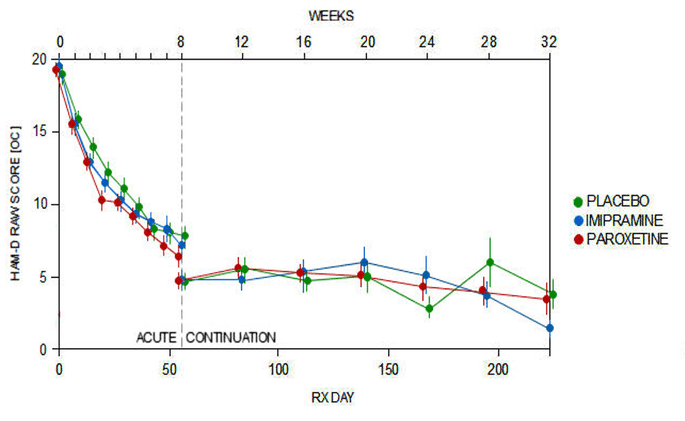
Like Fisher, let’s do a thought RCT of imipramine versus placebo in melancholia. The red dots here are suicides or suicide attempts.
Even though it can cause suicide, we would expect it to reduce the number of suicides because it treats this high risk condition. If you didn’t know better, this RCT would look like evidence antidepressants do not cause suicide.
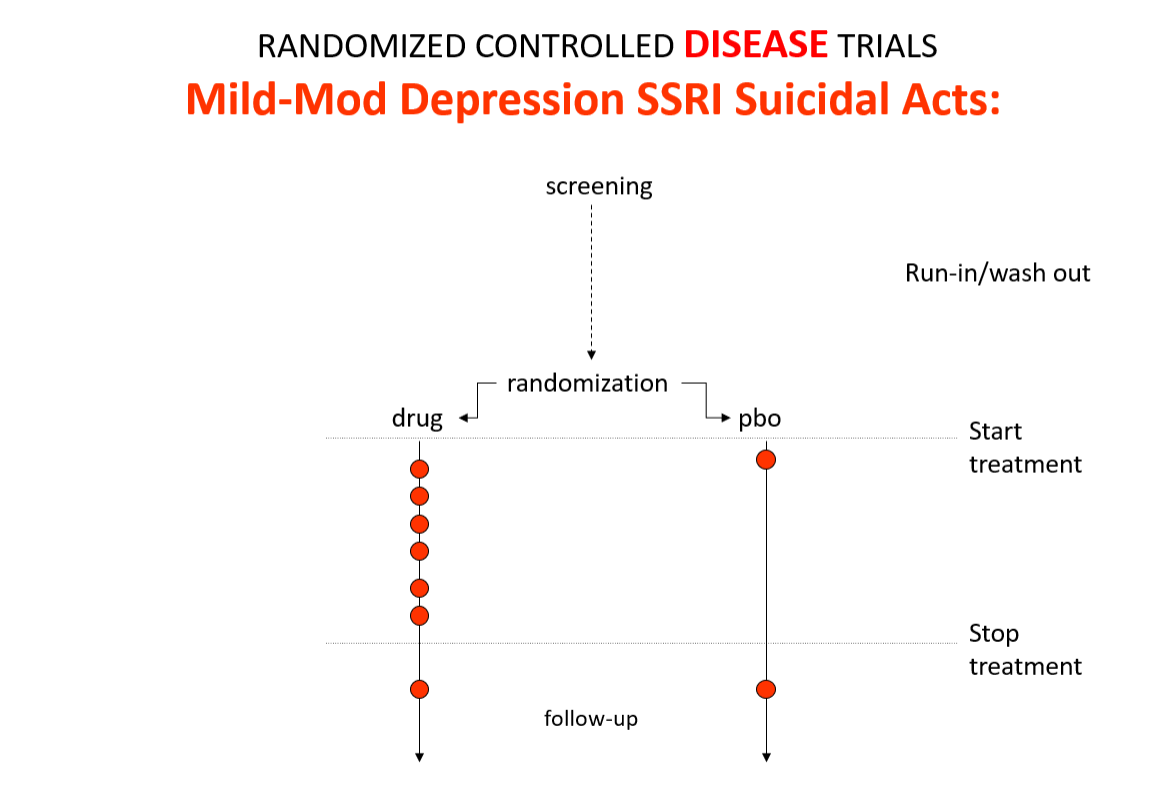
Slide 10: Here is the data on the trials in mild depression that brought the SSRIs to market – mild depression because SSRIs are no use in melancholia. You see an increase of suicidal events compared to placebo in people at little or no risk of suicide.
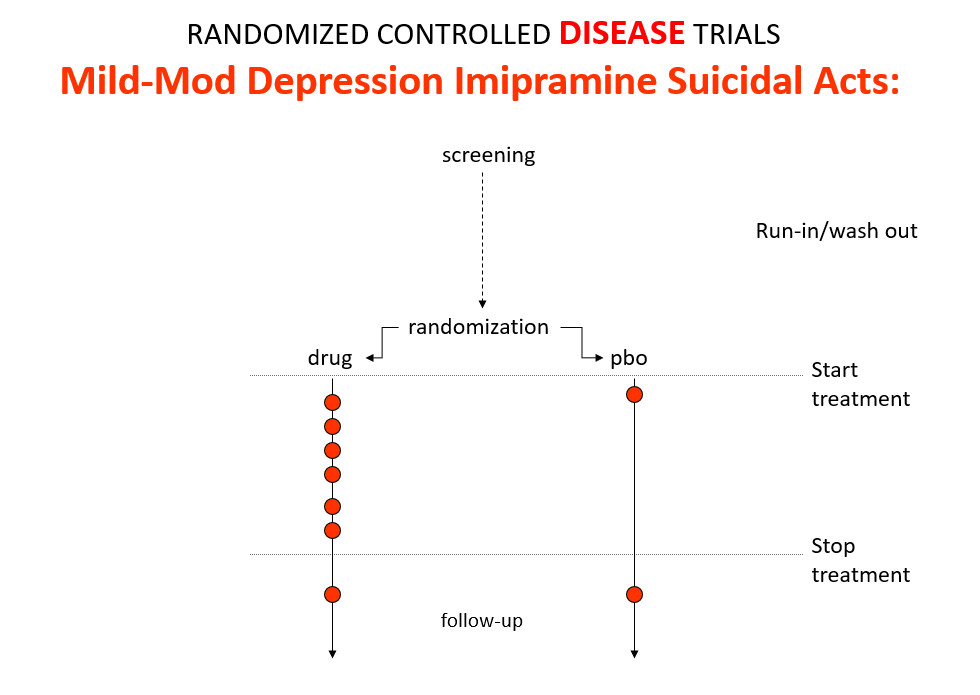
Slide 11: This is what the data for imipramine look like in the same mild depressions. This is not a thought experiment – it was used as a comparator in SSRI trials. Now it too causes suicides.
RCTs can give us diametrically opposite answers. This is because these are not Drug Trials. They are Treatment Trials and if the condition and treatment produce superficially similar effects, randomized trials cause confounding rather than solve it. This is true for most medical conditions and their treatments.
People evaluating drugs in traditional clinical trials, before RCTs, knew this. When a patient becomes suicidal in a trial you have to use your judgement to work out what is happening but in RCTs clinicians are not supposed to use their judgment. RCTs are more objective than our judgments – supposedly.
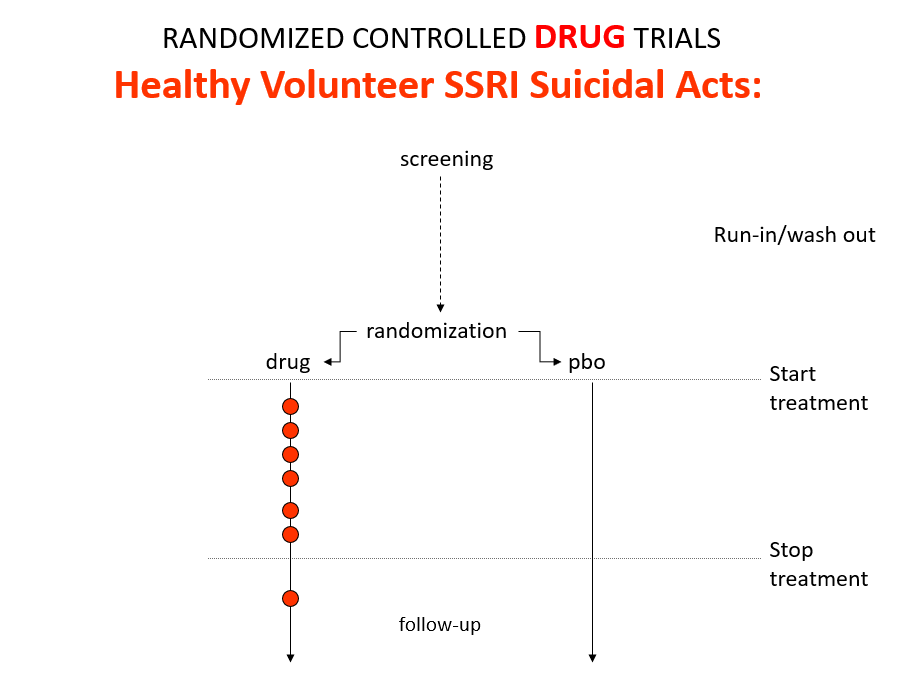
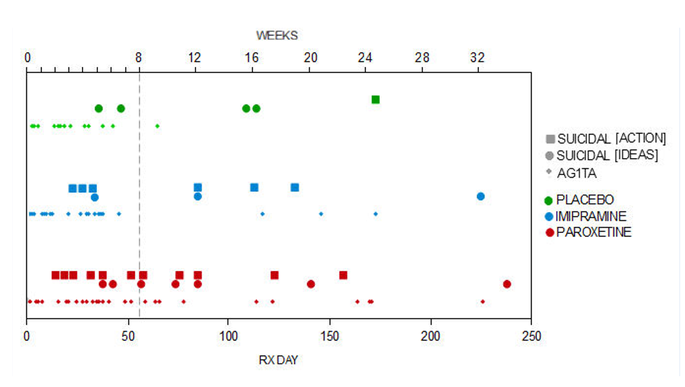
Slide 12: Here is what a Drug Trial looks like. In healthy volunteer studies in the 1980s, companies found SSRIs cause volunteers to become suicidal, dependent and sexually dysfunctional. We heard nothing about these problems when the drugs launched in part because Drug Trials enabled companies to engineer Treatment Trials to hide these problems.

Slide 13: If you break a limb and get recruited to an RCT randomly applying casts to one limb – not necessarily the broken one – the trial will show random application beats placebo. Practicing Evidence Based Medicine rather than Evident based Medicine here would clearly be crazy.

Slide 14: Here is a James Webb telescope image. James Webb is marvellously bringing out the infinite individuality of stars.
In addition to randomization, Fisher put a premium on Statistical Significance. By 1980 every leading medical statistician was saying we need to get rid of statistical significance in favor of Confidence Intervals.
Confidence Intervals had been introduced by Gauss around 1810. Because of measurement error, the telescopes in use often failed to establish whether there was one or two stars in a location. Measurement errors should distribute nornally and so constructing confidence intervals could help us distinguish individual stars.
We have moved a long way forward in this respect with the James Webb telescope you see here.

Slide 15: Confidence intervals rushed into medicine in the mid-1980s. All the authorities on the right – many linked to Boston – argued they were much more appropriate than significance testing. They are appropriate for measurement error but are they any more a cure for ignorance than statistical significance?
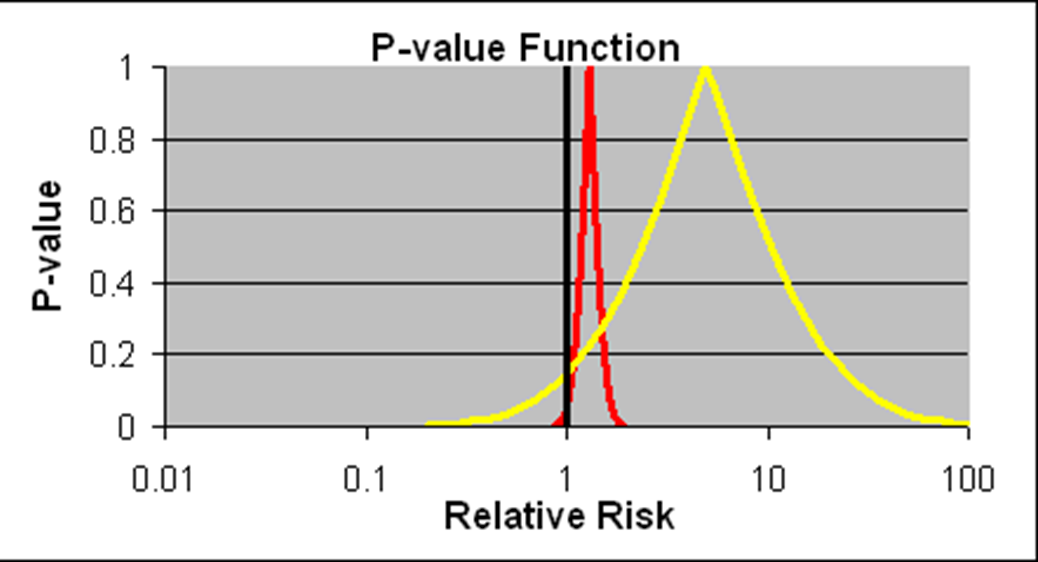
Slide 16: Confidence intervals we are told allow us to estimate the size of an effect and the precision with which it is known. We have much more precise details on the likelihood of the Red Drug here killing you than we have for the Yellow Drug. The best estimate of the lethal effect for the Yellow Drug however is greater. The standard view is that if we increase the size of the Yellow Drug Trial we will have greater precision and know better what the risks are. As we shall see, this is wrong.
As things stand, if you are asked to take one of these drugs, should you be guided by precision or effect size? Ian Hudson, FDA and WHO say the only dangerous drug here is the Red One. This is because more than 95% of the data, more than 19 out of 20 lie to the right of the line through 1.0 – confidence intervals have defaulted into statistical significance.
I would take the Red rather than the Yellow one. This is not measurement error and we don’t know what confidence intervals represent when they are not representing measurement error.
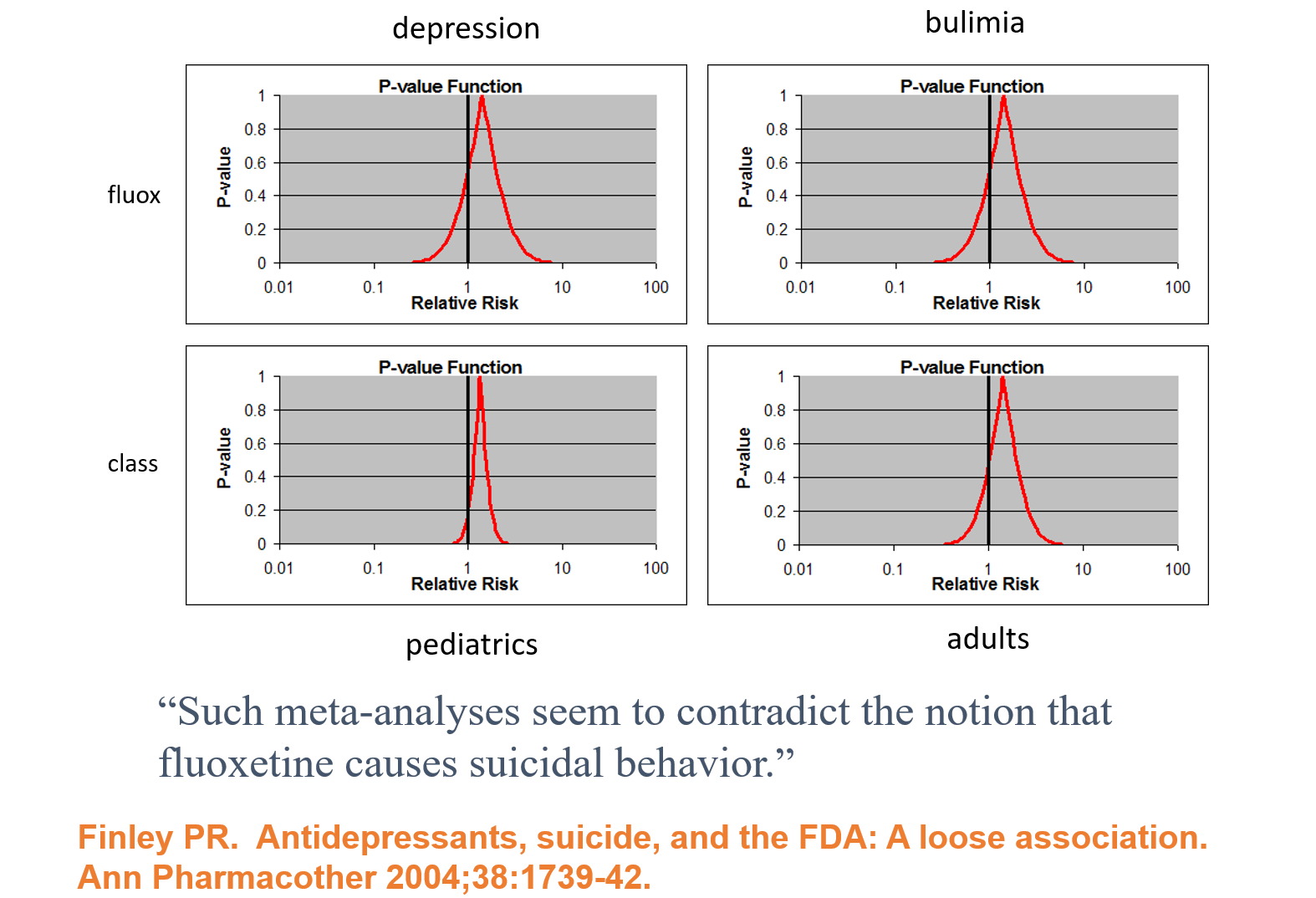
Slide 17: Faced with claims Prozac causes suicide, Lilly analysed their clinical trials and claimed there is no evidence their drug causes suicide. Confidence Intervals are being spun here as indicating we don’t know Prozac causes suicide as nothing is statistical significant. This is Ian Hudson thinking – at odds with all statistical expertise. It’s wrong. The consistency across young and old, depression and eating disorders strongly suggests in real life there is an excess of suicidal events.
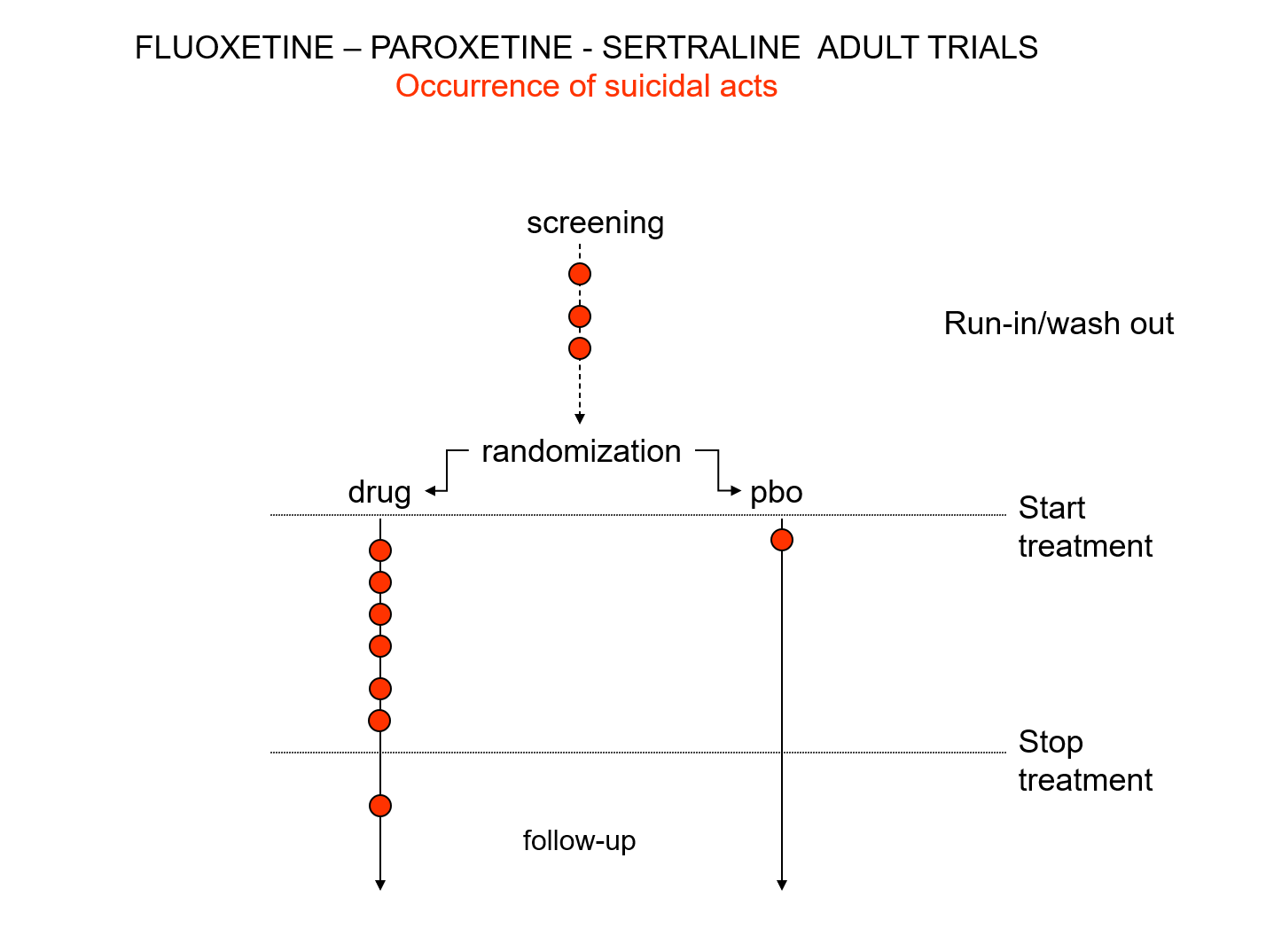
Slide 18: There is an intriguing mystery behind these figures. Here you see a representation of suicidal events that happened in the trials that brought Prozac, Paxil and Zoloft to market around 1990. You’ll note there are events under the word screening here. There is a 2 week washout period before a trial starts where people are whipped off their prior drugs before being put on the new treatment or placebo. This is a highly dangerous phase where people are in withdrawal and very likely to go on to a suicide attempt.
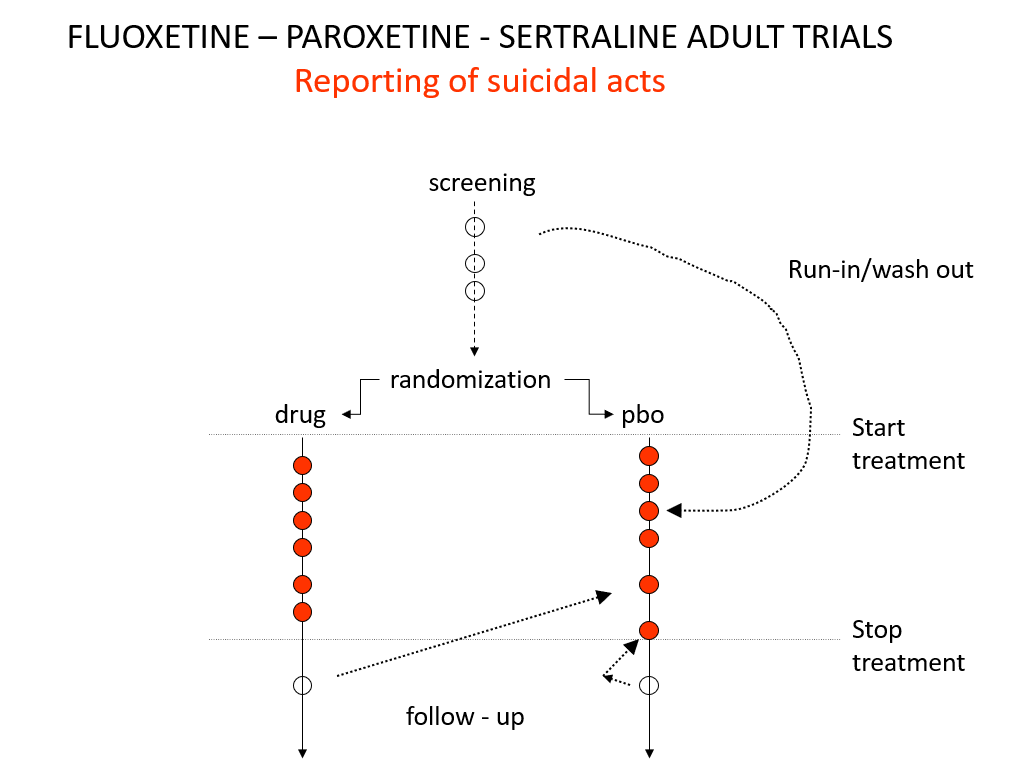
Slide 19: And here you see the moves companies made to avoid having a confidence interval excess of suicidal events on treatment. Companies only moved the events – not the people.
These moves were justified on the basis that people in the run in phase were not on active treatment – which is equivalent to being on placebo – but they often were withdrawing from active treatment which is highly dangerous. Some who stopped treatment at the end of the active phase of the trial committed suicide and were designated placebo too. Some on placebo, put on active treatment in the follow up period, committed suicide and were designated as placebo suicides on an intention to treat basis.
There are two articles from 2006 that bring out this point Did Regulators Fail and The Antidepressant Tale: Figures Signifying Nothing. The Antidepressant Tale gives other examples of confidence interval abuse.
After all these maneuvers, there was still an excess of suicidal events on these SSRIs but the confidence interval was no longer entirely to the right of 1.0. Confidence intervals have degenerated into statistical significance tests because regulators need a Stop-Go mechanism and statistical significance provides this. But doctors don’t need an external Stop-Go mechanism to replace their clinical judgement, so why do they go along with this?
Slide 20: Nobody noticed these maneuvers around 1990, but fourteen years in a crisis about children becoming suicidal on antidepressants, questions began to be asked. GSK and Pfizer responded:.
‘GSK did not intentionally submit any erroneous or misleading information to FDA. The suicide data submitted to FDA explicitly identified when events occurred during the placebo run-in period. FDA had all this information right from the beginning.’
“Pfizer’s 1990 report to FDA plainly shows … that 3 placebo attempts as having occurred during single blind placebo phases… FDA has neither criticized these data or the report as inappropriate, nor required additional analyses”.
These maneuvers breach FDA regulations and FDA staff noted this in memo’s at the time. But not only did FDA ignore these breaches of regulations senior figures, like Tom Laughren, put their name to articles that embraced these breaches of regulation – in one case in the cause of showing it was not unethical to have placebo controls in RCTs, as those on placebo were not at any greater risk than those on treatment.
There was much back and forth between FDA and companies in 1990. Was it criminal? Perhaps. I prefer the idea of strategic ignorance.
What I think we are seeing are events circling around a major crisis in knowledge production. This is not something you can expect FDA to take a lead on – they are not political actors, they are bureaucrats. Companies create knowledge or were creating the appearances of knowledge at this point, but doctors are surely primarily responsible for the creation of medical knowledge and doctors were missing in action around 1991– other than as spokespeople for companies.
Slide 21: The Sacred Mantra is that randomization controls for all possible confounders in all possible universes. The reality is randomization introduces confounders into clinical trials.
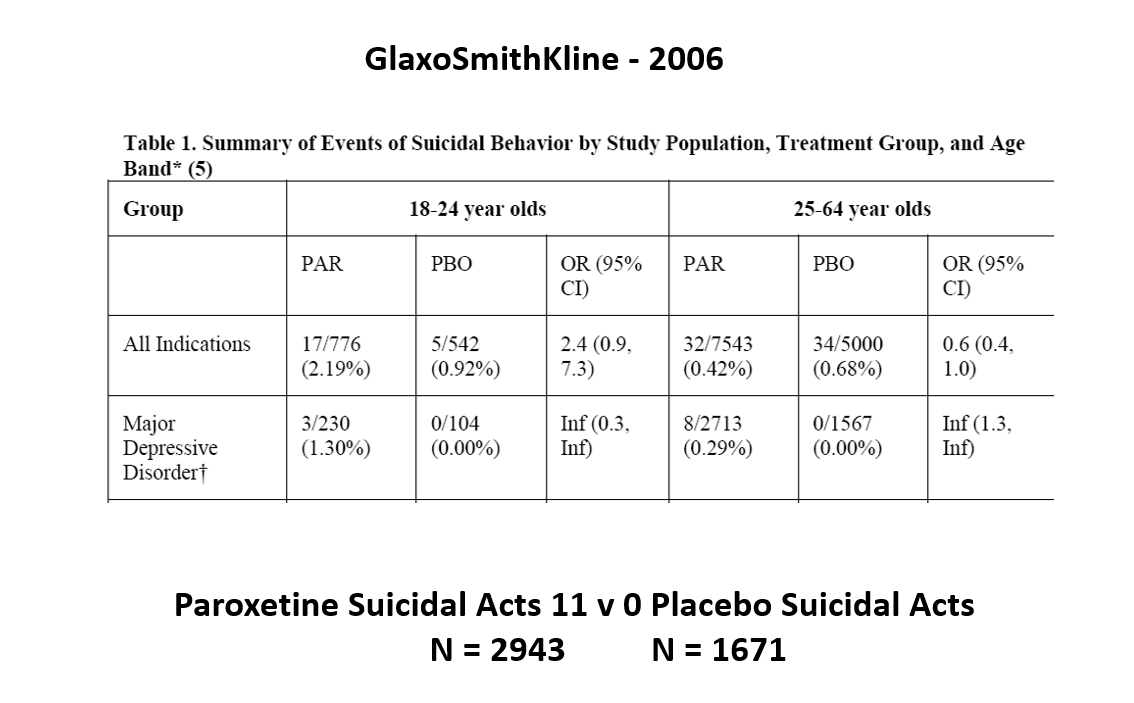
The images for the next 3 slides come from a GSK paper prepared in 2006 for submission to FDA. The small print is hard to read – the bold at the bottom gives you the key details.
The data for suicidal events on Paxil in Major Depressive Disorder trials in this first slide show it causes suicidal events. Even Ian Hudson would have to agree and these data were available at the time of the Tobin trials. But randomization is about to come to GSK’s rescue.

Slide 22: Faced with a problem like this, had GSK consulted me I’d have said do a trial in Intermittent Brief Depressive Disorders (IBDD). They might have said but there are trials of SSRIs in IBDD and they don’t work. I’d have said do one. They did and it had to be terminated early, Paxil did so poorly. I’d have said do another. Why – the figures for Paxil still look bad in this group?
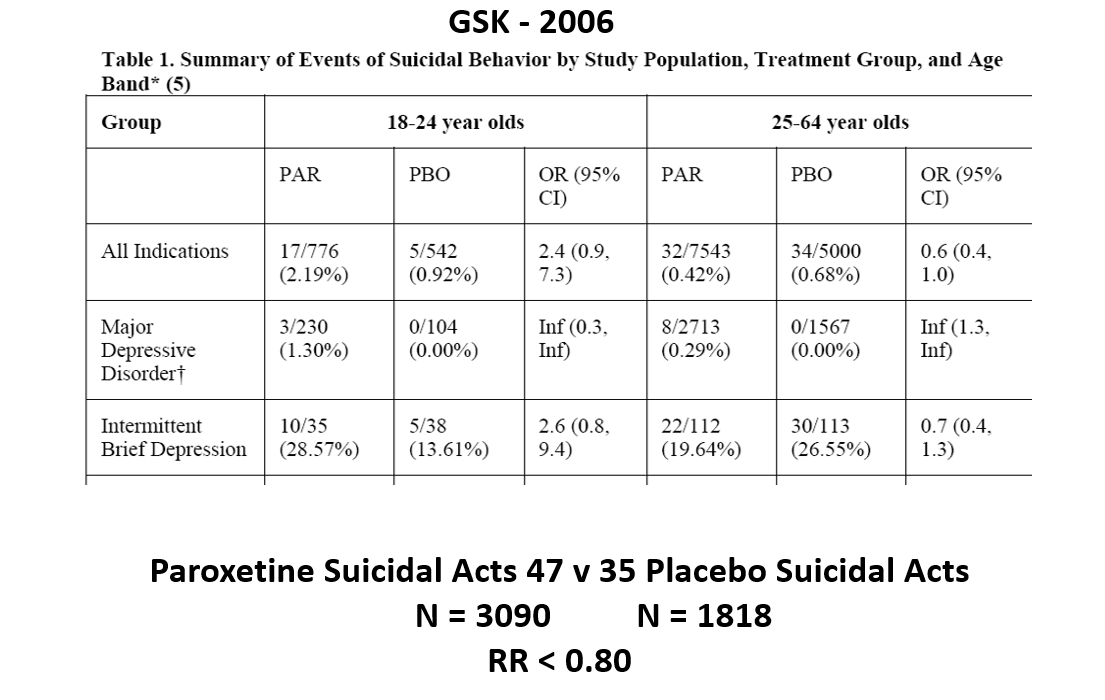
Slide 23: But when you add the IBDD data to the MDD data, all of a sudden the figures say Paxil protects against suicidal events.
This scenario can happen every time a condition we are treating is heterogenous – that is dementia, diabetes, parkinson’s disease, breast cancer, back pain, hypertension – pretty well everything in medicine. In these cases randomization will act to hide effects good and bad and leave us able to use a problem a drug causes to hide a problem a drug causes.

Slide 24: Graphically this is what it looks like. The Red Drug here is the MDD curve alone – more than 95% of the data are to the right of the 1.0 line. The traditional wisdom is that adding some more events to the Red Drug above should give us a more precise version of the same estimate
In fact when you add a few more people, about 3%, we have shifted the curve to the opposite side of the 1.0 line. Its far a more precise confidence interval but this is a precision that speaks to our ignorance rather than to better knowledge. No medical statistics book ever hints at this possibility.
We could add 40 suicidal events to the paroxetine IBDD arm before Ian Hudson would have to admit paroxetine causes a problem – on the basis that the results are now statistically significant.
IBDD patients could be admitted to MDD trials – we have no way to distinguish them. Some patients become IBDD by virtue of a poor response to an SSRI.
Randomization in heterogenous conditions will hide effects drugs cause. It allows us to use an adverse effect a drug causes to hide the same adverse effect that drug causes. Confidence intervals do not help us work out what is going on in these cases.
Nor do they help in heterogenous drug responses. Lets take 20 Aarons who are all sedated by a Red Drug and 20 Davids all stimulated by it. The best estimate in the confidence interval in this case will lie on the 1.0 line, showing the drug has no effect. A method to distinguish between one and two stars should not produce an answer that there are no stars here. Algorithmic judgements cannot substitute for a human judgement.
Slide 25: Here is another problem with Confidence Intervals. Young men take Finasteride to restore a thick head of hair. We could count hairs and build confidence intervals around before and after hair follicle numbers.
Finasteride also causes suicide and permanent sexual dysfunction and like most drugs has 3,500 other effects. Confidence intervals for hair numbers before and after is one thing, but applying them to suicidality or sexual function, which were not measured in the trial, and for Merck to then claim on this basis that the science does not support a link between finasteride and suicide on the basis that not all the data lie to the right of the 1.0 line isn’t managing measurement error. It’s a confidence trick – that happens all the time.

Slide 26: There are more dead bodies on antidepressants in trials than on placebo, yet the RCTs as Ian Hudson told you show the drugs work. This is because most RCTs have a surrogate outcome. For antidepressants its the Hamilton Rating Scale for Depression.
Fifteen years after its creation, Max Hamilton commented on his scale:
It may be that we are witnessing a change as revolutionary as was the introduction of standardization and mass production in manufacture. Both have their positive and negative sides
Hamilton saw this scale as a checklist of things to ask about in an interview – a mixed blessing.
Slide 27: Checklists are now viewed as more scientific than David Healy in a clinic asking you about your family. They will produce standardized but possibly disastrous interviews.
For instance, on this scale, there is a suicide item. Suicidality can stem from the illness or the drug. This needs a judgement call. If caused by the drug you should rate a Zero. If caused by the illness you might rate 3 or 4. If you just check yes for suicidality, the default is to the illness. Ditto for sex, and for sleep.
In the case of sleep, the illness can produce too much sleep or not enough sleep and each of the medicines can inhibit sleep or heavily sedate. There are 3 sleep questions. A scientific interview has a multitude of options requiring judgement calls.
In the 1980s, we brought problems to doctors needing help to get on with the lives we wanted to live. Since then, for drug companies, rating scales, sometimes left in the waiting room, ensure you do an interview that produces figures for which a company drug might seem an answer. Your interview will help you to help your patient to live the life Pfizer want him to live. Do that and you are no longer practicing medicine.
Slide 28: Many think RCTs are fine if only they were done by angels.
Study 329 was conducted in the very best university centres in North America. It has an authorship line to die for, starting with Marty Keller and including a Canadian Liberal Party Senator – Stan Kutcher. It was published in the Journal with the highest impact factor in child psychiatry. The article claims Paxil works wonderfully well and is safe for depressed teens.
What I am about to tell you applies to all industry trials across medicine.
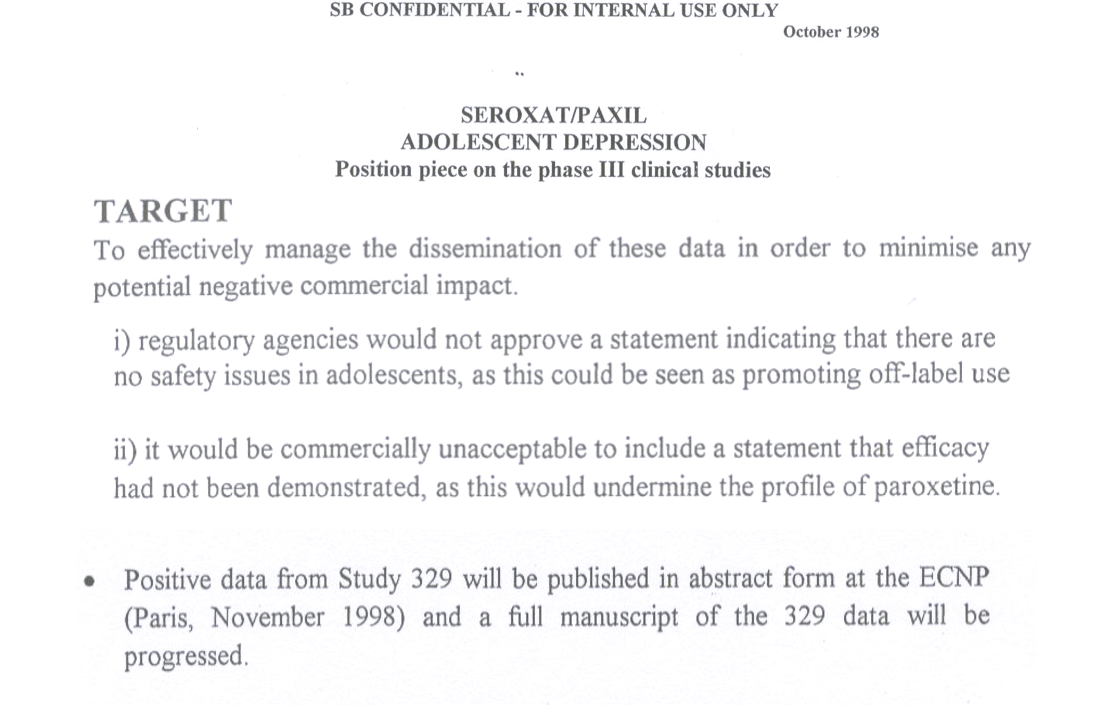
Slide 29: Three years earlier, in 1998, GSK concluded Paxil didn’t work in Study 329 and was not safe. That could not be published so they were going to pick out the good bits of the data and publish them. The good bits formed the Keller et al 2001 paper.
This 1998 internal SKB document led New York’s Attorney General to file a fraud action against GSK. As part of the resolution of this, GSK agreed to make their Paxil trial data public. A decade later, GSK resolved a Dept of Justice action, which also involved Study 329, for $3 Billion dollars.
Slide 30: These actions gave a team of us an incentive to Restore Study 329 and we now had more raw data from this study than FDA or other regulators had seen for this or any company study.
Slide 31: In contrast to Keller, we found the 8-week acute phase showed no difference between Paxil or placebo. We found the same for the never published 6 month continuation phase – never published till we published it 18 years after the trial ended.
Slide 32: Keller noted 6 emotionally labile events in the trial, some of which might have been suicidality, 4 on paroxetine. But in our hands a fifth of the children on Paxil had a behavioral event mostly suicidality – 18 out of 93 children.
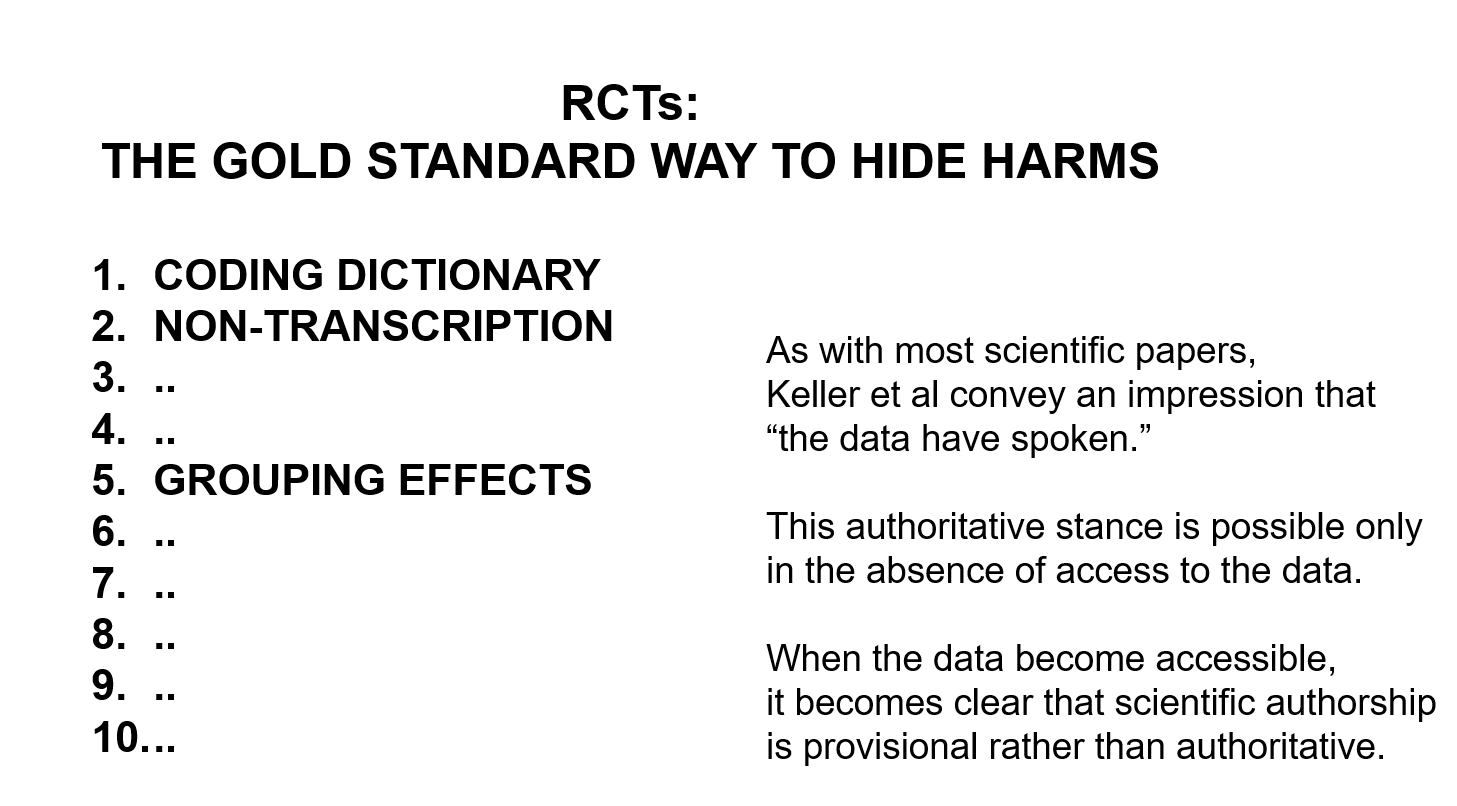
Suicide is not what I want to focus on. It’s the ability of company studies to hide adverse events. Our paper lists 10 ways to hide things. Coding – as in calling suicidality emotional lability, is top of this list – this is the first act of authorship but no reviewer or journal pays any heed to it.

Slide 33: In a Pfizer trial, at the same time, a man on active drug got agitated, poured gasoline/petrol on himself and set fire to it intending to kill himself but he only died from his burns 5 days later. Pfizer coded him as death by burns. Once the coding is done, the paper is all but written.
There is some chance FDA found out about this man because if you have to go to hospital or you die companies had to file a report outlining what happened and did so for this man.

Slide 34: But in Study 329, FDA know nothing about a 15 year old boy, 2 weeks after being put on Paxil, who was out on the street waving a gun, threatening to kill people. He was brought to hospital by the police. There was no report to tell FDA what happened. Thirty years ago companies found a way to legally avoid filing these reports. Companies are still using this trick in trials published this year in all major journals and regulators either don’t spot or are not bothered to close a very obvious loophole. In Study 329, 4 children vanished through this loophole.
Slide 35: The sentences on the right are the 3 sentences with which this article ends – the message is companies have created an impression that RCT articles are like tablets of stone brought down from the mountain top, commanding doctors to prescribe and us to take. But when we have access to RCT data, this raises questions – as science should – rather than issues commands.
In addition to Coding, Grouping is also an act of authorship. If you have 500 events in 93 children on Paxil, rather than list them all, cardiac events are usually grouped in a Cardiac group etc. Behavioral events are usually grouped in a Psychiatric group. GSK grouped all behavioral events under Neurological. This groups emotional lability with headaches and dizziness, which are very common. Grouped this way the behavior problems disappear. Grouped as Psychiatric, the problem is immediately clear.
The Restoring Study 329 article took over a year to get it published. What was fascinating was the BMJ did not contest the data but they were very exercised by the act of interpretation. They appeared to assume that the data had spoken and GSK faithfully transmitted what they had heard. They found it heard to grasp that GSK used a coding dictionary that even FDA had never heard of.
Any scientific analysis inevitably involves an act of authorship or interpretation. But BMJ found it hard to let us author the behavioral events out of the neurological group into a Psychiatry group. There is no such thing as data without an interpretation. Ideally the interpretation should command consensus but for BMJ this appeared to mean that we should adopt what GSK had done without question.
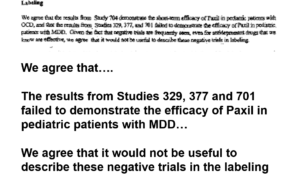
Slide 36: Everyone knows Prozac was approved for children who are depressed but not that Paxil was too. A year after the Keller paper came out, this is part of an FDA approvable letter for Paxil.
It says GSK have told FDA Study 329 is negative. FDA agree its negative – in fact all 3 trials are negative – but FDA will still approve Paxil for kids. FDA also agree with GSK’s suggestion not to mention the negative trials in the label of the drug. Why would FDA agree to this?
Before answering that, let me note FDA also viewed the Prozac trials in teens as negative.
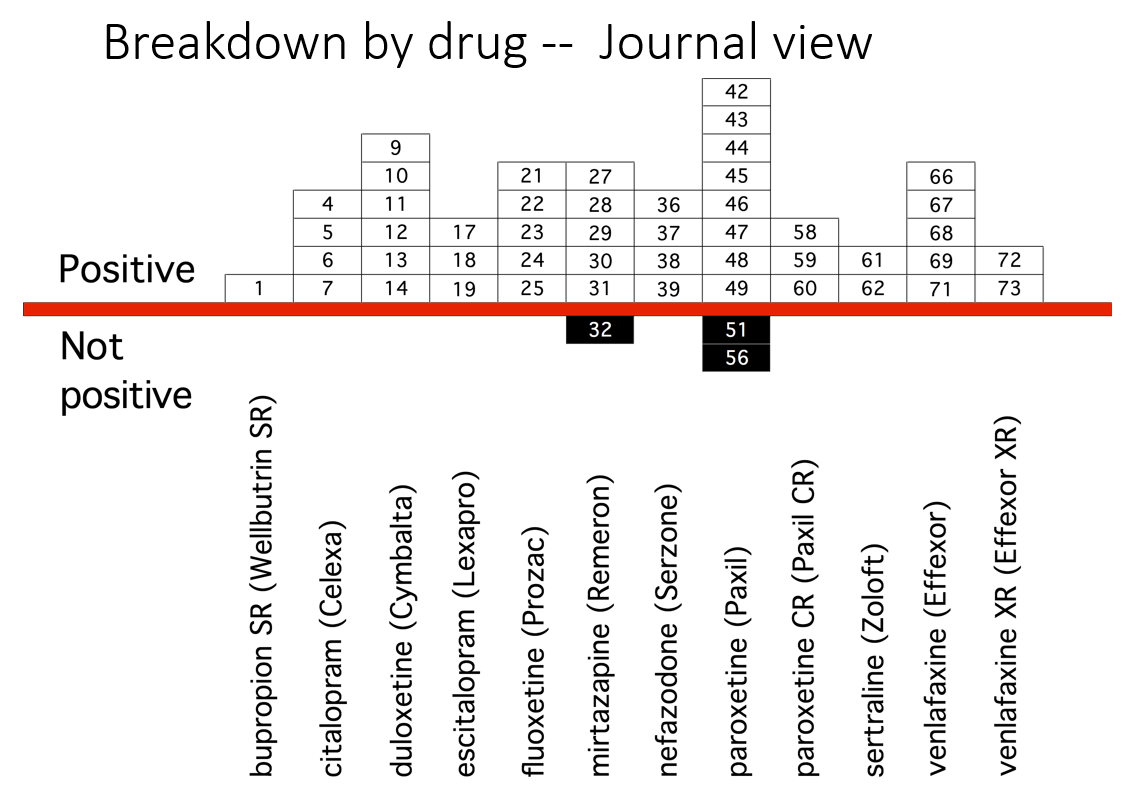
Slide 37: This slide from Erick Turner’s 2008 article shows published adult ‘trials’ on various antidepressants, almost all indicating the drugs work well and are safe. Look at the sertraline column – 3 from the right. It shows two studies – the minimum needed for approval.
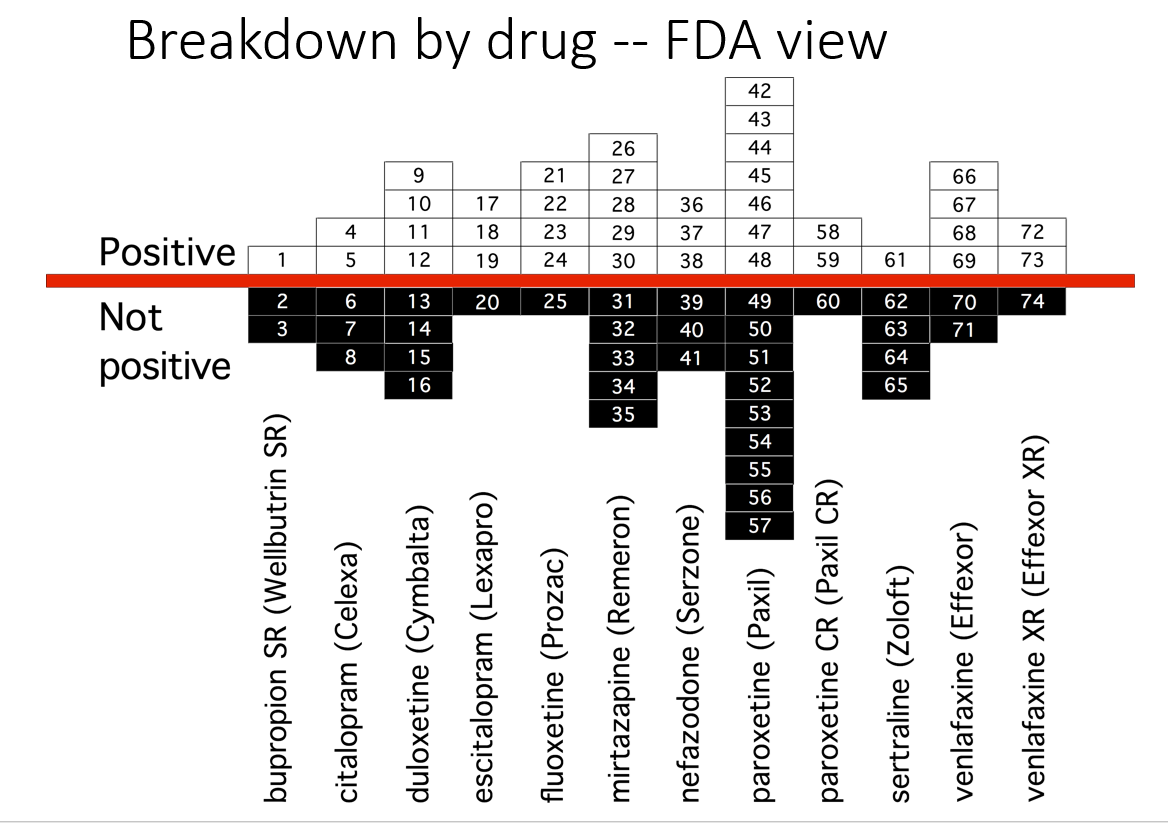
Slide 38: Another slide shows the trials as FDA viewed them. 46% of these trials are negative. Many published as positive were negative to add to the unpublished negative trials. Look at the sertraline column – only one positive study.
Why do FDA say nothing about this? Well if FDA said trials are negative – the companies might get sued for fraud or fined – as happened for Study 329.

Slide 39: Here you see the PTSD page of a 30 page document listing Zoloft articles in progress. These papers aim at capturing markets not at informing us on how to use Zoloft safely.
Pfizer did 4 Zoloft PTSD trials. All negative. FDA approved it on the basis of 2 trials with a minimal benefit for women. These good bits plucked out are what’s being published. You see under Status on the right two articles are complete and will be sent to the very best journals. On the left you see TBD – to be determined – when Pfizer decide which names would sell most Zoloft.
You saw a 24 person authorship line for Study 329 but the real author is not there. Across medicine studies of on-patent drugs are ghostwritten.
In the case of children’s antidepressant trials the entire literature was written by ghosts and there is a complete mismatch between the published claims and the data – the greatest mismatch in all of science. On the basis of published claims the use of these drugs is escalating rapidly in teenagers with predictably bad results.
Slide 40: Fifty years ago, Britain joined the EU and ran into trouble. Cadbury’s chocolate, their favorite chocolate, they were told, could not be called chocolate. It didn’t have the right quota of cocoa solids. British consternation over chocolate led to Brexit some decades later.
What FDA do is in their name – they regulate Food and Drugs. Faced with butter or chocolate or drugs, companies must meet an assay standard – so much cocoa solids, animal fats, or so many points on a Depression rating scale in 2 trials. Meet that and FDA let you use the words chocolate, butter, or antidepressant. It’s not FDA’s job to decide if this is good butter, or if chocolate is good for you, or to police the medical literature.
Sllide 41: Since 1990, however, regulators increasingly say they approve drugs on the back of a supposed positive Benefit-Risk ratio. This is Ian Hudson thinking. If there are no proven adverse effects and just a benefit then of course there is a positive Benefit-Risk ratio.
The medical act of bringing good out of the use of a poison is incompatible with all this.
We would all agree there is a positive benefit-risk ratio for parachute approval in terms of lives saved versus lives lost – even though some men might have difficulties making love in the weeks afterwards, owing to harness effects. If things aren’t clear enough for us all to endorse, regulators are de facto getting us to live the lives companies want us to live when they make Benefit-Risk claims.
Unlike parachutes, SSRI RCTs have more dead bodies on SSRIs than placebo. In addition. the commonest effect of an SSRI is to cause genital numbness in close to everyone who takes one within 30 minutes of a first tablet. Almost everyone will have the way they make love changed while on an SSRI and they may later find themselves unable to make love ever again, either because they can’t stop or because the drugs can wipe out sexual function for ever. This may be far more important to a person than any mood benefit.
But the focus on the mood effect, means the sexual effect was missed entirely in the trials regulators scrutinized both because that’s how trials work but also with a little extra gaming from companies.
Some years ago treating a man with OCD, I tried an SSRI – the first line treatment and then more heavy duty drugs when the SSRI didn’t work. All made him worse. One day he came in much better – he had stopped all his drugs but he was cured by going back smoking. He had also googled nicotine and OCD and found studies showing nicotine and related drugs can help OCD.
When I say the Art of Medicine lies in Bringing Good out of the Use of a Poison, people hiss at me but everyone would likely agree this man was bringing good out of the use of a poison. SSRIs however are prescription-only because we expect them to be more dangerous than over the counter alcohol and nicotine.
The important thing is that this man (perhaps with input from me) is the only person in a position to make a meaningful Benefit Risk call. I can’t see what role FDA could have in this. Benefit-Risk calls are an individual matter. Making the claims FDA now make puts them in a role of getting people to live the life Pfizer want them to live.
Am I making all claims on the basis of Citizen Research more than Expert input? No – among the articles this man found about nicotine and OCD was one whose significance passed him by. One of the authors was Arvid Carlsson, who created SSRIs and won a Nobel Prize for Medicine.
But when you have Skin in the Game, Motivation can be worth just as much as Expertise.

Slide 42: As a result of Ian Hudson’s views, as I wrote 25 years ago, everyone who participates in a company trial today puts all the rest of us in a state of Legal Jeopardy. We should boycott trials, until this changes. See Clinical Trials and Legal Jeopardy.
Slide 43: That article was 25 years ago, this is 25 days ago and argues everyone entering a trial now are deceived by consent forms that promise coverage for injuries, unaware that there are no injuries on modern treatment, or no injuries that can be admitted. See The Coverage of Medical Injuries in Compary Trial Informed Consent Forms.
Slide 44: However, since 2010, the US Supreme Court in the Matrixx case made it clear that Ian Hudson’s views do not apply to investors wanting to make up their mind about the Benefits and Risks of investing. We who are investing our lives in these treatments still do not have such rights.
Slide 45: The beating Tell Tale Heart of this talk came with the publication of this article 33 years ago this month, in which 3 Boston clinicians claimed fluoxetine caused 6 people to become suicidal. Analyzing the cases closely and following traditional clinical approaches for determining causality, this article nailed beyond doubt that fluoxetine could cause some people to become suicidal.
Lots of other groups reported similar findings. I published 2 cases of men, who were challenged, dechallenged and rechallenged with an SSRI. There was no other way to explain what happened them except that fluoxetine had caused it. This was Evident Based Medicine .
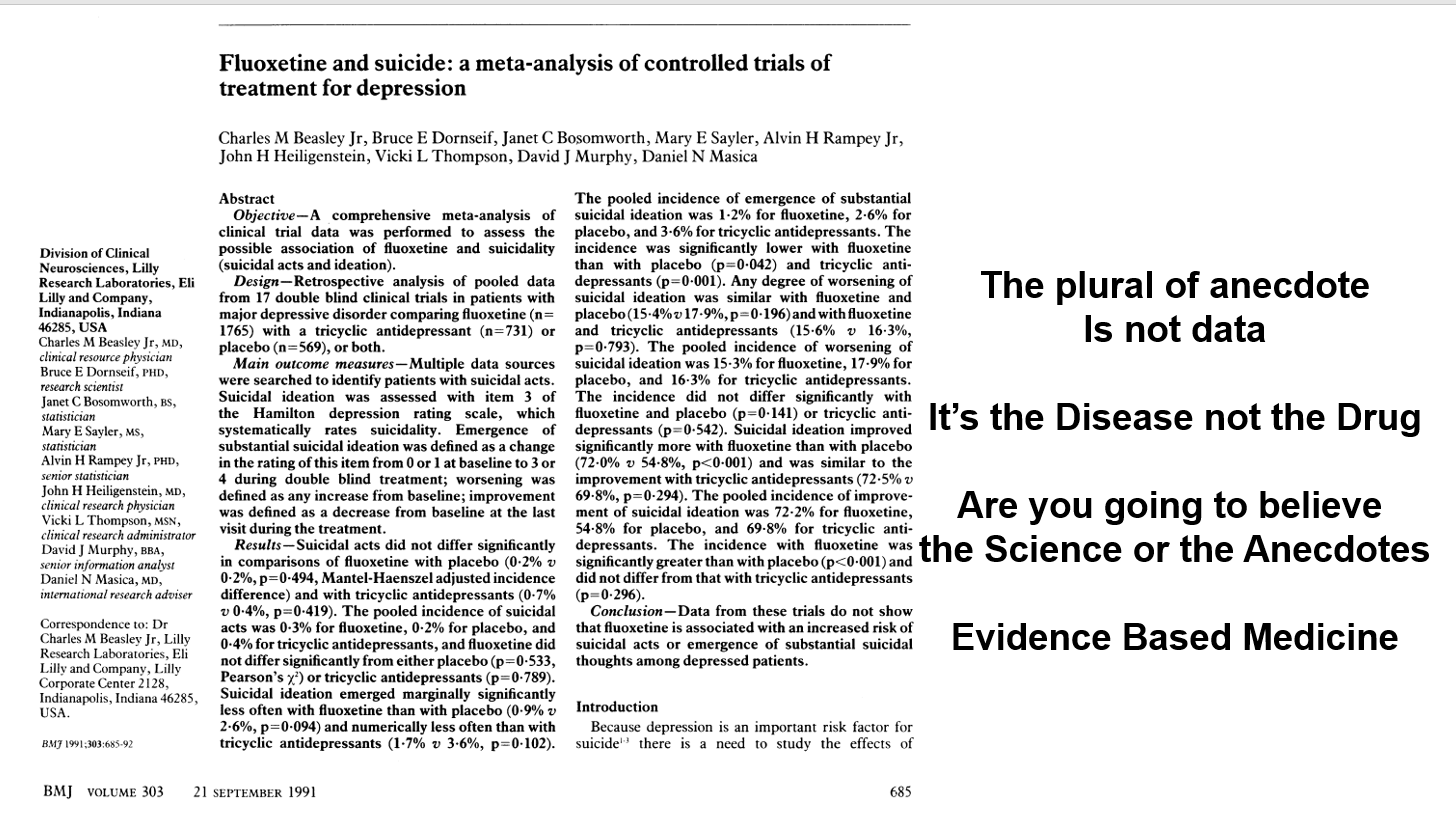
Slide 46: Almost the same week as my article came out, BMJ published an article in which Lilly claimed an analysis of their clinical trials showed no evidence fluoxetine made people suicidal. The cases being reported, therefore, were sad but anecdotal – and the plural of anecdote is not data. Depression was the problem not fluoxetine. Clinical trials are the science of cause and effect. Doctors, the public, media, and politicians were being asked – are you going to believe the science or the anecdotes?
This was a knowledge creation moment that likely had input from all companies and perhaps FDA. This article created Evidence Based Medicine and just as with RCTs 30 years earlier, the people most commonly exhorting doctors to practice EBM today are Pharma companies.
In fact, the original phrase is the plural of anecdotes is data – otherwise Google wouldn’t work.
The idea the disease is responsible for suicide attempts and suicides in healthy volunteers is hard to believe but companies can wheel out experts to say just that.
My key point is that the Teicher paper is the science – the Lilly data is an artefact. My challenge to you is which are you going to believe the Science or the Artefact?
The Science of Medicine lies in making hard judgement calls. The made by algorithm approach, combined with inappropriate statistics, creates artefacts not science.
You’ve seen earlier how Lilly cooked the books. When you get the trial data, the Evident Based Medicine and Evidence Based Medicine approaches here can be reconciled – as you might expect with real science.
But even there was an incompatability there isn’t a problem. Resolving discrepancies is how we do science.
This points to a deep problems with Lilly’s argument. They are not in the business of being scientific – resolving discrepant observations. Lilly’s argument is a religious one – a dogmatic one – they forbid us to believe the evidence of our own senses.
This is papal infallibility riding again.
Peter Drucker, the doyen of marketing gave us a secular update – the goal of marketing is not to increase the sales of Prozac, its to own the market. This was the moment Pharma took ownership of the market.
This ownership allows companies to dictate what the risks, the benefits and the trade-offs of drugs are. Allows them to force us to live the lives they want us to live rather than engage with the risky and unprofitable business of producing products that will help us to live the lives we want to live. Following this Artefact is profoundly alienating.
Slide 47: This faces us with a what is science question? The usual histories start with the foundation of The Royal Society in 1660, which established the ground rules for Science. Science would deal with matters that could be Settled by Data. Participants could be Xtian, Hindu, Jew, Muslim, or Atheist, but participants were called on to leave these badges at the door and make a consensus based judgement call about the best way to explain the experimental outcome in front of them.
The histories of science emphasize the word Data. Settled is the more important word. Statistics played no part in this science. The experiments were events and didn’t need the descriptions statistics can provide. Science was emphatically not about replacing judgment calls with a statistical artefact. It only became so 33 years ago.

Slide 48: This account of our history overlooks an earlier event. In 1618, Walter Raleigh was executed – for being too close to those pesky Europeans. Raleigh was convicted on the basis of things said about him by people who did not come into court to be cross-examined.
Legal systems worldwide recognized the injustice of this and introduced Rules of Evidence. Hearsay could not be used as evidence. Jurors – a group of 12 people, Xtians, Hindus, Muslims, Atheists and Jews, can only base a verdict on material put in front of them that can be examined and cross-examined. The process of forcing 12 people with very different biases to come to a Verdict about what is in front of them is the essence of science.
Verdicts and diagnoses are provisional – the view that best fits the current facts. This might appear to contrast with the objectivity of science, but scientific views are similarly provisional. Scientists attempt to overturn verdicts with new data.
Let’s say I gave Aaron fluoxetine 33 years ago and he became suicidal. I could examine and cross-examine him, run labs and scans, raise the dose, stop the drug, add an antidote, check with colleagues has anyone else seen anything like this or can they explain it in any other way. Aaron is the data – all of the data. He is the apparatus in which the experiment is taking place.
If Aaron and I conclude fluoxetine made him suicidal and report this to FDA, the first thing FDA does is to remove his name. No-one can now examine or cross-examine him and come to a scientific view about whether there is a link or not. His injury has been made Hearsay – indeed misinformation.
If you are later injured in the same way and see tens of thousands of reports of suicidality on SSRIs on FDA’s adverse event reporting system, you cannot bring this into court because no-one can be brought into court. It’s Hearsay not Evidence.
Company RCTs are equally hearsay and should not be let into Court as evidence. Accessing the data in this case means accessing people – like Aaron or me – and we cannot do that with the people in company trials, who often don’t exist. Except rarely, the authors on the articles have seen none of these people and cannot speak to what happened either.
In contrast, if Aaron and I report his case in he New England Journal or the American Journal of Psychiatry as a Case Report, with our names on it, we can both be brought into Court.
Slide 49: By 1983 the view was emerging that RCTs offered the scientific and sophisticated way to establish if a drug had adverse effects as this quote by Rossi et al indicates:
Spontaneous reporting is “the least sophisticated and scientifically rigorous . . . method of detecting new adverse drug reactions.
A mid-career Lasagna, the man who more than anyone introduced RCTs, responded:
This may be true in the dictionary sense of sophisticated meaning ‘adulterated’ . . . but I submit spontaneous reporting is more ‘worldly-wise, knowing, subtle and intellectually appealing’ than grandiose, expensive RCTs.
Slide 50: Here you have an older Louis Lasagna saying:
In contrast to my role in the 1950s which was trying to convince people to do controlled trials, now I find myself telling people that it’s not the only way to truth.
Evidence Based Medicine has become synonymous with RCTs even though such trials invariably fail to tell the physician what he or she wants to know which is, which drug is best for Mr Jones or Ms Smith – not what happens to a non-existent average person.

Slide 51: Here is James Webb again to remind you that confidence intervals were a step on the way to revealing the individuality of stars. In medicine, statistical approaches operate against individuality.
Using Chance to control Bias does not foster clinical science, especially when we allow a mindless algorithm to replace clinical judgement. Clinical medicine, like law, and the first 300 years of science uses Bias to Control Chance and both medicine and law need to assert the validity of this approach.
Slide 52: Using Bias to control Chance rather than some algorithmic method of controlling Chance is critical when numbers enter the frame. This is our only defense against medical neo-liberalism.
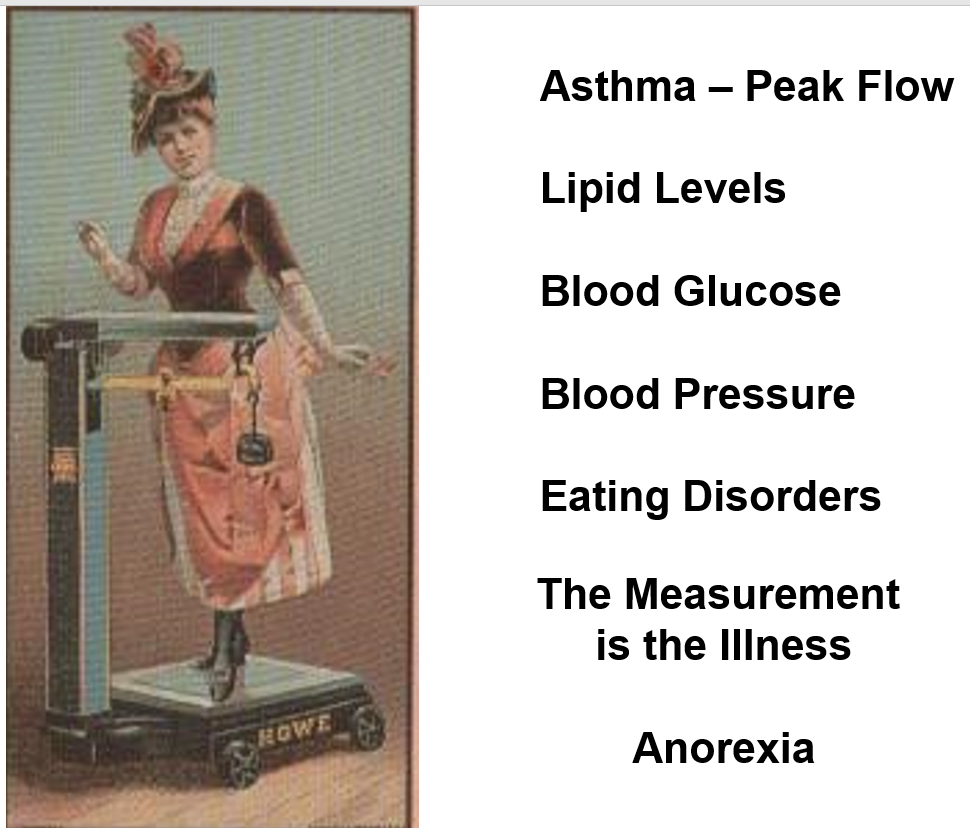
Around 1980 Pharma began treating healthy people. They discovered that numbers for our peak flow rates, bone densities, blood pressure, lipids, or sugar provided opportunities to sell drugs. Up to 1980, we brought our problems to healthcare – seeking help to live the lives we wanted to live. After that health services began to give us problems and the amount of medicines consumed rose dramatically. We began treating numbers rather than people.
Remaining on top of data like this is difficult. Just after weighing scales for people were introduced in the 1860s, we got the first descriptions of anorexia nervosa. In the 1920s, weighing scales in drug stores came with norms for our ideal weight given our height and sex and eating disorders mushroomed. When scales migrated into our homes in the 1960s eating disorders became epidemic – in the countries that had weighing scales. Measurements can make both us and our doctors neurotic.

Slide 53: There is an extra element to the equation. The service industries emerged in the 1950s. Through to 1980, no-one viewed health as a service industry – doctors were professionals who exercised judgement the way a Judge might. But service industries have managers and health got managers. With this the exercise of clinical discretion, the jewel in the crown of Health Care became a problem for those who manage services.
The idea of bringing good out of the use of a poison does not compute for managers, insurers, politicians or increasingly the public.
Before 1980, clinicians mobilized the resources of the organization they worked to handle the risks your condition posed to you. Now instead you can palpably feel the clinicians you meet are managing the risks you pose to the organization we work for.
Slide 54: Managers manage what they can measure. For them figures have a sheen of scientific gold. We are re-running the King Midas story – this gold coating is incompatible with Human Care and Life.
This governance by numbers is the essence of the neoliberalism that began in Chile and Britain – treat the money supply numbers or inflation numbers regardless of what is happening a country. Medicine is the best place to see this and its deleterious effects in action – aggravated by the fact that bowing down before a golden algorithmic idol inhibits anyone from leading us out of this desert in which we now wander.
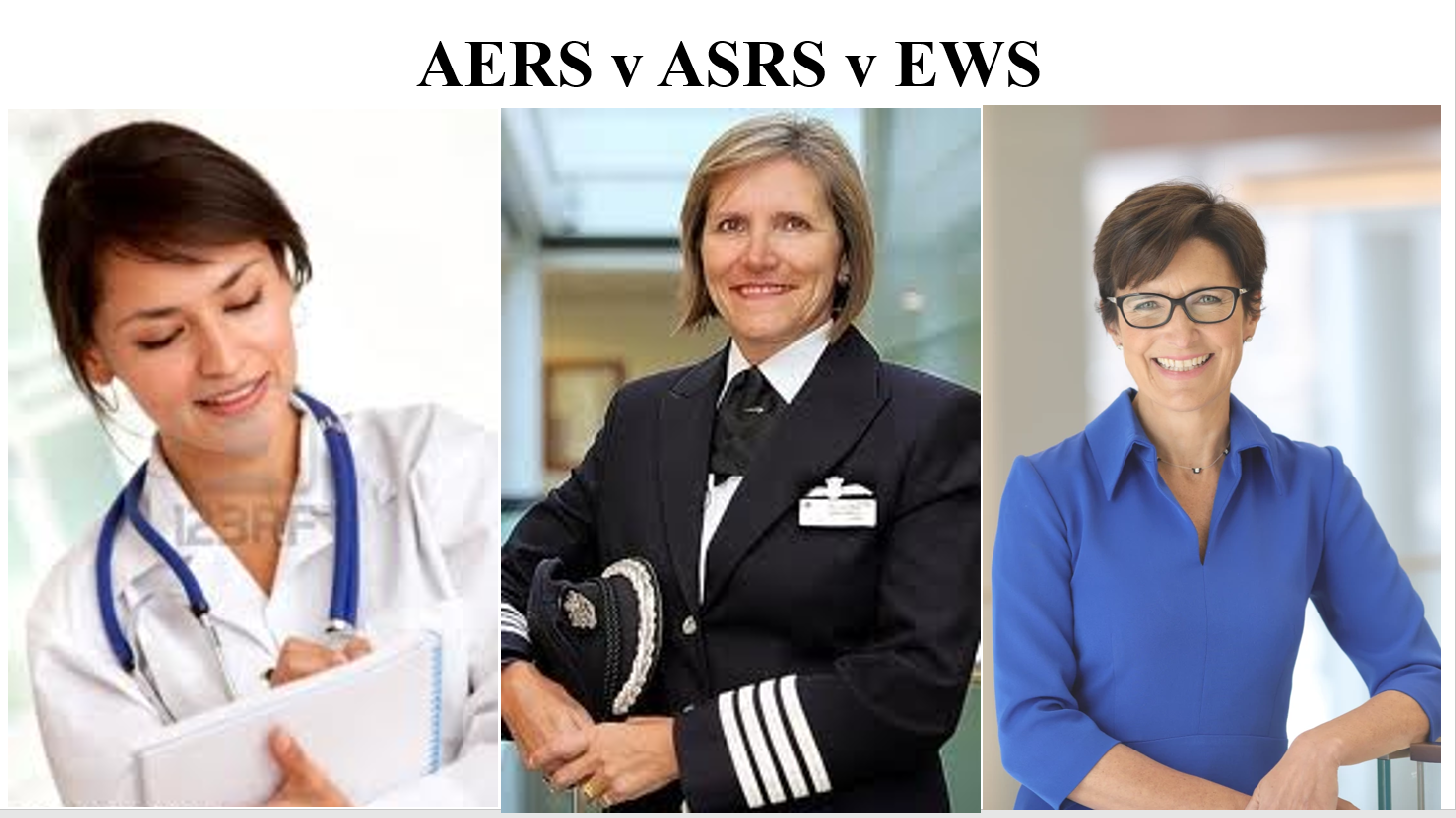
Slide 55: When the pilot here reports problems, safety systems pay heed because they know she won’t fly if they don’t because of the consequences for her.
Jane Frazer is the CEO of Citibank. Since the financial crisis, bankers have an Early Warning System. Who knows if it helps? The financial crisis was linked to a moral hazard. Bankers were outsourcing risk, knowing that if things crashed you and I would suffer but they would continue to collect their bonuses. This made it hard for them to do the right or brave thing.
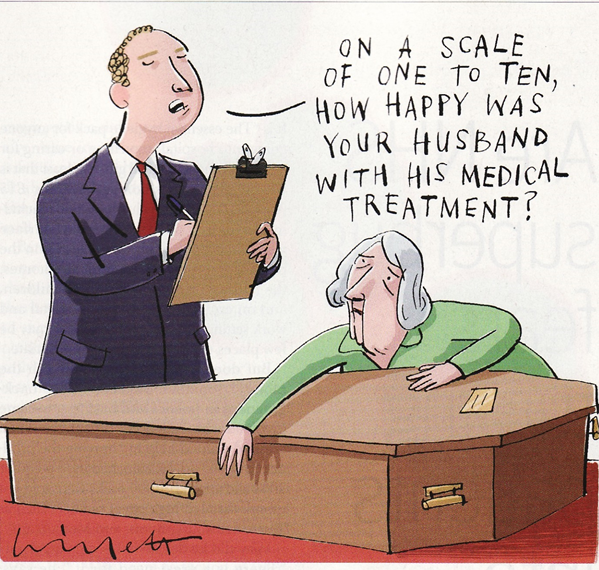
If the doctor on the left reports a problem, no-one pays any heed. She too outsources risk putting pills that like mortgages look too good to be true in our mouths. This is morally hazardous. Like a mortgage, if a drug looks too good to be true it probably is. If we blow up, she continues to be well paid. There is no incentive for her to do the right thing.
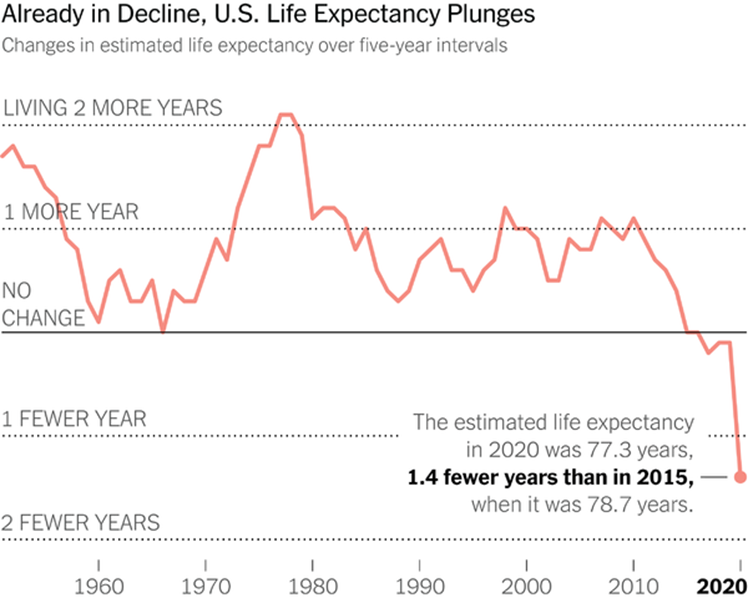
Slide 56: This moral hazard is leading to a pharmaceutical crisis that maps onto the financial crisis of 15 years ago. Here is a recent New York Times image of Life Expectancy in the US. You’ll see it began dropping in 1980, when we began treating numbers rather than people and converted health into a service industry. This Fall cannot be attribued to COVID. My view is that it is most likely linked to polypharmacy. The UK has similar falling Life Expectancy data – again pre-COVID.
![]()
Slide 57: Drugs like guns are techniques – amoral. The morality of their use lies in us. If we stop thinking about what we are doing when we use them, we are highly likely to be diminished.
Like Guns, Drugs create an arms race. The country with the best Medical Techniques and Guns wins wars and both armament and medical developments have been driven forward by military needs – to keep men able to fight in the case of drugs.
There is difference between Guns and Drugs. The chemicals in drugs are always risky. The information that transforms those chemicals into medicines has become increasingly dangerous. At the moment, the Drugs Race is not a better Chemical Race – it’s about creating more effective propaganda. The best propaganda is invisible – in this case it masquerades as science. The greatest concentration of fake literature on earth now centers on the reports of RCTs on the Drugs our doctors give us.
With both Guns and Drugs there is a limit to effectiveness. In the case of the Atom Bomb it is so effective that it cannot be used. It is the same with Drugs, if you are on more than 3, the effectiveness of each falls off as you add more meds into the mix.
To get the most effectiveness you need to be on 3 or less. As of 2016, over 40% of over 45s in the United States were on 3 or more drugs every day of the year – this figure includes the people who never come to see doctors. Over 40% of over 65s are on 5 or more drugs every day of the week. Knowing what is happening teenagers, this can only increase.
We know that reducing medication burdens can increase life expectancy, reduce hospitalizations, and improve quality of life.

Slide 58: Reducing a medication burden is not easy – as this image from the movie The Hurt Locker illustrates. Many of these drugs explode on attempting to withdraw them. This is the primary medical task of our age and there will never be any RCTs to help us out. The best evidence will likely lie in clinical experience of tackling similar situations. Great if I have a walkie-talkie to clinical colleagues but my key partner in this is you – you bring cues from missing doses of some of these drugs, and your sense of what they are doing that I can only access through you. And of course you ultimately dictate which risks we take.
In the 1940s and 1950s, RCTs had a role when we didn’t know if things worked. From the 1960s we had so many good drugs that worked – brought on the market without an RCT in sight – a new role beckoned for RCTs – to work out what worked best. RCTs cannot do this and besides it did not suit company interests. Companies instead created Randomized Controlled Assays which among other things allow weaker and weaker drugs on the market.
The pressing medical need now is to get people off the meds they are on and RCTs and what is called EBM have little or no role to play in helping us with this.

Slide 59: If a doctor tries to modestly reduce medication burdens or recognize that in some cases a treatment might have become a problem, current public health systems will not accommodate her. In the US, it is current culture that will mobilize against this. The doctor will be told this would be a good private practice offer that people can choose, but the public health system expectation is that people want and should get more diagnoses and drugs.
This is because getting treatment to save our lives was once a privilege and wealth and public health systems want everyone to be able to access treatment. They cannot now see that these good intentions are killing people. Now we have to be wealthy to get off medicines to save our lives.
Canada now leads the world in MAiD – Medical Assistance in Dying. In places like Belgium and Holland young women are getting MAiD because they have drug induced treatment resistant depression. While there must be concerns when young women in their 20s get MAID for treatment resistant depression – an antidepressant induced illness – I’m not quibbling about the morality of MAiD – any good doctor will almost certainly have cases where MAiD is the caring thing to do.
What I am quibbling about is the morality of a system that encourages us to have any service we want, including MAiD, but denies us the option of having less services. Denies us a Greener, more sustainable HealthCare. At the moment, not even Green parties have got a handle on this.
Slide 60: This lady comes from an Arthurian Legend. Arthur has been out-fought by a Black Knight who spares his life if he can answer a riddle – What do Women Most Desire. He has a year to find the answer. He and his court hunt desperately for it. The day he is due to die, Arthur and his troop meet this woman who tells him that she has the answer to the riddle but one of his knights must become her husband. Gawain jumps down and offers himself up. Arthur answers the riddle, and a furious Black Knight lets him go.
Slide 61: Gawain gets married. Everyone at the Court is unhappy for him.

Slide 62: In the bedchamber Gawain can’t bear to look at her. She takes control and asks him – do you want me to look like this by night with you and the way I was by day in court or like this by day in court. He has no idea and says – whatever you want. This is the right answer.
The answer to both riddles is she, like us, wants to control her own life. There may be a disease that needs treating – but she doesn’t want us to tell her how to live life, or want her negative emotions eliminated with a pill. She may be doing better at living life than you or I.
The evidence based medicine we now practice creates a False We – a non-existent average person – a fairy tale.
Rather than paying heed to the non-existent average person who comes out of clinical trials, when we relearn that we can learn much more from the person right in front of us, she and others who come to see us will seem more interesting and as they sense that we will be more attractive to them – easier to work with.
A relationship based medicine is the only validly scientific form of clinical practice. If you can’t build up a relationship with people because you and they see a different doctor every time, a relationship in which you are looking closely at and listening attentively to them – perhaps even detecting if there is a change in their smell, you are not doing science. The person in front of you is the apparatus in which the experiment is taking place. The computer screen is not.
Both science and morality depend on collaboration. Collaboration creates a virtuous circle – an Us – that leaves us all better placed to live the life we want to live. It creates Social Capital.
Redesignate Company Trials as Assays
Government of the People by the People has been replaced by governance.
If it is not to perish entirely from the earth…
We need to do…
Footnotes
This may be the most important lecture I have ever given – it’s the longest at least. It has been heavily shaped by Dee Mangin, Peter and Julie Wood and everyone linked to RxISK – Bill James, Johanna Ryan, Peter Selley, Sarah Tilley, Mary Hennessey, Annemarie Kelly and many others who have worked behind the scenes but don’t want to be named and others whose comments on posts are often more illuminating than the posts themselves.
It has been shaped over a 25 year period by Andy Vickery, Cindy Hall, Skip Murgatroyd and Michael Baum who in the legal cases they involved me in brought me face to face with the many issues covered here.
It has been shaped by Jon Jureidini, Melissa Raven, Joanna Le Noury, and Elia Abi-Jaoude, who along with Mickey Nardo and Catalin Tufanaru, both now dead, were the team behind the Restoration of Study 329 – see the final article at Restoring Study 329.
It would not be possible to leave Peter Goetzsche out of the frame and an intense struggle to restore the Prozac trials in adolescents – along with the bravery of Ralph Edwards in publishing this paper. See Flat as Kansas.
Finally to complete a set of Peters, Peter Doshi has been one of the most remarkable people working on all these issues extraordinarily effectively.
There have been any number of fabulous media people like Shelley Jofre and Andy Bell who brought key issues to light, along with Ariane Denoyel and others who have grappled with the issues outlined here.
More recently, Dan Johnson, along with Yoko Motohama and Vincent Schmitt who have lost teenage sons to the drugs mentioned here, triggered the series of lectures noted above of which this is the third in the series. Jon Thompson and his colleagues in the math department in the University of New Brunswick, along with Peter Selley and colleagues in the Devon and Exeter Medical Society allowed me to dress rehearse and improve the talk.
I have stolen ideas from lots of people such as Steve Lanes – too many to acknowledge. As Steve’s example shows, some of the best help has come from people working in industry.
The Q and A after this talk in Boston reveals a tendency we all have to say things would be fine if industry just weren’t involved in trials. This is not my view. Industry don’t help but they are primarily exploiting medical failures to get to grips with the faultlines in RCTs – and a medical willingness to accept a simplistic solution to the problem of objectivity rather than engage with others in establishing what is objective or at least the best provisional version of objectivity.

The Covid-skeptic world has been claiming the World Health Organization (WHO) plans to become some sort of global autocratic government, removing national sovereignty and replacing it with a totalitarian health state. The near-complete absence of interest by mainstream media would suggest, to the rational observer, that this is yet another ‘conspiracy theory’ from a disaffected fringe.
The imposition of authoritarian rules on a global scale would normally attract attention. The WHO is fairly transparent in its machinations. It should therefore be straightforward to determine whether this is all misplaced hysteria, or an attempt to implement an existential change in sovereign rights and international relations. We would just need to read the document. Firstly, it is useful to put the amendments in context.
The changing role of WHO
Who’s WHO?
The WHO was set up after the Second World War as the health arm of the United Nations, to support efforts to improve population health globally. Based on the concept that health went beyond the physical (encompassing “physical, mental and social well-being”), its constitution was premised on the concept that all people were equal and born with basic inviolable rights. The world in 1946 was emerging from the brutality of colonialism and international fascism; the results of overly centralized authority and of regarding people to be fundamentally unequal. The WHO constitution was intended to put populations in charge of health.
In recent decades the WHO has evolved as its support base of core funding allocated by countries, based on GDP, evolved to a model where most funding is directed to specified uses, and much is provided by private and corporate interests. The priorities of the WHO have evolved accordingly, moving away from community-centered care to a more vertical, commodity-based approach. This inevitably follows the interests and self-interests of these funders. More detail can be found on this evolution elsewhere; these changes are important to putting the proposed IHR amendments in context.
Of equal importance, the WHO is not alone in the international health sphere. While certain organizations such as UNICEF (originally intended to prioritize child health and welfare), private foundations and non-government organizations have long partnered with the WHO, the past two decades have seen a burgeoning of the global health industry, with multiple organizations, particularly ‘public-private partnerships’ (PPPs) growing in influence; in some respects rivals and in some respects partners of the WHO.
Notable among PPPs are the Gavi – the Vaccine Alliance (focused specifically on vaccines) and CEPI, an organization set up at the World Economic Forum meeting in 2017 specifically to manage pandemics, by the Bill & Melinda Gates Foundation, Wellcome Trust and the Norwegian Government. Gavi and CEPI, along with others such as Unitaid and the Global Fund, include corporate and private interests directly on their boards. The World Bank and G20 have also increased involvement in global health, and especially pandemic preparedness. The WHO has stated that pandemics occurred just once per generation over the past century and killed a fraction of those who died from endemic infectious diseases, but they nonetheless attract much of this corporate and financial interest.
The WHO is primarily a bureaucracy, not a body of experts. Recruitment is based on various factors, including technical competency but also country and other equity-related quotas. These quotas serve a purpose of reducing the power of specific countries to dominate the organization with their own staff, but in doing so require the recruitment of staff who may have far lower experience or expertise. Recruitment is also heavily influenced by internal WHO personnel, and the usual personal influences that come with working and needing favors within countries.
Once recruited, the payment structure strongly favors those who stay for long periods, mitigating against rotation to new expertise as roles change. A WHO staffer must work 15 years to receive their full pension, with earlier resignation resulting in removal of all or part of the WHO’s contribution to their pension. Coupled with large rental subsidies, health insurance, generous education subsidies, cost-of-living adjustments and tax-free salaries, this creates a structure within which protecting the institution (and thus one’s benefits) can far outlive initial altruistic intent.
The DG and Regional Directors (RDs – of which there are six) are elected by member states in a process subject to heavy political and diplomatic maneuvering. The current DG is Tedros Adhanom Ghebreyesus, an Ethiopian politician with a checkered past during the Ethiopian civil war. The amendments proposed would allow Tedros to independently make all the decisions required within the IHR, consulting a committee at will but not bound by it. Indeed, he can do this now, having declared monkeypox a public health emergency of international concern (PHEIC) against his emergency committee’s advice, after just five deaths globally.
Like many WHO employees, I personally witnessed, and am aware of, examples of seeming corruption within the organization, from Regional Director elections to building renovations and importation of goods. Such practices can occur within any large human organization that has lived a generation or two beyond its founding. This is, of course, why the principle of the separation of powers commonly exists in national governance; those making rules must answer to an independent judiciary according to a system of laws to which all are subject. As this cannot apply to UN agencies, they should automatically be excluded from direct rulemaking over populations. The WHO, like other UN bodies, is essentially a law unto itself.
WHO’s new pandemic preparedness and health emergency instruments.
The WHO is currently working on two agreements that will expand its powers and role in declared health emergencies and pandemics. These also involve widening the definition of ‘health emergencies’ within which such powers may be used. The first agreement involves proposed amendments to the existing International Health Regulations (IHR), an instrument with force under international law that has been in existence in some form for decades, significantly amended in 2005 after the 2003 SARS outbreak.
The second is a new ‘treaty’ that has similar intent to the IHR amendments. Both are following a path through WHO committees, public hearings and revision meetings, to be put to the World Health Assembly (WHA – the annual meeting of all country members [‘States parties’] of the WHO), probably in 2023 and 2024 respectively.
The discussion here concentrates on the IHR amendments as they are the most advanced. Being amendments of an existing treaty mechanism, they only require approval of 50 percent of countries to come into force (subject to ratification processes specific to each member State). The new ‘treaty’ will require a two-thirds vote of the WHA to be accepted. The WHA’s one country – one vote system gives countries like Niue, with less than two thousand residents, equal voice to countries with hundreds of millions (e.g. India, China, the US), though diplomatic pressure tends to corral countries around their beneficiaries.
The IHR amendments process within the WHO is relatively transparent. There is no conspiracy to be seen. The amendments are ostensibly proposed by national bureaucracies, collated on the WHO website. The WHO has gone to unusual lengths to open hearings to public submissions. The intent of the IHR amendments to change the nature of the relationship between countries and the WHO (i.e. a supra-national body ostensibly controlled by them), and fundamentally change the relationship between people and central supranational authority – is open for all to see.
Major amendments proposed for the IHR
The amendments to the IHR are intended to fundamentally change the relationship between individuals, their country’s governments, and the WHO. They place the WHO as having rights overriding that of individuals, erasing the basic principles developed after World War Two regarding human rights and the sovereignty of States. In doing so, they signal a return to a colonialist and feudalist approach fundamentally different to that to which people in relatively democratic countries have become accustomed. The lack of major pushback by politicians and the lack of concern in the media and consequent ignorance of the general public is therefore both strange and alarming.
Aspects of the amendments involving the largest changes to the workings of society and international relations are discussed below. Following this are annotated extracts from the WHO document (REF). Provided on the WHO website, it is currently under a process of revision to address obvious grammatical errors and improve clarity.
Resetting international human rights to a former, authoritarian model
The Universal Declaration on Human Rights, agreed by the UN in the aftermath of World War Two and in the context of much of the world emerging from a colonialist yoke, is predicated on the concept that all humans are born with equal and inalienable rights, gained by the simple fact that they are born. In 1948 the Universal Declaration of Human Rights was intended to codify these, to prevent a return to inequality and totalitarian rule. The equality of all individuals is expressed in Article 7:
“All are equal before the law and are entitled without any discrimination to equal protection of the law. All are entitled to equal protection against any discrimination in violation of this Declaration and against any incitement to such discrimination.”
This understanding underpins the WHO constitution, and forms a basis for the modern international human rights movement and international human rights law.
The concept of States being representative of their people, and having sovereignty over territory and the laws by which their people were governed, was closely allied with this. As peoples emerged from colonialism, they would assert their authority as independent entities within boundaries that they would control. International agreements, including the existing IHR, reflected this. The WHO and other international agencies would play a supportive role and give advice, not instructions.
The proposed IHR amendments reverse these understandings. The WHO proposes that the term ‘with full respect for the dignity, human rights and fundamental freedoms of persons’ be deleted from the text, replacing them with ‘equity, coherence, inclusivity,’ vague terms the applications of which are then specifically differentiated in the text according to levels of social and economic development. The underlying equality of individuals is removed, and rights become subject to a status determined by others based on a set of criteria that they define. This entirely upends the prior understanding of the relationship of all individuals with authority, at least in non-totalitarian states.
It is a totalitarian approach to society, within which individuals may act only on the sufferance of others who wield power outside of legal sanction; specifically a feudal relationship, or one of monarch-subject without an intervening constitution. It is difficult to imagine a greater issue facing society, yet the media that is calling for reparations for past slavery is silent on a proposed international agreement consistent with its reimposition.
Giving WHO authority over member States.
This authority is seen as being above states (i.e. elected or other national governments), with the specific definition of ‘recommendations’ being changed from ‘non-binding’ (by deletion) to ‘binding’ by a specific statement that States will undertake to follow (rather than ‘consider’) recommendations of the WHO. States will accept the WHO as the ‘authority’ in international public health emergencies, elevating it above their own ministries of health. Much hinges on what a Health Emergency of International Concern (PHEIC) is, and who defines it. As explained below, these amendments will widen the PHEIC definition to include any health event that a particular individual in Geneva (the Director General of the WHO) personally deems to be of actual or potential concern.
Powers to be ceded by national governments to the DG include quite specific examples that may require changes within national legal systems. These include detention of individuals, restriction of travel, the forcing of health interventions (testing, inoculation) and requirement to undergo medical examinations.
Unsurprising to observers of the COVID-19 response, these proposed restrictions on individual rights under the DG’s discretion include freedom of speech. The WHO will have power to designate opinions or information as ‘mis-information or disinformation, and require country governments to intervene and stop such expression and dissemination. This will likely run up against some national constitutions (e.g. the US) but will be a boon to many dictators and one-party regimes. It is, of course, incompatible with the Universal Declaration of Human Rights, but these seem no longer to be guiding principles for the WHO.
After self-declaring an emergency, the DG will have power to instruct governments to provide WHO and other countries with resources – funds and commodities. This will include direct intervention in manufacturing, increasing production of certain commodities manufactured within their borders.
Countries will cede power to the WHO over patent law and intellectual property (IP), including control of manufacturing know-how, of commodities deemed by the DG to be relevant to the potential or actual health problem that he /she has deemed of interest. This IP and manufacturing know-how may be then passed to commercial rivals at the DG’s discretion. These provisions seem to reflect a degree of stupidity, and unlike the basic removal of fundamental human rights, vested interests here may well insist on their removal from the IHR draft. Rights of people should of course be paramount, but with most media absent from the fray, it is difficult to see a level of advocacy being equal.
Providing the WHO DG with unfettered power, and ensuring it will be used.
The WHO has previously developed processes that ensure at least a semblance of consensus and an evidence-base in decision-making. Their process for developing guidelines requires, at least on paper, a range of expertise to be sought and documented, and a range of evidence weighed for reliability. The 2019 guidelines on management of pandemic influenza are an example, laying out recommendations for countries in the event of such a respiratory virus outbreak. Weighing this evidence resulted in the WHO strongly recommending against contact tracing, quarantine of healthy people and border closures, as the evidence had shown that these are expected to cause more overall harm to health in the long term than the benefit gained, if any, from slowing spread of a virus. These guidelines were ignored when an emergency was declared for COVID-19 and authority switched to an individual, the director general.
The IHR amendments further strengthen the ability of the DG to ignore any such evidence-based procedures. Working on several levels, they provide the DG, and those delegated by the DG, with exceptional and arbitrary power, and put in place measures that make the wielding of such power inevitable.
Firstly, the requirement for an actual health emergency, in which people are undergoing measurable harm or risk of harm, is removed. The wording of the amendments specifically removes the requirement of harm to trigger the DG assuming power over countries and people. The need for a demonstrable ‘public health risk’ is removed, and replaced with a ‘potential’ for public health risk.
Secondly, a surveillance mechanism set up in every country under these amendments, and discussed also in the pandemic preparedness documents of the G20 and World bank, will identify new variants of viruses which constantly arise in nature, all of which, in theory, could be presumed to pose a potential risk of outbreak until proven not to. The workforce running this surveillance network, which will be considerable and global, will have no reason for existence except to identify yet more viruses and variants. Much of their funding will originate from private and corporate interests that stand to gain financially from the vaccine-based responses they envision for infectious disease outbreaks.
Thirdly, the DG has sole authority to declare any event rated (or potentially related) to health an ‘emergency.’ (The six WHO Regional Directors (RDs) will also have this power at a Regional level). As seen with the monkeypox outbreak, the DG can already ignore the committee set up to advise on emergencies. The proposed amendments will remove the need for the DG to gain consent from the country in which a potential or perceived threat is identified. In a declared emergency, the DG can vary the FENSA rules on dealing with private (e.g. for-profit) entities, allowing him/her to share a State’s information not only with other States but with private companies.
The surveillance mechanisms being required of countries and expanded within the WHO will ensure that the DG and RDs will have a constant stream of potential public health risks crossing their desks. In each case, they will have power to declare such events a health emergency of international (or Regional) concern, issuing orders supposedly binding under international law to restrict movement, detain, inject on mass scales, yield intellectual property and know-how, and provide resources to the WHO and to other countries the DG deems to require them. Even a DG uninterested in wielding such power will face the reality that they put themselves at risk of being the one who did not ‘try to ‘stop’ the next pandemic, pressured by corporate interests with hundreds of billions of dollars at stake, and huge media sway. This is why sane societies never create such situations.
What happens next?
If these amendments are accepted, the people taking control over the lives of others will have no real legal oversight. They have diplomatic immunity (from all national jurisdictions). The salaries of many will be dependent on sponsorship from private individuals and corporations with direct financial interest in the decision they will make. These decisions by unaccountable committees will create mass markets for commodities or provide know-how to commercial rivals. The COVID-19 response illustrated the corporate profits that such decisions will enable. This is a situation obviously unacceptable in any democratic society.
While the WHA has overall oversight on WHO policy with an executive board comprised of WHA members, these operate in an orchestrated way; many delegates having little depth in the proceedings whilst bureaucrats draft and negotiate. Countries not sharing the values enshrined in the constitutions of more democratic nations have equal vote on policy. Whilst it is right that sovereign States have equal rights, the human rights and freedom of one nation’s citizens cannot be ceded to the governments of others, nor to a non-State entity placing itself above them.
Many nations have developed checks and balances over centuries, based on an understanding of fundamental values, designed specifically to avoid the sort of situation we now see arising, where one group is law unto itself can arbitrarily remove and control the freedom of others. Free media developed as a further safeguard, based around principles of freedom of expression and an equal right to be heard. These values are necessary for democracy and equality to exist, just as it is necessary to remove them in order to introduce totalitarianism and a structure based on inequality. The proposed amendments to the IHR set out explicitly to do this.
The proposed new powers sought by the WHO, and the pandemic preparedness industry being built around it, are not hidden. The only subterfuge is the farcical approach of media and politicians in many nations who seem to pretend they are not proposed, or do not, if implemented, fundamentally change the nature of the relationship between people and centralized non-State powers. The people who will become subject to these powers, and the politicians who are on track to cede them, should start paying attention. We must all decide whether we wish to cede so easily what it has taken centuries to gain, to assuage the greed of others.
Annotated summary of significant clauses in the IHR amendments.
Notes. (Within qualities from the IHR draft, italics are added for emphasis here.
DG: Director General (Of the WHO)
FENSA: (WHO) Framework for Engagement of Non-State Actors
IHR: International Health Regulations
PHEIC: Public Health Emergency of International Concern.
WHA: World Health Assembly
WHO: World Health Organization
“States Parties’ in UN parlance (i.e. self-governing countries) is simplified below to ‘State(s)’ or ‘country’.
See full document at the WHO IHR portal.
- Setting the scene: Establishing WHO authority over individuals and national governments in health-related decision-making.
Article 1: Definitions
‘Health technologies and knowhow’;: Includes ‘other health technologies’, [any of these that solve a health problem and improve ‘quality of life’ and includes technologies and knowhow involved in the] ‘development and manufacturing process’, and their ‘application and usage’.
Note relevance to requirement for countries to give these up to other entities on WHO demand. This must be unacceptable to most existing legal systems and corporations.
“standing recommendation’ means non-binding advice issued by WHO
“temporary recommendation” means non-binding advice issued by WHO
‘standing recommendations’ and ‘temporary recommendations:’ The removal of the ‘non-binding’ is consistent with the requirement later for States to consider the ‘recommendations’ of the DG as obligatory.
Article 2: Scope and purpose (of the IHR)
_“The purpose and scope of these Regulations are to prevent, protect against_, prepare**, control and provide a public health response to the international spread of diseases including through health systems readiness and resilience in ways that are commensurate with and restricted to public health risk all risks with a potential to impact public health**, and which …”
Wording changed from “restricted to public health risk” to “restricted to all risks with a potential to impact public health.” Public health is an extremely broad term, and potential risks can be any virus, toxin, human behavioral change, article or other information source that could affect anything in this vast field. This is an open slather that would in operation provide the WHO with a jurisdiction over anything potentially vaguely pertaining to some change in health or well-being, as perceived by the DG or delegated staff. Such broad rights to interfere and take control would not normally be allowed to a government department. In this case, there is no direct oversight from a parliament representing people, and no specific legal jurisdiction to comply with. It allows the WHO director general to insert himself and give recommendations (no longer ‘non-binding’ to almost anything pertaining to societal life (health, in the WHO’s definition, is physical, mental and social well-being).
Article 3: Principles
“The implementation of these Regulations shall be with full respect for the dignity, human rights and fundamental freedoms of persons based on the principles of equity, inclusivity, coherence and in accordance with their common but differentiated responsibilities of the States Parties, taking into consideration their social and economic development”
This signals a fundamental change in the human rights approach of the UN, including the Universal Declaration on Human Rights (UDHR) that all UN countries have signed up to. The concept of broad, fundamental rights (equal in all) is removed, and replaced with vacuous wording ‘equity, inclusivity, coherence.’ Human rights (of the individual) are seen as based on economic and ‘social’ development. This implies that the wealthy and poor have different rights, and there is a hierarchy of ‘development’ that defines one’s rights. This is a return to a feudalist or colonialist view of human rights (in many respects the excuses used to justify slavery), that the post-War WHO and UDHR had sought to move away from.
“shall be guided by the goal of their universal application for the protection of all people of the world from the international spread of disease. When implementing these Regulations, Parties and WHO should exercise precaution, in particular when dealing with unknown pathogens.“
Again, addition of a clause that enables the WHO to override human rights previously stated, including for speculative (unknown) threats.
Article 4: Responsible authorities
Each country is required to appoint an ‘authorized responsible authority’ for WHO to liaise with. Seemingly innocuous, but reflects the mindset change in status within these regulations, with the WHO becoming a body requiring compliance, no longer ‘suggesting’ or ‘supporting.’
- Establishing the international pandemic preparedness bureaucracy with WHO at the center
Article 5: Surveillance.
These amendments establish /expand a periodic review mechanism, similar to the UN human rights office. This seems in itself innocuous, but is a very large resource drain, especially for smaller countries, and requires (as in the human rights compliance case) a dedicated large international (WHO) bureaucracy and consultant base. WHO will require regular detailed reports, send assessors, and require changes. This raises questions both on (1) sovereignty in health and (2) rational and appropriate use of resources. WHO is not assessing the country’s health needs here, it is assessing one small aspect and dictating the resources spent on it, irrespective of other health burdens. This is a fundamentally poor and dangerous way to manage public health and means resources are unlikely to be spent for maximum benefit overall.
Article 6: Notification.
Countries (States Parties) to make information available to WHO at WHO request, and WHO can make this available to other parties (see later clauses) in a manner yet to be determined by the WHA. This may seem innocuous but in reality, removes State sovereignty over data (which had been significant prior to 2005 IHA amendments). It is unlikely that powerful States will comply, but smaller ones will be left with little choice (China has significantly inhibited information and will likely do so. It can be argued this is appropriate – such information can have significant economic and social implications).
Article 10: Verification
“If the State Party does not accept the offer of collaboration within 48 hours , WHO may shall , when justified by the magnitude of the public health risk, immediately share with other States Parties the information available to it, whilst encouraging the State Party to accept the offer of collaboration by WHO, _taking into account the views of the State Party concerned_.”
The WHO gains power to share information from a State or pertaining to a State with other States, without consent. This is remarkable: It is important to understand who the WHO is (essentially unaccountable beyond the WHA).
Article 11: Exchange of Information (Formerly provision of information by WHO).
This article enables WHO to share information obtained as discussed above, to both UN and non-governmental bodies (allowed recipients changed from (formerly) relevant intergovernmental to (now) relevant international and regional organizations (i.e. now including organizations not related to national governments).
WHO can therefore share State information with ‘relevant international organizations’ – this presumably includes such as CEPI, Gavi, Unitaid – organizations that have private and corporate representation on their boards with direct financial conflicts of interest.
Further:
“Parties referred to in those provisions, shall not make this information generally available to other States Parties, until such time as when: (a) the event is determined to constitute a public health emergency of international concern, a public health emergency of regional concern, or warrants an intermediate public health alert, in accordance with Article 12; or …”
Widens the criteria determining when the WHO can disseminate information from sovereign States, from PHEIC to ‘health alert’ (which in practice the DG or subordinates could apply to almost anything). This could occur, as specified later in the Article, when WHO staff decide a sovereign State does not have ‘capacity’ to handle a problem, or when the WHO staff decide (with unspecified criteria) that it is necessary to share information with others to make ‘timely’ risk assessments. This allows unelected WHO staff, on salaries supported from external conflicted entities, to disseminate information from States directly relevant to those entities, based on their own assessment of risk and response, against undefined criteria.
- Widening ‘public health emergency’ definition to include any health or pathogen-related event at DG’s discretion, and requiring States compliance.
Article 12: Determination of a public health emergency of international concern public health emergency of regional concern, or intermediate health alert
This Article both reduces the threshold for the DG to declare an emergency (it can just be a concern of a potential outbreak) and greatly increases the power of the WHO (removes requirement for State agreement) to then act.
“If the Director-General considers, based on an assessment under these Regulations, that a potential or actual public health emergency of international concern is occurring ….. determines that the event constitutes a public health emergency of international concern, and the State Party are in agreement regarding this determination, the Director-General shall notify all the States Parties, in accordance with the procedure set forth in Article 49, seek the views of the Committee established under Article 48 (but is not required to follow them)
Removes requirement for State to agree to release of information pertaining to that State. DG can declare a PHEIC against States wishes and instructions. The WHO becomes the dominant party, not the servant of the sovereign State.
Emergency committee review is optional for DG, who can act completely alone in determining PHEIC – a decision that can have vast health, social and economic implications and is allowed above to abrogate basic human rights norms.
_If, following the consultation in paragraph 2 above, the Director-General and the State Party in whose territory the event arises do not come to a consensus within 48 hours on whether the event constitutes a public health emergency of international concern, a determination shall be made in accordance with the procedure set forth in Article 49_.
Removes requirement of DG to seek agreement of State before acting.
“Regional Director may determine that an event constitutes a public health emergency of regional concern and provide related guidance to States Parties in the region either before or after notification of an event that may constitute a public health emergency of international concern is made to the Director-General, who shall inform all States Parties”
Regional directors appear to be granted similar powers, though full implications are unclear.
“In case of any engagement with non-State actors in WHO’s public health response to PHEIC situation, WHO shall follow the provisions of Framework for Engagement of Non-State Actors (FENSA). Any departure from FENSA provisions shall be consistent with paragraph 73 of FENSA.”
The WHO Framework for Engagement of Non-State Actors (FENSA) allows the DG to “exercise flexibility in the application of the procedures of FENSA” in the case of a health emergency (which here in the IHR is widened, as above, to any concern the FG has of potential harm, irrespective of State agreement.
“Developed State Parties and WHO shall offer assistance to developing State Parties depending on the availability of finance, technology and know how…”.
A line fascinating mainly for its anachronistic (but telling) use of the colonialist-like terms developing and developed in this formerly egalitarian WHO context.
“The State Party shall accept or reject such an offer of assistance within 48 hours and, in the case of rejection of such an offer, shall provide to WHO its rationale for the rejection, which WHO shall share with other States Parties. Regarding on-site assessments, in compliance with its national law, a State Party shall make reasonable efforts to facilitate short-term access to relevant sites; in the event of a denial, it shall provide its rationale for the denial of access”
WHO set as the dominant partner. The State must comply or provide excuses for not agreeing with WHO’s dictates.
“When requested by WHO, States Parties should shall provide, to the extent possible, support to WHO-coordinated response activities, including supply of health products and technologies, especially diagnostics and other devices, personal protective equipment, therapeutics, and vaccines, for effective response to PHEIC occurring in another State Party’s jurisdiction and/or territory, capacity building for the incident management systems as well as for rapid response teams”.
‘Should’ changed to ‘Shall,’ requiring States to provide resources at the WHO’s request for a PHEIC (e.g. monkeypox of an event the DG considers may pose a potential threat.) This begins a theme of the WHO acquiring the ability to order States to provide resources, and (later) know-how and intellectual property when ordered by the DG to do so.
NEW Article 13A WHO Led International Public Health Response
This new article explicitly lays out the new international public health order, with the WHO in charge at the center, rather than national sovereignty being paramount.
“States Parties recognize WHO as the guidance and coordinating authority of international public health response during public health Emergency of International Concern and undertake to follow WHO’s recommendations in their international public health response.”
This requires States to follow WHO recommendations in a PHEIC – declared by an individual (DG) whose position is determined by non-democratic states and who is open to wide influence by private and corporate money. The criteria for PHEIC are deliberately vague, and at the DG’s discretion. This is an amazing reversal of roles of the WHO versus States, and clearly abrogates sovereignty.
The wild failure of Covid response, and the WHO’s abrogation of its own guidelines, should give pause for thought here. The WHO could mandate abrogation of bodily autonomy on states regarding medication or vaccination, or testing.
“Upon request of WHO, States Parties with the production capacities shall undertake measures to scale up production of health products, including through diversification of production, technology transfer and capacity building especially in the developing countries.”
The WHO can require (tell) countries to scale-up production of certain products – to interfere with markets and commerce, at the WHO’s (DG’s) discretion.
NEW Article 13A WHO Led International Public Health Response
“**States Parties recognize WHO as the guidance and coordinating authority of international public health response during public health Emergency of International Concern and undertake to follow WHO’s recommendations in their international public health response**.”
This requires States to follow WHO recommendations in a PHEIC – declared by an individual (DG) whose position is determined by non-democratic states and who is open to wide influence by private and corporate money. The criteria for PHEIC are deliberately vague, and at the DG’s discretion. This is an amazing reversal of roles of WHO versus States, and clearly abrogates sovereignty. It is requiring sovereign states to submit themselves to an external authority, whenever that authority desires it (as the WHO DG can through previous amendments above, declare a PHEIC on the basis of just perceiving the potential form an infectious disease event).
The Covid response, including the WHO’s abrogation of its own guidelines and policies, should give pause for thought here. The WHO could mandate abrogation of bodily autonomy on states regarding medication or vaccination, or testing.
“**Upon request of WHO, States Parties with the production capacities shall undertake measures to scale up production of health products, including through diversification of production, technology transfer and capacity building especially in the developing countries.**”
The WHO can require (tell) countries to scale-up production of certain products – to interfere with markets and commerce, at WHO’s (DG’s) discretion.
“ [WHO] shall collaborate with other international organizations, and other stakeholders consistent with the provisions of FENSA, for responding to public health emergency of international concern.**”**
This enables the WHO to collaborate with non-State actors (private individuals, Foundations, private corporations (Pharma, its sponsors etc.). FENSA, which restricts such contacts, can be varied by the DG in a ‘health emergency’ that the DG declares.
- WHO requiring countries to provide resources, intellectual property and knowhow at WHO’s discretion.
New Article 13A: Access to Health Products, Technologies and Know-How for Public Health Response
“States Parties shall co-operate with each other and WHO to comply with such recommendations pursuant to paragraph 1 and shall take measures to ensure timely availability and affordability of required health products such as diagnostics, therapeutics, vaccines, and other medical devices required for the effective response to a public health emergency of international concern.”
The WHO determines response within States’ borders, and requires States to provide aid to other countries. At the WHO’s behest.
“**States Parties shall provide, in their intellectual property laws and related laws and regulations, exemptions and limitations to the exclusive rights of intellectual property holders to facilitate the manufacture, export and import of the required health products, including their materials and components**.”
States shall change their intellectual property (IP) laws, to allow sharing of IP on the DG’s determination of a PHEIC, at his/her discretion, to whom they determine. It is difficult to imagine a sane State would do this, but it is clearly required here.
“States Parties shall use or assign to potential manufacturers, especially from developing countries, on a non-exclusive basis, the rights over health product(s) or technology(ies)”
The WHO can require IP to be shared with other States (and thereby IP is passed to private corporations within those States.
“Upon request of a State Party, other States Parties or WHO shall rapidly cooperate and share relevant regulatory dossiers submitted by manufacturers concerning safety and efficacy, and manufacturing and quality control processes, within 30 days”
Requirement to release confidential regulatory dossiers to other States, including to WHO qualification programme, and to sovereign state regulatory agencies.
“[WHO shal]… establish a database of raw materials and their potential suppliers, e) establish a repository for cell-lines to accelerate the production and regulatory of similar biotherapeutics products and vaccines”,
WHO holding such materials is unprecedented. Under whose laws and regulatory requirements would this be done? Who is responsible for damage and harm?
“**States Parties shall take measures to ensure that the activities of non-state actors, especially the manufacturers and those claiming associated intellectual property rights, do not conflict with the right to the highest attainable standard of health and these Regulations and are in compliance with measures taken by the WHO and the States Parties under this provision, which includes:**
a) to comply with WHO recommended measures including allocation mechanism made pursuant to paragraph 1.
b) to donate a certain percentage of their production at the request of WHO.
c) to publish the pricing policy transparently.
d) to share the technologies, know-how for the diversification of production.
e) to deposit cell-lines or share other details required by WHO repositories or database established pursuant to paragraph 5.
f) to submit regulatory dossiers concerning safety and efficacy, and manufacturing and quality
control processes, when called for by the States Parties or WHO.”
The ‘highest attainable standard of health is beyond what any State has now. This effectively means, as worded, that the WHO can require any state to release almost any confidential product and intellectual property on any product related to the health sector.
This is an amazing list. The DG (WHO) on their own criteria can declare an event, then require a State to contribute resources and give up sole rights to intellectual property of its citizens, and share information to allow others to manufacture their citizen’s products in direct competition. The WHO also requires States to donate products to the WHO /other States on DG’s demand.
To understand the scope of the intellectual property rights to be forfeited to the DG, the definitions (Article 1) describe them as:
“health technologies and know-how” includes organized set or combination of knowledge, skills, health products, procedures, databases and systems developed to solve a health problem and improve quality of life, including those relating to development or manufacture of health products or their combination, its application or usage …”.
- WHO claiming control of individuals and their rights within States
Article 18 Recommendations with respect to persons, baggage, cargo, containers, conveyances, goods and postal parcels.
“Recommendations issued by WHO to States Parties with respect to persons may include the following advice:…..
– review proof of medical examination and any laboratory analysis;
- require medical examinations;
- review proof of vaccination or other prophylaxis;
- require vaccination or other prophylaxis;
- place suspect persons under public health observation;
- implement quarantine or other health measures for suspect persons;
- implement isolation and treatment where necessary of affected persons;
- implement tracing of contacts of suspect or affected persons;
- refuse entry of suspect and affected persons;
- refuse entry of unaffected persons to affected areas; and
- implement exit screening and/or restrictions on persons from affected areas.”
This (article 18) was already in existence. New Article 13A, however, now requires States to follow WHO recommendations. The WHO will thus now be able to, based on the sole determination of an individual (DG) under influence of non-democratic states and private entities, order states to incarcerate their citizens, inject them, require identification of medical status, medically examine, isolate and restrict travel.
This is clearly insane.
“[Recommendations issued by WHO shall]…ensure mechanisms to develop and apply a traveller’s health declaration in international public health emergency of international concern (PHEIC) to provide better information about travel itinerary, possible symptoms that could be manifested or any prevention measures that have been complied with such as facilitation of contact tracing, if necessary.”
The WHO can require the availability of private travel (itinerary) information, and require the provision of medical travel documents. This is requiring the disclosure of private medical information to the WHO.
Article 23 Health measures on arrival and departure
“Documents containing information concerning traveller’s destination (hereinafter Passenger Locator Forms, PLFs) should preferably be produced in digital form, with paper form as a residual option. Such information should not duplicate the information the traveller already submitted in relation to the same journey, provided the competence authority can have access to it for the purpose of contact tracing.”
Text (which clearly needs further work) aimed at future requirements for vaccine passports for travel.
- WHO setting the scene for digital health passports
Article 35 General rule
“**Digital health documents must incorporate means to verify their authenticity via retrieval from an official web site, such as a QR code.**”
Further presaging digital IDs containing health information, that must be available to enable travel (i.e. not at individual’s discretion).
Article 36 Certificates of vaccination or other prophylaxis
“Such proofs may include test certificates and recovery certificates. These certificates may be designed and approved by the Health Assembly according to the provisions set out for digital vaccination or prophylaxis certificates, and should be deemed as substitutes for, or be complementary to, the digital or paper certificates of vaccination or prophylaxis.”
As above. Setting up the WHO/WHA to set international travel requirements (the UDHR says there is a basic right to travel). While not new here, this is expanded by the expansion of PHEIC provisions, and focused more on the DG’s determination. It is moving from national sovereignty to a transnational travel control beyond national sovereignty – not directly answerable to populations, but heavily funded and influenced by private interests.
“Health measures taken pursuant to these Regulations, including the recommendations made under Article 15 and 16, shall be initiated and completed without delay by all State Parties”
Requirement for all countries to comply with these recommendations (they only take 50 percent of the WHA to implement).
“State Parties shall also take measures to ensure Non-State Actors operating in their respective territories comply with such measures**.”**
Also requires private entities and citizens within the state to comply (which likely requires changes of many national laws, and the relationship between government and people).
This requires a totalitarian approach from the State, subject to a totalitarian approach from a supra-state (but clearly not meritocratic) entity. Following these IHR revisions, the DG of WHO, at his discretion, has the capacity to order private entities and citizens in any country to comply with his/her directives.
- WHO being empowered to order changes within States, including restrictions on freedom of speech.
Article 43 Additional health measures
“[Measures implemented by States shall not be more restrictive than.]… would achieve attain the appropriate highest achievable level of health protection.”
These changes are very significant. Appropriate’ meant taking into account the costs and balancing these against potential gains. It is a sensible approach that takes the whole of society and population needs into account (good public health).
‘highest achievable level of protection’ means elevating this problem (an infectious disease or potential disease) above all other health and human/societal concerns. This is stupid, and probably reflects lack of thought and poor understanding of public health.
“WHO may request that shall make recommendations to the State Party concerned reconsider to modify or rescind the application of the additional health measures …”
On removing health interventions, the WHO DG now can require such actions (States have agreed to ‘recommendations’ being binding above). As elsewhere, the WHO is not the instructing party, not the suggesting party. The WHO takes sovereignty over formerly State matters. The following paragraph requires a response in 2 weeks rather than formerly 3 months.
Article 44 Collaboration and assistance
“States Parties shall undertake to collaborate with and assist each other, in particular developing countries States Parties, upon request, _to the extent possible_, in:…”
Changes move the relationship from the WHO suggesting/requesting, to the WHO requiring.
“in countering the dissemination of false and unreliable information about public health events, preventive and anti-epidemic measures and activities in the media, social networks and other ways of disseminating such information.”
States undertake to work with the WHO to control information and limit free speech.
“the formulation of proposed laws and other legal and administrative provisions for the implementation of these Regulations.”
States agree to pass laws to implement restrictions on free speech and sharing of information.
“countering the dissemination of false and unreliable information about public health events, preventive and anti-epidemic measures and activities in the media, social networks and other ways of disseminating such information;…”
The WHO shall work with countries to control free speech and flow of information (based on their own criteria of what is right and wrong).
- Nuts and Bolts of the verification bureaucracy to ensure countries follow WHO requirements.
NEW Chapter IV (Article 53 bis-quater): The Compliance Committee
53 bis Terms of reference and composition
“The State Parties shall establish a Compliance Committee that shall be responsible for:
(a) Considering information submitted to it by WHO and States Parties relating to compliance with obligations under these Regulations;
(b) Monitoring, advising on, and/or facilitating assistance on matters relating to compliance with a view to assisting States Parties to comply with obligations under these Regulations;
(c) Promoting compliance by addressing concerns raised by States Parties regarding implementation of, and compliance with, obligations under these Regulations; and
(d) Submitting an annual report to each Health Assembly describing:
(i) The work of the Compliance Committee during the reporting period;
(ii) The concerns regarding non-compliance during the reporting period; and (iii) Any conclusions and recommendations of the Committee.
2. The Compliance Committee shall be authorized to:
(a) Request further information on matters under its consideration;
(b) Undertake, with the consent of any State Party concerned, information gathering in the territory of that State Party; (c) Consider any relevant information submitted to it; (d) Seek the services of experts and advisers, including representatives of NGOs or members of the public, as appropriate; and (e) Make recommendations to a State Party concerned and/or WHO regarding how the State Sarty may improve compliance and any recommended technical assistance and financial support.”
This sets up the permanent review mechanism to monitor the compliance of States with the WHO’s dictates on public health. This is a huge new bureaucracy, both centrally (WHO) and with a significant resource drain on each State. It reflects the review mechanism of the UN human rights office.
- More on WHO requiring states to provide taxpayer money to WHO’s work, and restricting freedom of populations to question this work.
ANNEX 1
A. CORE CAPACITY REQUIREMENTS FOR DISEASE DETECTION, SURVEILLANCE
AND HEALTH EMERGENCY RESPONSE
“**Developed Countries States parties shall provide financial and technological assistance to the Developing Countries States Parties in order to ensure state-of-the-art facilities in developing countries States Parties, including through international financial mechanism…”**
States shall provide (i.e. divert from other priorities) aid funding to help other States develop capacity. This has a clear opportunity cost in other disease/societal programs where funding must accordingly be reduced. However, this will no longer be in the budgetary control of States, but required by an external entity (WHO).
“**At a global level, WHO shall… Counter misinformation and disinformation”.**
As above, the WHO takes the role of policing / countering free speech and exchange of information (funded by the taxes of those whose speech they are suppressing).
Useful links
The WHO documents regarding the IHR amendments
A summary of the amendments and their implications
Author
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
[](https://brownstone.org/author/david-bell/)

Before coming to Kiev, President Joe Biden sought assurances from Russia that it would not bomb his special train.
The first anniversary of the East-West military confrontation in Ukraine was an opportunity for the West to convince its people that they were "on the right side of history" and that their victory was "inevitable."
None of this is surprising. It is normal for governments to communicate about their activities. Except that here the information is lies by omission and the comments are propaganda. This is such a reversal of reality that one wonders whether the defeated of the Second World War have not come to power in Kiev today.
Russia’s illegal, unjustifiable and unprovoked war
All Western interventions claim that we condemn the "illegal, unjustifiable and unprovoked war of Russia" [1]. This is factually wrong.
Let’s leave aside the qualification of "unjustifiable". It refers to an indecent moral position. No war is just. Every war is the acknowledgement, not of a fault, but of a failure. Let us examine the qualifier "unprovoked".
According to Russian diplomacy, the problem began with the 2014 US-Canadian operation and the overthrow of the democratically elected Ukrainian president, Viktor Yanukovych, in violation of Ukrainian sovereignty and thus the UN Charter. There is no denying that Washington was instrumental in this so-called "revolution of dignity": the then Assistant Secretary of State for Europe and Eurasia, Victoria Nuland, posted herself at the head of the coup plotters.
According to Chinese diplomacy, which has just published two documents on the subject, one should not stop at this operation, but go back to the "Orange Revolution" of 2004, also organized by the United States, to see the first violation of Ukrainian sovereignty and the United Nations Charter. Obviously, if Russia does not mention it, it is because it also played a role in it, which it did not do in 2014.
The Western public is so shocked by the ease with which the United States manipulates mobs and overthrows governments that it is no longer aware of the seriousness of these events. From the overthrow of Mohammad Mossadegh in Iran in 1953 to the overthrow of Serge Sarkissian in Armenia in 2018, it has become accustomed to forced regime changes. Whether the deposed leaders were good or bad should not matter. What is unbearable and inadmissible is that a foreign state organized their overthrow by masking its action behind a few national opponents. These are acts of war, without military intervention.
Facts are stubborn. The war in Ukraine was caused by the violations of Ukrainian sovereignty in 2004 and 2014. These violations were followed by an eight-year civil war.
Nor is war illegal under international law. The UN Charter does not prohibit the use of war. The Security Council even has the possibility of declaring war (articles 39 to 51). This time the particularity is that it opposes permanent members of the Council.
Russia co-signed the Minsk Agreements to end the civil war. However, not having been born yesterday, it understood from the start that the West did not want peace, but war. So she had the Minsk Agreements endorsed by Security Council Resolution 2202, five days after their conclusion, and then forced the Russian oligarch Konstantin Malofeyev to withdraw his men from the Ukrainian Donbass. It attached to the resolution a statement by the presidents of France, Ukraine and Russia, as well as the German chancellor, guaranteeing the implementation of these texts. These four signatories committed their countries.
– Ukrainian President Petro Poroshenko declared in the following days that there was no question of giving anything up, but rather of punishing the inhabitants of Donbass.
– Former Chancellor Angela Merkel told Die Zeit [[2](#nb2 ""Hatten Sie gedacht, ich komme mit Pferdeschwanz?", Tina Hildebrandt und (...)")] that she only wanted to buy time so that NATO could arm the authorities in Kiev. She unknowingly clarified her statement in a discussion with a provocateur she believed to be former President Poroshenko.
– Former President Francois Hollande confirmed in Kyiv Independent the words of Mrs. Merkel [3].
– That left Russia, which implemented a special military operation on February 24, 2022 under its "responsibility to protect". To say that its intervention is illegal is to say, for example, that France’s intervention during the genocide in Rwanda was also illegal and that the massacre should have been allowed to continue.
Emails from Russian President Vladimir Putin’s special adviser Vladislav Surkov, which have just been revealed by the Ukrainian side, only confirm this process. In the years that followed, Russia helped the Ukrainian republics of Donbass prepare intellectually for independence. This interference was illegal. It was in response to the equally illegal interference of the United States, which armed not Ukraine but the Ukrainian "integral nationalists. The war had already begun, but Ukrainians exclusively conducted it. It resulted in 20,000 deaths in 8 years. The West and Russia intervened only indirectly.
It is important to understand that by pretending to negotiate peace, Angela Merkel and François Hollande have committed the worst of crimes. Indeed, according to the Nuremberg Tribunal, "crimes against peace" are even more serious than those "against humanity". They are not the cause of this or that massacre, but of the war itself. This is why the chairman of the Duma, Vyacheslav Volodin, has called for the convening of a new Nuremberg Tribunal to try Angela Merkel and François Hollande [4]. The Western press has not relayed this call, which shows us the gulf between the two perceptions of the conflict.
The order of the International Court of Justice of March 16, 2022 stated, as a precautionary measure, that "the Russian Federation must immediately suspend the military operations which it began on February 24, 2022 on the territory of Ukraine" (ref: A/77/4, paragraphs 189 to 197). Moscow did not comply, considering that the Court had been asked about the requirement of genocide perpetrated by Kiev against its own population and not about the military operation to protect the Ukrainian population.
For its part, the United Nations General Assembly has adopted several resolutions, the latest of which is A/ES-11/L.7, of February 23, 2023. The text "Reiterates its demand that the Russian Federation immediately, completely and unconditionally withdraw all its military forces from Ukrainian territory within the internationally recognized borders of the country, and calls for a cessation of hostilities.
Neither of these texts declares the Russian intervention "illegal. They order or demand that the Russian army withdraw. 141 of 193 states consider that Russia should stop its intervention. Some of them think it is illegal, but most of them think it is "no longer necessary" and is causing unnecessary suffering. This is not the same thing at all.
States have a different point of view than jurists. International law can only sanction what exists. States must protect their citizens from the conflicts that are brewing, before it is too late to respond. That is why the Kremlin did not comply with the UN General Assembly. It did not withdraw from the battlefield. Indeed, it has watched for eight years as NATO has armed Ukraine and prepared for this war. It knows that the Pentagon is preparing a second round in Transnistria [5] and must protect its population from this second operation. Just as it chose the date of its intervention in Ukraine on the basis of information indicating an imminent attack by Kiev on the Donbass, which was only confirmed later [6], so ot is deciding today to liberate the whole of Novorossia, including Odessa. This is legally unacceptable as long as the proof of the Western shenanigans is not provided, but it is already necessary from the point of view of its responsibility.
Clearly, these two ways of thinking have not escaped the notice of observers. Judging that Russian intervention is no longer necessary must be distinguished from supporting the West. That is why only 39 out of 191 states participate in Western sanctions and send weapons to Ukraine.
Ukraine is a "democracy"
The second message from Western leaders is that Ukraine is a "democracy". Apart from the fact that this word has no meaning at a time when the middle classes are disappearing and income disparities have become greater than at any other time in human history, moving away from the egalitarian ideal, Ukraine is anything but a "democracy.
Its constitution is the only racist one in the world. It states in Article 16 that "Preserving the genetic heritage of the Ukrainian people is the responsibility of the state", a passage written by Slava Stetsko, the widow of the Ukrainian Nazi prime minister.
This is the subject that makes people angry. At least since 1994, "full nationalists" (not to be confused with "nationalists"), i.e., people who claim to follow the ideology of Dmytro Dontsov and the work of Stepan Bandera, have held high positions in the Ukrainian state [7]. In fact, this ideology has become more radical over time. It did not have the same meaning during the First World War as during the Second. Nevertheless, Dmytro Dontsov was, from 1942 on, one of the designers of the "final solution of the Jewish and Gypsy questions". He was the administrator of the organ of the Third Reich in charge of murdering millions of people because of their ethnic origin, the Reinhard Heydrich Institute in Prague. Stepan Bandera was the military leader of the Ukrainian Nazis. He commanded numerous pogroms and massacres. Contrary to what his successors claim, he was never interned in a concentration camp, but under house arrest in the suburbs of Berlin, at the headquarters of the concentration camp administration. He ended the war leading the Ukrainian troops under the direct orders of the Führer Adolf Hitler.
One year after the beginning of the Russian military intervention, full nationalist and Nazi symbols are visible everywhere in Ukraine. Forward journalist Lev Golinkin, who has started an inventory of all monuments to criminals involved in Nazi crimes all over the world, has compiled an amazing list of such monuments in Ukraine [8]. According to him, almost all of them are after the 2014 coup. Therefore, it must be admitted that the coup authorities do claim to be "integral nationalism", not simply "nationalism". And for those who doubt that the Jewish President Zelensky celebrates the Nazis, two weeks ago he awarded the "Edelweiss title of honor" to the 10th separate mountain assault brigade in reference to the Nazi 1st mountain division that "liberated" (sic) Kiev, Stalino, the Dnieper crossings and Kharkov [9].
Few Western personalities have agreed with the words of President Vladimir Putin and his Foreign Minister Sergei Lavrov on this subject [10]. However, Israeli Prime Minister Naftali Bennett and his Defense Minister, General Benny Gantz, have repeatedly stated that Ukraine must comply with Moscow’s injunctions at least on this point: Kiev must destroy all Nazi symbols it displays. It is because Kiev refuses to do so that Israel does not deliver weapons to it: no Israeli weapons will be handed over to the successors of the mass murderers of Jews. This position may of course change with the coalition government of Benjamin Netanyahu, himself an heir to Vladimir Jabotinsky’s "revisionist Zionists" who formed an alliance with the "integral nationalists" against the Soviets.
The current policy of the government of Volodymyr Zelensky is incomprehensible. On the one hand, the democratic institutions are functioning, on the other hand, not only are the integral nationalists being celebrated everywhere, but the opposition political parties and the Orthodox Church under the jurisdiction of the Moscow Patriarchate have been banned; millions of books have been destroyed because they were written or printed in Russia; 6 million Ukrainians have been declared "collaborators of the Russian invader" and the personalities who support them are being assassinated.

The USSR collapsed in on itself, not from the war in Afghanistan (1979-89), but from the Chernobyl disaster (April 26, 1989). The Soviets suddenly realized that the state was no longer in control. The members of the Warsaw Pact, whom Leonid Brezhnev had made vassals, revolted. The churches, the Communist Youth and the gays of East Germany brought down the Berlin Wall [1]. Not only did the USSR not react, but also it abandoned its allies outside Europe, especially Cuba. The First Secretary of the party, Mikhail Gorbachev, turned from a reformer into a liquidator. The USSR broke up, creating many new independent states. Then it was a descent into hell. A few "New Russians" appropriated the collective assets and waged a machine-gun war in the streets of Moscow and St. Petersburg. Production collapsed. It became difficult to find food in many Russian regions. Life expectancy dropped sharply by about 15 years. The fall was so sharp that no one thought the country would recover quickly.
At the same time, the United States imagined what it could do without a rival. President George H. Bush Sr. addressed a full Congress on September 11, 1990, and floated the idea of a "New World Order. He had just staged a war in the Gulf that almost every state in the world joined. Even before the dissolution of the USSR, the United States had become the hyperpower that no one contests [2]. The Straussian Paul Wolfowitz elaborated a doctrine aimed at preventing the emergence of a new competitor, which would take the place of the Soviet Union. He unhesitatingly designated the political project of François Mitterrand and Helmut Köhl, the European Union, as the enemy to be destroyed. The European Union was flawed from the start, with the obligation to bring in all the Warsaw Pact states and the former USSR until its institutions became unworkable and the Maastricht Treaty stipulated that Washington would defend the EU.
The Pentagon was so sure that it no longer had an adversary that it demobilized one million men once Iraq was crushed. The research and development units of the armies were disbanded. President Bush Sr. believed that this was the last war and that an era of prosperity was beginning.
Although no one threatens the supremacy of the US, it feels that its internal balance is fragile. Their jobs have been relocated and their economy is based more on the internationalization of their currency, the dollar, than on the wealth they produce.
In 2001, the Straussians organized the September 11 attacks [3] and adopted the Rusmfeld/Cebrowski doctrine [4]. They suspended fundamental freedoms at home with the USA Patriot Act and wage an "endless war" that ravaged the "wider Middle East".
Russia, however, did not see it that way. In a speech given on February 11, 2007 at the Munich Security Conference [5], President Vladimir Putin denounced the Bush New World Order as "unipolar". According to him, it would be more accurate to describe it as "monopolistic". He notes that far from bringing peace, it sowed misfortune.
During the subprime crisis, the Russian intellectual Igor Panarin, who was working for the secret service at the time, studied the hypothesis that the dollar would collapse and the US population would be divided along ethnic lines, so that the country would eventually break up [6]. His work was wrongly interpreted as a replica of the hypothesis of the Frenchwoman Helène Carrère d’Encausse, who envisaged a break-up of the Soviet Union, also on an ethnic basis. None of this happened, nor was my hypothesis that the "American empire" would not survive the "Soviet empire" verified.
So what did happen?
In the 15 years since the Munich speech, Russia’s priority has been to rebuild its power. In 2012, it promised to protect Syria from Anglo-Saxon-backed jihadists (the so-called "Arab Spring"), but waited two years before intervening. When it came out of the shadows, it had plenty of new weapons. On the battlefield, it learned how to use them and trained its personnel, which it renewed every six months. Although Vladimir Putin, in his Munich speech, named Brazil, India and China as his privileged partners in building a multipolar world, he waited a long time before sealing a privileged relationship with Beijing. China, which is still partly developing, is putting a lot of demographic pressure on Russian Siberia, but it has understood that, in order to get out of the "monopoly dictatorship," it must be Russia’s ally. Both countries have suffered from the West and have experienced their lies. They have no future without each other.
Western defeat in Ukraine should be an eye-opener for the United States. The tensions examined by Igor Panarin are resurfacing. The attacks of September 11 and the "endless war" will have been nothing more than a diversion. They gave the "American empire" a reprieve, but nothing more.
In the 35 years since the collapse of the USSR, the United States has wrongly convinced itself that it has defeated its rival. In reality, it was the Soviets themselves who overthrew it. They believed that the Russians would need a century to recover from their mistakes. In fact, they have become the world’s leading military power. The United States has succeeded in subjugating Western and Central Europe, but today it must confront all the states it has bullied, led by Russia and China.
During this period, the Republicans and Democrats have given way to two new currents of thought: the Jacksonians around Donald Trump and the Wokists, puritans without God. We are currently witnessing an intensification of population movements in the USA. Electoral specialists note that many Americans are leaving the Woke regions and joining the Jacksonians [7]. Moving companies report that their clients are leaving large cities for smaller ones where life is cheaper and more pleasant. However, they all note that their customers increasingly cite a new motive: they are moving to join family members. This explanation is consistent with what Colin Woodard observed a decade ago [8]: U.S. citizens are clustering by community of origin. Real estate developers are observing the multiplication of gated communities. Their clients are grouping together with people like themselves, having inherited the same culture and belonging to the same social class. They often worry about the rise of insecurity and talk about a possible civil war.
Let’s not be blind. All empires are mortal. So is the "American empire".
[1] « À l’Est : la Révolution Gay », par Didier Marie, Rebel (France), Réseau Voltaire, 1er mars 1993.
[2] “Bush’s Strategic Doctrine”, by Thierry Meyssan, Voltaire Network, 9 July 2004.
[3] “Everything points to Thierry Meyssan being right today”, by Thierry Meyssan, Translation Roger Lagassé, Voltaire Network, 3 September 2021.
[4] “The Rumsfeld/Cebrowski doctrine”, by Thierry Meyssan, Translation Roger Lagassé, Voltaire Network, 25 May 2021.
[5] “The unipolar governance is illegal and immoral”, by Vladimir Putin, Voltaire Network, 11 February 2007.
[6] The crash of the dollar and the disintegration of the USA (only in Russian), Igor Panarin (2008).
[7] «On the move», Jennifer Harper, The Washington Times, April 14, 2023.
[8] American nations : a history of the eleven rival regional cultures of North America, Colin Woodard, Penguin Group (2011).

In this article, I will discuss the observations of unethical and criminal activity that have been repeatedly made by whistleblowers in the pharmaceutical industry. The focus will be on insider disclosures of the toxic corporate culture at Pfizer and the company’s habitual tendency to conduct illegal activity in order to maximize pharmaceutical sales. In many cases, this misconduct has lead to disastrous consequences (e.g., for participants in its experimental trials or for the public at large their drugs were marketed to), and in each case, Pfizer has done everything it can to conceal its illegal activity.
In the first part of this series, I discussed the profound challenges a whistleblower faces when they break the code of silence held by the pharmaceutical industry. Nonetheless, a few people have been willing to make that sacrifice, and there is so much to learn from each of them. If you have not yet read it, I would highly recommend reading it first.
The Forgotten Side of Medicine -- What Can We Learn From the Pfizer Whistleblowers?
Because that code of silence has been in place for decades, the public is relatively unaware of what goes on within the industry. When insiders provide a window into that dark world, it is both shocking and difficult to believe. I had been working on this series for a while and felt that this was the time to release it because it helps create the context for both what Jordan Walker confided to Project Veritas about Pfizer and his surreal breakdown once he realized what he had done.

In this series, I chose to focus on Peter Rost, a pharmaceutical executive who, through a very odd set of circumstances, became a Pfizer Vice President (Pfizer typically never lets outsiders assume that role). Once appointed, he found himself in the very odd position of having to dig up as much dirt on Pfizer as possible to avoid getting fired. Rost witnessed the Pfizer company cruelly abusing his Pharmacia coworkers and to a lesser extent Pfizer’s own employees (detailed in part 1); therefore, he was not opposed to unearthing information that incriminated Pfizer. Best of all, because Rost had been stripped of his work responsibilities, he had plenty of time to investigate his employer.
Rost’s Vendetta
Rost’s talent was recognized by his sales-focused industry, and many of his superiors held him in high regard. Unfortunately for Pfizer, as detailed in part 1, Rost was not comfortable being complicit in criminal activity, so when he encountered it, he would choose to take action against it (thereby putting himself in conflict with the ethos of his industry).
In a previous job, Rost had reported Wyeth (another large pharmaceutical company) for tax evasion, and as fate would have it, that lawsuit became publicized shortly after Rost had managed to put himself in a position where Pfizer could not fire him. Nonetheless, Pfizer did all that they could against Rost, including providing much of the incriminating information they had collected on him to Wyeth.
Due to the previous lawsuit against Wyeth, Rost was able to obtain a copy of all documentation on him that Pfizer and Pharmacia had sent to his previous employer to Wyeth (which began occurring once they were made aware of his lawsuit against Wyeth). From these documents, Rost learned that Pfizer and Pharmacia had hired private investigators to dig up as much dirt as possible on him to prove that he was a security risk, and then they had forwarded these documents to Wyeth:
I had never seen anything like this before and I was truly shocked and appalled. I had gone from company high performer to security threat in a matter of days. This was something I couldn’t have imagined in my wildest dreams. Pharmacia was a company that I had trusted—the fact that I had found illegal marketing and sales methods in my department didn’t mean that I stopped trusting the entire corporation. But now, I felt as if I had been in a beautiful candlelit room, only to have a lightning flash suddenly reveal cracks, mold, and cob- webs. I just couldn't believe what I saw, and even worse, they had sent all this to Wyeth. All the loyalty I had felt to the company, all the respect I had had for executives in the organization vanished. And I was left with the ugly truth: I couldn’t trust anyone. To even try to talk to them and reason with them was futile.
But it got worse. As I flipped through the pages, I found more notes that Pharmacia’s lawyer had written after I had spoken with him. The most sensitive parts were blocked out by a fat black marker, but what remained was astonishing in itself. According to his conclusions, I had no choices; I was out of a job with no likelihood of employment in the industry; I had every incentive to fight Pfizer, and he also claimed that I already hated them. This was news to me: I hardly knew Pfizer, but I certainly was reevaluating what I thought of Pharmacia after reading this. Then came the whopper—the notes implied that I might put a gun to my head so my family could get my life insurance.
All of a sudden I realized what a mistake I had made, trying to get help from a Pharmacia lawyer. I recalled that during our conversation he had suggested for me to contact the Employee Assistance Program. Perhaps this attitude shouldn’t have been surprising; Pharmacia’s lawyer clearly thought that anyone who tried to resolve potential criminal acts within the company and keep his job was a mental case [_Rost also highlighted that a common tactic utilized by the Soviet Union against political dissidents was to diagnose them as being psychotic and then forcefully confine them to asylums_].
Fortunately, Pfizer failed to realize the mess they were in, because they had never dealt with someone who knew how to fight back:
In the next round of documents Pharmacia delivered to Wyeth a few weeks later, I saw Ronald’s reaction first-hand. His first mail to Pharmacia’s chief legal officer asked, “What the heck is this all about?”? Pharmacia responded that I seemed to believe that by not offering me a job, Pfizer was unlawfully retaliating against me. Then Pharmacia’s general counsel wrote, “I haven't done the research, but the theory seems dubious.”
This was very interesting. Pharmacia’s most senior legal officer admitted that he hadn't checked the legal implications of the actions they had taken against me. They clearly didn’t think I was al that important. While this is always a sobering realization, it also showed me how unprepared they were for dealing with an employee who actually knew some of his rights.
In short, a wonderful confluence of circumstances arose, which positioned Rost to do something no one else to my knowledge has ever done.
Digging for Dirt
Since he needed to ensure his job security, Rost decided that the best use of his time at work was to dig up as much dirt on Pfizer as possible:
I went on an info hunt, and it didn’t take long until I found my next surprise. Back in 2001, thirty Nigerian families had sued Pfizer in federal court, saying the company conducted an unethical clinical trial of an antibiotic [as the sole treatment for meningitis] on their children. The suit referred to a letter from the hospital saying the study had been approved by the ethics committee, and the suit claimed that Pfizer had backdated the letter.
Moreover, a Pfizer infectious disease specialist [discussed later in the article] had repeatedly told Pfizer management that the company was violating international law and medical ethics standards. He was subsequently dismissed and later settled with the company, according to other newspaper reports. Clearly, the fact that Pfizer was accused of backdating one letter and that I might have received another one was significant. And so was the fact that they had fired one alleged whistleblower already.
One of the many red flags raised here is Pfizer’s tendency to repeat the same criminal activity (Rost uncovered this series of events shortly after receiving a legal letter which he was almost certain was backdated).
Pfizer’s Employee Survey
Note: The quotations in this section and the next one comprise what is arguably the most important parts of the article.
Given that I didn’t have much to do anymore I had ample time to seek out Pfizer's weaknesses. As I searched the corporate intranet, I found exactly what I needed. Pfizer had done an exhaustive employee survey in 2001, and it was clear from the first page that CEO Hank McKinnell was proud about the fact that 88 percent of Pfizer’s employees had responded. There was lots of wonderful information about what Pfizer employees thought of the company; the highest ranked statement was, “I like working for Pfizer.” A whopping 89 percent of the employees agreed with this sentence.
The second most favorable result was generated by the statement, “I am proud to work for Pfizer,” a full 88 percent agreed with this. Only a contrarian might wonder why 12 percent weren't proud to work at Pfizer, or what those employees might have known about the company. At the time this survey was taken, 12 percent was equivalent to 6,000 employees.
But those weren't the numbers I was interested in. There was a different table in the survey that showed the lowest-ranked statements, and here things started to get interesting. The two most unfavorable ratings were given to the statements, “The right people get promoted,” and “People are promoted for the right reasons.” Only 36 percent and 42 percent agreed with these statements.
Soon I also discovered some data that didn’t rank at the bottom, but still was a major red flag to anyone that cares about corporate ethics. Some 30 percent of Pfizer’s employees, or about 15,000 persons at the time, didn’t agree with the statement, “Senior management demonstrates honest, ethical behavior.” And 34 percent didn’t agree with, “I have confidence and trust in senior management.” But the real surprise was that 49 percent didn’t agree with the statement, “Management is willing to give up short-term gain to do the right thing.” What was going on in Pfizer’s executive suite?
Note: Pfizer subsequently tried to bury these embarrassing results. The 2004 survey removed the embarrassing questions and the 2001 survey was wiped from the server after Rost discovered it. As this article will show, Pfizer has a tendency to make inconvenient documents disappear.
Unprofessional Boundaries
It wasn't hard to make the connection with the rumors I had heard before the acquisition. Pfizer had a stellar public reputation, but what Pharmacia employees had been told by their Pfizer counter- parts was something very different. This was a company managed by a group of people who had grown up together, partied together, and some of them had also allegedly spent time together between the sheets. What we heard was amazing—almost unbelievable.
I set out to find the truth. First I spoke to someone I knew well, an HR manager who had left Pfizer quite recently. He had spent many years working at Pfizer and believed the rumors were true—a group within Pfizer’s management had been in and out of bed with each other for a number of years. In one instance a senior person allegedly dated a direct report while he was married. Soon after, that direct report turned and dated a guy reporting to her. And then this guy dated several women in his department.
The problem with this alleged situation was that it could create tensions if someone thought someone else received a favorable treatment because of sexual favors. Real or imagined, this is a situation that can’t be tolerated by any management, since senior executives need to lead by example and can’t be effective if they aren't respected, which, clearly, certain Pfizer executives were not.
I actually knew someone who had worked with the woman in one of these alleged relationships. We met over lunch and I asked him to confirm if the stories were true. He claimed that not only were the stories true, he had personally observed the woman and her subordinate touch and make loving gestures. He also said that their behavior had been embarrassing to other people who were in the same room as these two.
He explained how they'd had to make special arrangements when the female executive was dating her boss, whenever his wife appeared at corporate functions.
I realized that if any of this were true, it could cause a public meltdown of Pfizer’s management team, much like the recent scandal at Boeing that had forced the CEO’s resignation. I also sensed that if Pfizer knew that I knew, they might just handle me more carefully.
After Rost alerted Pfizer to these issues, he succeeded in further raising their alarm, and their legal team immediately moved to investigate them. In the process, he learned even more about Pfizer’s leadership structure:
Before the meeting ended I repeatedly asked them to hire an independent law firm that could shield the identities of the people who had given me this information. In response, they made it clear that was not “how they operated.” They also discussed, and half laughed, about the impossibility of approaching the managers that were allegedly involved in these affairs. It was clear to me that they didn’t think they could confront members of senior management. I wondered if they would have been so cautious if this had been, for example, a district manager having an affair with a sales rep or someone else further down in the power structure.
More Fraud
In Rost’s continued quest to investigate wrongdoings, he found evidence that executives from Pharmacia’s Japan division had been cooking the books to inflate their sales numbers by reassigning sales from the next year to the previous one, in order to inflate their sales numbers to obtain a bonus. They also paid off wholesalers to go along with them. As he continued to look further into it, he also found evidence that this practice was also occurring in Pharmacia’s European markets.
This deceptive method is known as channel stuffing (“selling” more to the distribution channels than they can sell) and it inevitably unravels itself, since that increase keeps on needing to pull from more and more revenue in subsequent years to sustain itself.
Since channel stuffing constitutes investor fraud (as it provides incorrect data used to determine stock prices), the government will frequently prosecute it. Channel stuffing caused Enron’s downfall (the CEO was criminally sentenced but died shortly before his sentencing). In 2004, another pharmaceutical company, Bristol-Myers Squibb, was fined 150 million dollars for doing this. Similarly, another lawsuit involving channel stuffing eventually resulted in a 750 million dollar fine for ArthroCare, a surgical medical device manufacturer (along with prison sentences for its CEO and CFO).
I believe this prioritization of legal prosecution has developed because the wealthy write our laws, and the government is more incentivized to protect the interests of the rich (as opposed to those of the general public who are harmed by bad drugs). Similarly, my friends in the financial industry have seen that the most truthful information you can ever get from a pharmaceutical company is in its financial reports to investors.
Given the penalties for channel stuffing, this report also was of great concern to Pfizer, and gave Rost even more leverage over them. This was especially the case once Pfizer failed to appropriately address the issues, which in return gave Rost the grounds to open a U.S. Securities and Exchange Commission( SEC) investigation.
Pfizer’s Purgatory
Because Pfizer could not fire Rost, they tried to make things uncomfortable for him. He soon was reduced to having one employee (a secretary), isolated from everyone while at work, and left with nothing to do except show up at his office. They also repeatedly moved his office, until he pointed out that this constituted illegal harassment of a whistleblower. Since Rost was not allowed to do any work for Pfizer, he used that free time to research Pfizer’s internal workings, motivated also by their unconscionable abuse of their employees.
As Rost began bringing more improper and even illegal activity to Pfizer’s attention, he also noted this his emails would disappear, and incriminating documents he’d located would disappear. Eventually, Pfizer cut his access to his email without stating who had done it. Similarly, his communications (email and phone) were constantly monitored (despite this being against company policy), and Pfizer’s operators were instructed to prevent anyone from reaching him over the phone (although a sympathetic employee in the PR department sometimes would put them through).
To evaluate exactly how Pfizer was treating him behind his back, Rost would periodically utilize contacts in the industry to probe their behavior:
I spoke to the recruiter later in the day and I asked her where she had called and what the operator had said. The recruiter told me she had called Pfizer in New York, they had asked what her name was and the reason she wanted to talk to me, as well as some other questions.
“This happens al the time,” she said.
“Does this happen with al the pharmaceutical companies?” I asked.
“No, only with Pfizer. No one else does this.”
I asked her why she thought Pfizer did this, and she responded that based on the questions she had received she thought they recorded the information.
Rost Goes Public
The New England Journal of Medicine (NEJM) is considered to be one of the most prestigious medical journals in the world, and is also a frequent repository for fraudulent studies used to push some of the best selling pharmaceutical products onto the market (e.g., the human papillomavirus (HPV) vaccine or the COVID vaccine). In 2004, four years after her retirement (and a year into Rost’s purgatory), the chief editor of the NEJM, Marcia Angell M.D., published an excellent exposé of the issues within the drug industry, and the medical journals' complicity in this enterprise.
One of the quotes Dr. Angell is best known for is:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.”
_Note: More quotes from Dr. Angell can be found here._
On a whim, Rost decided to pen a review on Amazon, strongly endorsing Dr. Angell’s book, and within it openly declared that he was a Pfizer executive (it’s worth reading). This quickly got the attention of a journalist from USA Today who quoted Rost’s review in an article on the subject:
"It's really hard to find new drugs, and it's getting harder and harder," Rost, representing himself, not Pfizer, said in an interview. "There is a lot of low-hanging fruit out there that has been picked off. It is very, very difficult to really find a breakthrough." Instead, Rost says, drugmakers focus on tweaking existing drugs to make money, not to advance science.
_Note: As discussed in the previous article, in recent decades the inability to produce breakthrough drugs has been a major challenge for the industry (most of the new drugs are redundant unneeded “Me-too” drugs). I believe this dearth was a key motivation for why the mRNA technology was pushed through, as there is an almost limitless number of proprietary drugs that could be made with it._
Drug Reimportation
For decades, America has been known for having the worst ratio between healthcare expenditures and healthcare quality in the world (i.e., many places that spend far less than us have much better healthcare outcomes for their populace). Most tragically, this ratio only continues to worsen as we move forward in time (presently about 20% of all spending in the United States goes to healthcare).
Because there is so much money involved, I would argue that the systemic corruption within our healthcare system is almost inevitable. There is the tendency towards monopolization to protect its industry from competition In turn, the debacle we’ve witnessed throughout COVID-19 represented the inevitable progression of this industry’s greed.
It should, thus, come as no surprise that the drug industry charges as much for medications as it believes it can get away with. The cost of the same drugs varies widely from country to country, and as you might guess, the worst price-gouging occurs within the United States. Many people who struggle to afford their medications in the U.S. have noticed that these medications are much cheaper on the other side of the U.S. border (e.g., a Canadian pharmacy).
This observation has given rise to the practice of “drug reimportation” where drugs made in the United States that were exported for sale are bought in the international market and then imported back to the United States, and sold for a much lower price than they typically cost domestically. If you believe in capitalism and the free-market, drug reimportation should be allowed to correct market imbalances created by price gouging. However, if your business goal is to maintain a monopoly (and pay off the government to enforce it), drug reimportation is a huge problem, as it cuts into a lot of the profits made by ripping off the American public.
At this point, I have watched decades of failed attempts to reform the out-of-control costs in the healthcare system. In each case, because the legislators responsible for writing those laws (in one way or another) are bought out, no one was willing to tackle the real sources of price gouging in our healthcare marketplace, and each of those attempts failed. I would argue that this is why healthcare spending continues to rise in the United States.
As luck would have it for Rost, at the time he penned his review, the hot political issue was allowing drug reimportation (which the pharmaceutical was trying to torpedo by arguing that it somehow threatened consumer safety). Since Rost was a pharmaceutical executive willing to speak out against these practices (something virtually unheard of due to the consequences of doing so), and he knew a lot about the subject (e.g., Europe had had no issues with drug reimportation), he rapidly attracted the attention of the press and politicians who were trying to advance this issue.
I have to admit that my lawyer was not happy about al this. His job was to protect my legal case, which he told me was excellent. The fact that I was speaking up made me vulnerable and could have ruined the whole case. He was surely right that I took a big risk, but I felt that it was more important that I got the message out. And after a few months, Jon even said that I was doing a pretty good job. “Who knows,” he admitted. “You might actually achieve some change.”
Before long, Rost was called before congress to testify on the reimported drug issue. This was a nightmare for Pfizer (as their business depended upon inflated American drug prices), and in their panic, Pfizer managed to make things even worse for themselves through their crude attempts to discredit Rost and prevent him from communicating with the public. Before long, Rost’s message was heard throughout America.
But journalists and news anchors were still very surprised that I didn’t get fired [Rost could not publicly disclose his whistleblower status at the time]. It was as if everyone had forgotten that we live in a democracy with freedom of speech and other basic rights.
The biggest surprise, however, wasn't the flood of e-mails, or that many employees were upset about what I had said. The biggest surprise was that so many actually agreed with my comments. In fact, about 40 percent of the e-mails I received were supportive. I imagine it took a lot more guts to write a positive e-mail than to send a critical message and copy a superior. In truth, I wished my supporters hadn’t written, since I assumed that Pfizer was reading my e-mail.
Even a retiree wrote and agreed with me, “I applaud your efforts to encourage a more constructive approach to pharmaceutical importation. As a recent retiree from Pfizer, I am worried that by being short- sighted, Pfizer is doing something that is not its own best interest.”
_Note: Alex Berenson who wrote for the New York Times when Rost went public played a critical role in bringing Rost’s story to America. I suspect one of the reasons Berenson later became a critic of the COVID-19 response was because his career began in a bygone era when liberal journalists could still criticize the pharmaceutical industry and Bernson made a point to do just that during his time at the NYT._
Ultimately, Rost became too hot for anyone at Pfizer to handle, eventually leading to a situation where:
I never heard from either one of them [his assigned supervisors] again. To the best of my knowledge, I became the only Pfizer employee without a boss.
Pfizer nonetheless continued to harass Rost (e.g., they sent lawyers to monitor him at presentations he gave), while Rost continued to find creative ways to cause headaches for Pfizer (many are detailed within his book). One of the most impressive results he achieved was a group of doctors (unhappy with how Pfizer was treating Rost) independently deciding to ban Pfizer sales reps from their practices.
Pfizer is a very sales-oriented company and these events shook them up. Their worst nightmare would be a national boycott of their products.
What Happened with Drug Reimportation?
Although Rost was able to make the issue of drug reimportation a nationwide issue, it ultimately failed to be legalized because the “safety concerns could not be addressed.” While this result was expected, there were three interesting things I took away from all of it.
The first was how the issue was squashed (this should sound familiar to all of you):
By the end of December 2004, the Department of Health and Human Services came out with their report on drug importation. The report admitted that it would be possible to safely import drugs on a large scale, but claimed that establishing such a system wouldn't be cost effective.' The report also concluded that such a system would harm pharmaceutical companies’ research and development efforts.
The report was required by the new Medicare law, and had been developed by a thirteen-member panel led by U.S. Surgeon General Richard Carmona. Not surprisingly, the panel consisted of many rep- resentatives from several government agencies that oppose prescrip- tion drug reimportation.
They [and later Pfizer] used a study by the London School of Economics, which claimed that national health systems within the EU realized minimal savings from parallel- traded products. There was just one thing both the HHS report and the Pfizer letter forgot to mention. This “study” had been funded by the drug industry.
The second was the FDA’s promises to develop a “safe” way to import and reimport pharmaceuticals which two decades later still has not happened.
The final one was that some congressmen who had supported Rost at the time were still in the government twenty years later (e.g., Bernie Sanders), at which point, they chose to switch sides and stand behind Pfizer and their COVID-19 vaccine. Somewhat analogously, although many of my friends love Bernie Sanders, I have always been suspicious of him, because I know of cases where parents of vaccine-injured children tried to raise this issue with him and he shut them down instead of listening (Sanders has built a reputation as an advocate for disenfranchised groups that no one else will listen to).
Other Whistleblowers
John Virapen
The only other whistleblower I know of who was a pharmaceutical executive was John Virapen, so I will include him even though he was not involved with Pfizer. Virapen began life as a colonial subject of the British Empire (which translated to a childhood of abuse, discrimination, and poverty), in British Guyana, and eventually became a pharmaceutical sales rep. He excelled at what he was doing and eventually became an Eli Lilly executive in Sweden, who played the pivotal role in getting Prozac approved globally. Like Rost, he was backstabbed by the industry. Specifically, Eli Lilly fired Virapen after he won the approval, something he believed was due to Eli Lilly, like Pfizer being an old boys’ network that did not want an outsider of color like him in the management (Rost’s story likewise shows a similar old boys’ network existing at Pfizer).
Virapen experienced a great deal of guilt for what he was complicit in, and like Rost after he was fired, found himself in circumstances where he could speak out against the industry. In his memoir, he shared the routine criminal activity he engaged in (e.g., he had to make bribes to get Prozac approved in Sweden). He resorted to blackmail, such as photographing physicians with Eli-Lilly-provided prostitutes, to pressure them to conform to Eli Lilly’s sales requirements.
Note: a more detailed version of Virapen’s story can be found here. If Youtube pulls the above video, it can also be found here.
Dr. Juan Walterspiel
Although to my knowledge, no other executive has come forward, the pharmaceutical industry has many other whistleblowers including former Pfizer employees. For example, in the previously mentioned illegal Pfizer experiment in Nigeria, 11 of the 200 children with meningitis who were studied died [most of whom should not have with proper care], and later the highly toxic antibiotic they tested was subsequently pulled from the market.
One of the doctors at Pfizer’s research center tried to warn them about the trial but was ignored and eventually fired despite being a whistleblower (all of the events and the whistleblower lawsuit are summarized here and here). In addition to the trial being conducted in a reprehensible way (and was thought to have inspired the Constant Gardener), evidence also emerged that Pfizer bribed the Nigerian government to conduct the trial, and falsified documentation to appease the regulatory authorities.
John Kopchinski
Pfizer is also notorious for being greedy enough with their sales practices to be repeatedly fined for their criminal conduct (sadly this is not a complete list of Pfizer’s criminal settlements):
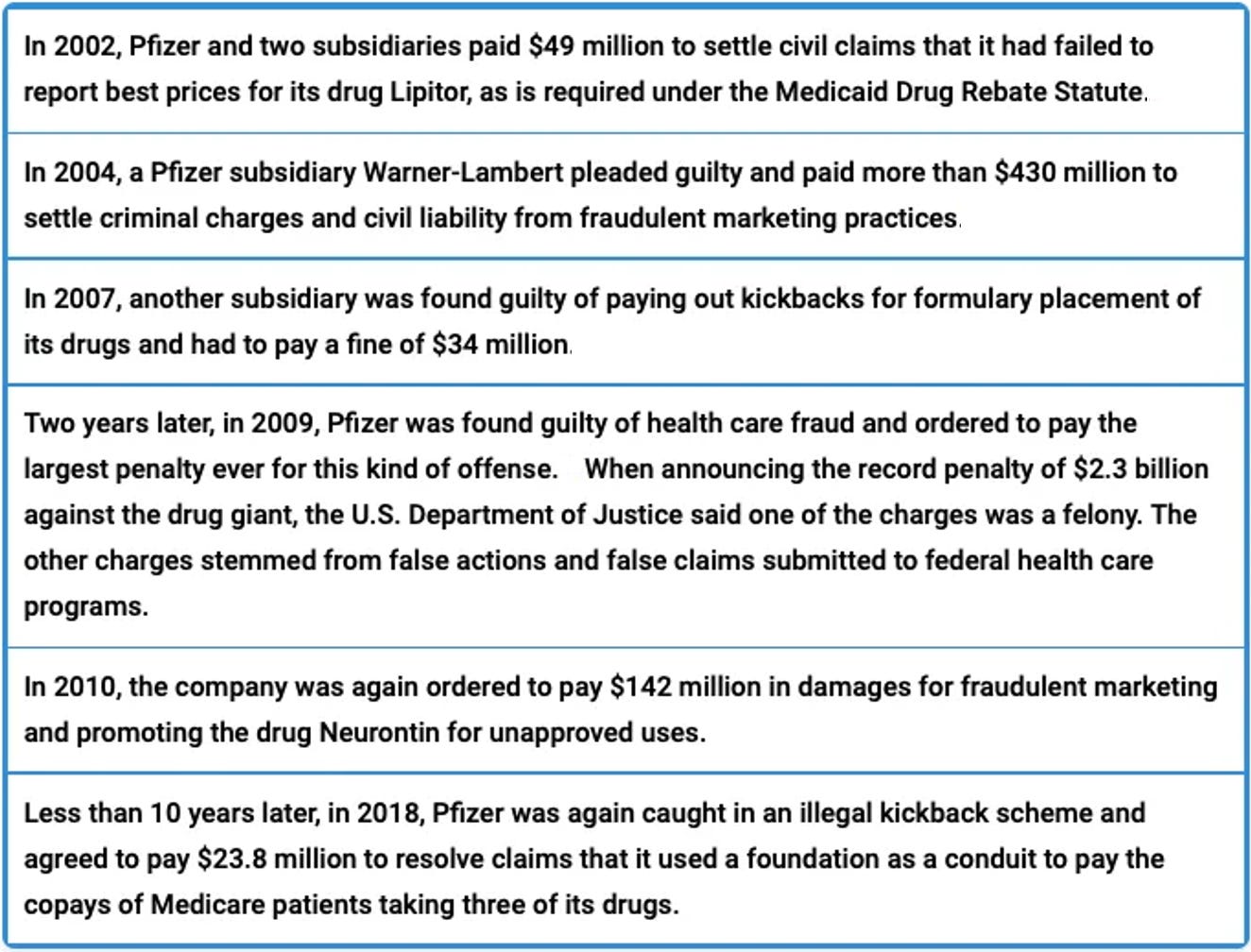
The 2.3 billion dollar settlement was for Bextra. Bextra was Pfizer’s version of Vioxx, and, like Vioxx, was aggressively promoted for off-label uses, and eventually was pulled from the market for causing too many fatal heart attacks and strokes (Bextra was pulled in 2005, Vioxx in 2004).
The whistleblower who helped initiate the lawsuit, John Kopchinski, was a sales rep who was recruited by Pfizer’s CEO during his early 1990s acquisition of veterans. In early 2003, Kopchinski raised concerns over Bextra, and instead of being listened to, was summarily dismissed from the company and left jobless. A few excerpts from his story mirror the experiences of many other Pfizer whistleblowers:
“Particularly in pharma, it’s no secret that it’s an industry that can blackball former employees,” Kelton [Kopchinski’s attorney] said, “so the reward is important both to encourage people to step forward and to recognize that their contributions are huge.”
[Less than a year after being hired by Pfizer], Kopchinski was selling the epilepsy drug Neurontin when a previous whistleblower’s suit was unveiled against [Pfizer] over similar illegal promotion tactics that led to stiff penalties and a form of corporate probation [Pfizer has been repeatedly forced to sign a corporate integrity agreements with the U.S. government].
At the time, [Kopchinski] was told by managers that the Neurontin suit would be in the news and any physicians who asked questions should be told it was just complaints from a disgruntled former employee, Kopchinski said. Ironically, after filing the Bextra suit, “I was the disgruntled former employee,” he said. [
In both the Bextra case (detailed here) and the Neurontin case (detailed here), Pfizer followed a fairly similar pattern. They aggressively pushed their sales reps to prescribe as many drugs as possible (and provided bonuses for doing so), and they used an elaborate scheme of bribes to incentivize doctors to prescribe these drugs. Most of the uses Pfizer made up for the drugs had nothing to do with the drug’s intended use, and in many cases, these reckless uses were quite dangerous to patients.
Note: Another drug in the same class as Bextra, Celebrex, was also aggressively promoted by Pfizer (and sold by reps like James Reidy). Instead of being pulled from the market, it received a black box warning from the FDA. Later in 2016, Pfizer was forced to pay 406 million dollars to shareholders because of the losses they incurred from Pfizer concealing the harms of Bextra and Celebrex.
Jamie Reidy
Most of the pharmaceutical employees who worked on the retail end of the business have come forward with similar stories of their sales culture. The below video, although not from Pfizer, gives one of my favorite windows into this world (I hope you liked the ending I added to it):
This circa 2000 clip shows how Pharma sales reps are trained behind the scenes. Like Pfizer, GSK aggressively and illegally promotes drugs (like this one) and has received billions in fines. I can't even imagine how much wilder the industry has become since this was filmed.
Jamie Reidy was one of the many veterans picked up in Pfizer’s recruitment drive for ex-military in the early 1990s, and his story mirrored what other former Pfizer representatives have told me—they were an ideal demographic because Pfizer wanted a pool of candidates who would follow corporate’s sales scripts and not deviate from them. Reidy eventually published his experiences within a comical memoir released while Rost was making waves in the national press (Rost likewise helped Reidy on the national PR front). Reidy’s self-deprecating memoir was later adapted into a popular romantic comedy, Love and Other Drugs, so his story is one of the better-known peeks inside Pfizer (it also resulted in him immediately being fired by the new pharmaceutical company employing him).
Since Pfizer established their dominance in the market through the success of their sales division, I was quite interested to hear Reidy’s perspective on the the nuts and bolts of the operation.
Pfizer being Pfizer, however, it didn’t have to resort to trolling college campuses; Pfizer could pick and choose its sales force from candidates who got their start at other companies.
Pfizer’s approach was built around utilizing algorithms their marketing research team had developed, which identified the most effective scripts for each stage of the sales process (from opening the encounter through closing the deal). Pfizer essentially practiced evidence-based sales and had the results to validate their model. Many of these scripts are quite interesting to read through. Each illustrates how each pharmaceutical company would twist the data to support their drug, and how much of a doctor’s education and comprehension of the drugs they prescribed resulted from what the sales reps primed them to focus on (note: so much of human behavior is explained by what people have been primed to focus on).
Pfizer’s model thus required inspiring zealotry and standardization in its salesforce (as Rost detailed in the first half of this series, Pfizer reps were well known for this tactic):
From Day One, people told us how great we were. “Pat yourselves on the back,” our first speaker said, “because you are the cream of the crop.” I had already noticed that our class did not lack confidence, and the knowing grins on people’s faces confirmed my perception.
“Any drug rep from any company will tell you that he left initial training thinking that his drugs were the best in the industry, such was the power of pharmaceutical brainwashing [I wonder if this also applies to Jordan Walker’s department]. Pfizer reps departed training with a “Pass me the Kool-Aid” conviction that not “only were our drugs the best in the industry, but also that our company was the best in the world. Doctors and competing reps alike routinely commented on a “Pfizer attitude,” a tangible vibe suggesting we were intrinsically better than any other salespeople. Interestingly, army trainees emerge from boot camp with a similar sense of indestructibility, an unshakable belief that there could not be a more prepared soldier on earth. The key to creating this self-confidence [bravado] in both arenas was the same: an endless repetition of messages and tasks [Note: Pfizer would also frequently tell reps in service about how wonderful Pfizer was].”
“The brainwashing was not limited to our view of ourselves, however. Rather, the Pfizer training staff instilled within us indelibly negative impressions of our competitors, creating a hatred for people we had yet to compete against, let alone meet”
“They lied. They cheated. Their women dressed slutty. They bought physicians’ love with extravagant dinners and golf at Pebble Beach, instead of earning it through ethical practices. (I later learned that every company told its reps that they did things the “right way,” while the other companies cheated.) ”
Although Pfizer had been repeatedly fined for criminal sales activity, I didn’t see anything within Reidy’s memoir that was clearly illegal. Much to the disdain of the sales reps, although headquarters was always pushing the reps to sell more, headquarters was also shutting down any plan reps implemented which was potentially illegal (bribes to prescribe or promoting a drug for uses it was not approved for—known as off-label marketing).
The only cases I found in his book where the sales reps employed external incentives to influence a physician to prescribe their drug was through utilizing their sex appeal (and sometimes seducing either the physician or their staff). However, unlike monetary bribes, this is nearly impossible to outlaw so it has never been made illegal.
At the time Viagra came out, because no reasonable treatments for erectile dysfunction existed, everyone was clamoring for it (to the point that Viagra samples were regularly stolen). Not surprisingly, it was soon sought out by individuals beyond those it had been approved for (old men with poor circulation impeding erections). As a result, some off-label marketing to women and younger men for increased sexual performance did eventually occur (even though Pfizer at the start told its reps not to do this, because the accelerated approval of the then-novel drug put them in a precarious position with the FDA).
In summary, I do not believe Reidy provided any concrete proof of illegal activity within Pfizer, so he is not technically a whistleblower. However, he did provide an invaluable window into the corporate culture of Pfizer which also helps put their behavior into context.
Note: Ever since its approval, a variety of side effects (including heart attacks, strokes, blindness, hearing loss, or melanoma) have been attributed to Viagra. As Reidy detailed, many of these were known from the start by Pfizer. Many lawsuits have been thus filed for these injuries. Unfortunately, the legal system rarely supports these types of lawsuits, so Pfizer (along with subsequent manufacturers of similar drugs) have been able to dodge most of them and settle the rest.
Allen Jones
I mention this story last because it is potentially the most important one in this series (and resulted in him being named whistleblower of the year in 2012). Jones initially worked at Pennsylvania’s Office of the Inspector General (PA’s OIG) for 5 years (1986-1991), retired to be closer to his family, and then returned 11 years later in 2002, once his situation changed.
When he returned, he was assigned to investigate PA’s chief pharmacist, who Jones found was managing an unregistered bank account into which Johnson and Johnson (J&J) was essentially depositing illegal bribes. Additionally, some of that money was then transferred to the Director of Texas’s Department of Mental Health and Mental Retardation. In return for these funds, state officials traveled across the country to promote switching large numbers of patients to J&J’s new antipsychotic medication (which cost ten times as much as other similar drugs, and frequently created significant side effects).
Jones reported the case to his boss, and was told to drop the case as it was “too political” to touch. Since Jones did not comply, he was taken off the case. Then in 2003, he found out that J&J’s bribery lobbying was successful and everyone in PA would soon be switched to J&J’s drugs, regardless of their medical needs or background. Given that many of the people subject to this edict cannot oppose it (e.g., prisoners with mental illnesses or the many children who are pushed into the state mental health system), there were significant ethical issues with allowing it to proceed, which led to Jones deciding to risk his livelihood to stop it.
Note: I know a few people in foster care who were forcefully medicated with psychiatric drugs and had terrible experiences from them. To appreciate the full human cost of this greedy industry’s initiative to push their dangerous anti-psychotics on children, please read this article.
Jones filed a first amendment suit to protect himself, reported what was happening to the New York Times, and then was fired. Jones then filed suit against PA and set off a series of lawsuits (some of which were pursued by state Attorney Generals) and J&J ultimately had to pay billions of dollars in fines for their conduct. PA’s state Pharmacist was also convicted, but I feel his ultimate punishment was relatively minor. His conviction, however, is important to the current story because he was convicted of taking bribes from J&J and Pfizer.
Like Pfizer and J&J, AstraZeneca has also been fined billions for off-label-marketing, bribing physicians to prescribe their drugs, and was involved in the initiative to bribe state officials to push these medications on mental health patients. This bribery was not exclusive to the United States either; these three companies are currently being tried in court for bribing terrorists within the Iraqi government to coerce their Ministry of Health into using their products, and a few years ago, AstraZeneca was fined for bribing state health care providers in Russia and China to push their products.I hold the opinion that once the corruption of this industry is understood (which will probably always exist because of how much money there is to be made in medicine), the best path forward is to prohibit mandating of their products. If a product is safe and effective, it will sell itself and does not need to be forced on people.Unfortunately, the systemic fraud within this industry regularly brings bad pharmaceuticals to market that are neither safe nor effective.
As the examples with the state psychiatric programs show, this is a longstanding issue. It is my hope that bringing the public’s attention to the unjustifiable COVID-19 vaccine mandates can help bring about critical changes for medical autonomy that are needed throughout medicine.
Note: Since Moderna is a much newer company, an equivalent track record does not exist for them. I also believe this accounts for why they had a much less elaborate system in place to gaslight the participants in their clinical trials compared to the other COVID-19 vaccine manufacturers.
Conclusion
Pfizer eventually got fed up with Rost humiliating them on national television. He was fired and entered a protracted legal battle with Pfizer that eventually concluded in 2013 with an undisclosed settlement. At the time this happened, Pfizer made a point to widely publicize his termination in the national media. In Rost’s own words:
There is no question in my mind that Pfizer's [illegal] termination of whistleblowers [highlighted through this article] sends chilling signals to honest employees within the company. The media campaign they unleashed when they fired me served the same purpose. Pfizer’s outrage was apparent.
I hope that this article has made the case that Pfizer has a culture of corruption and a sociopathic leadership that has absolutely no problem with harming people or breaking the law to drive up sales. Assuming you accept that premise, I would argue that that means Pfizer was probably the worst party that could have been given a blank check by the government for the purpose of forcing an extremely dangerous experimental vaccine gene therapy onto the American people. Just think—if Pfizer already was that bad with government oversight--how bad do you think they would be once the government actively conspired to conceal their criminal activity and the harms of their product?
Similarly, if we consider the plight of many of the recent whistleblowers like Brook, the degree to which the government has chosen to ignore their claims is truly incredible. Similarly, nine months ago I covered an investigation by one of the less corrupt agencies of the government into HHS’s COVID-19 response, where they essentially concluded corruption trumped sound scientific policy (because employees in each department confided this in private interviews).
One of the most interesting things I discovered in it was just how hostile the U.S. Health and Human Services department (HHS,e.g., the CDC, NIH, and FDA) was to whistleblowers. None of the typically required safeguards existed to support employees blowing the whistle, and when queried, officials in each department could not cite a specific reason for why they had never gotten around to creating those safeguards.
Additionally, most of the employees felt that their leadership was already aware of the issues (and to some extent complicit in them), and they feared retaliation if they complained. Not surprisingly, between 2010-2021, there were zero cases where misconduct was officially reported by an employee of the HHS, and when asked, officials in each department interpreted this as a sign that no problems requiring reporting existed.
Sadly, corruption is not unique to the pharmaceutical industry, and many of the experiences shared by the brave whistleblowers in this series are mirrored by those outside of the medical industry. As you might expect, Pfizer and many of the other pharmaceutical companies involved in the COVID-19 vaccines (along with many defense contractors and other members of the medical industrial complex), have lobbied aggressively to restrict the ability of whistleblowers to uncover and correct their misdeeds. For example, consider what they did at the end of 2021, a year after their vaccines had entered the market.
As I look at how things have transpired decade by decade, it never ceases to amaze me how much more corrupt our government (and media) have become in a relatively short period of time. At the same time though, I believe Team Humanity still wins, because the internet has made it impossible to prevent the general public from becoming aware of these misdeeds.
As I end this series, I would like to share one of Rost’s concluding remarks which, like many other things he has shared, is just as true now as it was twenty years ago:
I didn’t always think this way. I didn’t want to become a whistleblower. I didn’t want to write this book. But in the end, I had to; I just couldn’t let the crooks win. The fact that you have just read this book means—to me—that I have won my fight against an overpowering opponent.
I for one, decades later, am profoundly grateful for the odd quirks of fate that led Rost to speak out against Pfizer.
I hope this article has provided some valuable context to fully appreciate Jordan Walker’s previous remarks to Project Veritas and his new ones today:
What goes on inside Pfizer and the pharmaceutical industry is surreal, and I hope the window opened for you by these whistleblowers will allow you to draw your own conclusions about Pfizer’s culture and what really goes on behind the scenes. I admit I avoided discussing much of what jumped out to me from their testimonies (and those of whistleblowers from other pharmaceutical companies) since this series was already pushing the limit of how much people will read.
I thank each of you for the time you took to read this article and those who shared the series with the audience that needed to hear it.
Postscript: I meant to include this but completely forgot to. One of my colleagues occasionally saw a patient who was a vaccine sales rep for Pfizer that would actively boast about how often their entire family was vaccinated. In the middle of the vaccine roll-out, that patient showed up asking for a medical exemption from their vaccine.

Now that my piece on Exogenous Moral Orientation has accumulated many views and comments, I want to respond in a general way to the objections raised by my readership.
When you write an essay putting forth a Broad Theory of How Things Are, nobody will read it unless it has a lede that speaks to contemporary interests and a concrete focus on current events. That’s the only reason I opened with Bill Gates and his rumoured ambition to depopulate the earth. I ought to have anticipated that this would prove as much a distraction as an enticement. In answer to the many emails and comments taking issue with my statements here, I would observe that theories of Gates and the vaccines must be brought into alignment with several basic facts: Vaccination rates across Africa and the third world are truly dismal, Gates himself has repeatedly criticised the mRNA vaccines for their inability to stop transmission, and the earth’s population has continued to increase since the pandemic began, undaunted by all public health policies. 1 If the plan is indeed depopulation via the mass administration of shitty pharmaceuticals, we can take some solace in the boundless idiocy of our shadowy overlords.
Beyond those specifics, it is incredibly important to realise that the political order of the West is marked by affinities and proclivities; it tends in specific directions. In an attempt to make sense of pandemic policy, many try to find the single point of manipulation – the PCR test fraud, the false study that sabotaged hydroxychloroquine, or the key vaccinator responsible for steering early funding to BioNTech. You must widen your view to see that these are single plots in a much broader nexus of policies and scheming that all strive in the same direction, while lacking any single point of control or direction.
What is Bill Gates trying to do? Many will doubt that he really wishes “ to create a world where every person has the opportunity to live a healthy, productive life ,” but the inverse image of the man as an aspiring global depopulator will not convince very many people beyond our circles either. Like other philanthropists, Gates has very mundane and self-interested aims:
By attaching his name to initiatives that are already highly regarded – that the cultural system already prefers – he hopes to achieve broader relevance and transform his personal wealth into a form of cultural and political influence. This doesn’t mean that Gates isn’t bad or that he shouldn’t be stopped. It just means that he is a follower more than he is a leader, and that we shouldn’t expect this sad, weak, bloated man to explain very much.
I was pleased to see that some left-leaning readers of the plague chronicle happily identified with the exogenous moral orientation, more or less as I described it. They objected, however, that they didn’t recognise their own political preferences in the decisions of our elite at all.
It’s an old and extremely interesting political illusion, that for those on the left, something akin to a “corporate right” appears to be steering the world, while those on the right see the establishment as primarily leftward tending. Aware of this strange fact, both sides will often use words like “neoliberal” to characterise elite political orientation as something separate from or beyond the conventional political spectrum. The problem is that leftism is not well understood. It is actually a kind of ideological technology, optimised to displace a prior ruling aristocracy and seize control of institutions via alliances of opportunity with disadvantaged social groups. Appeals to economic justice and redistributive policies are simply a means of forming these alliances, which are then used to empower a new managerial elite. This doesn’t mean that many leftists aren’t totally sincere and committed to their vision of equality, but as in all political movements, it is the opportunists and the cynics who run the show. These kinds of people have no interest in any egalitarian utopia, were that even possible, and this gives rise to our optical illusion: From the left, the new elite, which consolidates power for its own purposes, seems to have an aura of “the right” about it, while those on the right are most sensitive to the leftist ideological tactics that brought this new elite to power.
But, that’s just leftism as an ideology. The EMO is a moral instinct prior to ideology, and it can fit any number of different ideological systems. The EMO operates as a taste or a preference, which returns specific answers to specific policy questions. These answers change easily depending upon the scope and the framing of a given problem, leading to a wealth of inconsistencies. If the choice is between the native population of a Western country and third-world immigrants, the EMO will demand that the third-worlders be favoured. If the choice is between reliable power generation in the third world and the environment, the EMO will demand that the environment be favoured. What is apparently very difficult to squeeze past the EMO, are things which look like pragmatic compromises, such as endeavouring to improve third-world conditions via conventional power plants. This path, even though it is the most promising both for the environment and for real people in the world, fails to satisfy the operative moral demands and is eschewed. 2 Contradictions like these are clues, which reveal that we’re dealing here not with any coherent agenda, but rather with moral instincts and unexamined preferences.
Various commenters insist on the reality, the urgency and even the existential crisis posed by climate change. In fact, I formulated these thoughts while reading climate change literature, and I think nothing reveals the reality of the EMO so clearly as this subject. Even if, for the sake of argument, we posit that all of the climate models are correct and that the earth is steadily warming as a result of human CO2 emissions, we still lack a good explanation for Western climate policies, which are only secondarily interested in reducing emissions, and which deploy CO2 primarily as a pretence to circumscribe human impact on the environment. German emissions would be substantially lower, had we invested the billions we put into wind and solar into nuclear power generation instead. In that case, we would have the capacity to scale heat pumps and electric vehicles without threatening to break the grid, confining emissions still further. Instead, Green policies effectively demand an indefinite, continued reliance on natural gas and coal, which is acceptable, because the danger of nuclear power in their minds is not so much the overhyped threat of another Chernobyl, as it is the very real prospect of enabling further civilisational and industrial expansion at the expense of “nature,” which the EMO cannot countenance.
Another clue that something is not quite right with climate change, is that, as an area of cultural and political anxiety, it exists only in the EMO thought-world. This is in contrast to other issues, which prompt varying responses in those with endogenous and exogenous moral inclinations. Consider the war in Ukraine. Those with a pronounced endogenous moral orientation will be sceptical of the conflict and demand that military resources be conserved for national defence. Those with a pronounced exogenous moral orientation will be more likely to appeal to abstract universals like democracy and demand empathy with out-group Ukrainians. 3 We would expect climate change, as an objective problem, to provoke endogenously oriented solutions, and we would expect these to be very extreme, given the alleged immediacy and gravity of the threat. If we are indeed on the brink of triggering a climate “tipping point” (the concept is far more controversial even within the halls of Science than you have been led to believe), limpwristed Paris Agreements would be the least of it. Major powers would be imposing industrial limits on their rivals via sanctions and threats, to reserve the remaining CO2 capacity of the atmosphere for themselves. But, we see nothing like this at all, which suggests that the cluster of prognostications, beliefs and prescriptions around climate change are themselves the exogenously oriented moral response to a totally separate issue, which I will leave my readers to ponder. 4
Finally, because many objected that I overestimate Gates’s sincerity, I’d like to emphasise that I’m not making any claims about the subjective, inner life of anybody. I’m merely trying to articulate the moral system that explains the actions and professed beliefs of philanthropists, policymakers and many ordinary people in the West. By encouraging elites to ally themselves with immigrants or other more endogenously oriented outsiders against their native populations, the EMO definitely has malicious effects. The depressing truth is that people will be inclined to buy into moral systems which benefit them in other ways, and it is very hard to know where sincerity ends and cynicism begins, or to what degree sincerity can ever be an excuse.
Footnotes:
-
The growth rate – which has been in long-term decline – decreased by a barely-perceptible 0.1% since 2020 . 1
-
Third-worlders are typically favoured only when this redounds to the disadvantage of westerners; they are generally disfavoured on environmental and human-impact questions. Pragmatic environmentalists who subscribe to the theory of demographic transition ought to support any means of improving third-world conditions, as even relatively modest environmental impacts here promise to lower the birth rate. Instead, they favour hugely increasing the environmental impact of millions of third-worlders via mass immigration to the developed West, while they perpetuate third-world poverty via things like unworkable energy leapfrogging schemes, thus (at least in their framework) ensuring that birth rates and mortality remain elevated.
Note that that the moral dynamic surrounding Covid – rooted particularly in a kind of hygiene purity mania – prevented pragmatic solutions to the pandemic in much the same way. The authors of the Great Barrington Declaration tried to sell their alternative to mass containment under the rubric of “focused protection,” but in fact it is better to say that their plan hinged on building natural immunity in the youngest and least vulnerable demographics via “focused exposure.” The moral instincts governing pandemic policy made accepting any infections impossible, even at the cost of higher mortality. 2 -
These are of course only two of various possible constellations. More endogenously oriented Americans, who want to expand American influence in the world or who hold specific anti-Russian animosities, may well find themselves on the Ukrainian side. The same goes some endogenously oriented Eastern Europeans, who perceive the war as a national threat. 3
-
This is true whatever you think about the empirical reality of claims that atmospheric CO2 from human industrial activity is responsible for some portion of industrial-age warming – a proposition I tend to accept in broad terms. 4

The following book represents an extraordinary historical achievement in the reporting of events in science and medicine.
It also appears to be a record of a great crime against humanity.
In 2022, the Pfizer documents, a tranche of 55,000 documents, many of them thousands of pages long, were released via a court order. This was due to a successful lawsuit by attorney Aaron Siri. The US Food and Drug Administration had asked the court to keep these documents hidden for 75 years — until after most of us alive now would be dead and gone.
Luckily, the court did not concur.
We at DailyClout.io, a website devoted to civic transparency, realized that the raw documents were impossible to cover in normal journalistic ways. One reason was the massive scope of the documentation. But another reason was that the documents are written for scientists and medical researchers, in language that only specialists in those fields could really understand properly or explain.
We sent out a call for expert volunteers from those fields on our own platforms, and we did so also on the video and podcast platform, War Room Pandemic, hosted by Stephen K. Bannon. A global audience thus recognized how important it was for an informed public — who had been harried, bullied, and “mandated” to receive Pfizer’s and Moderna’s mRNA injections in 2021-2022 — to understand what was really revealed inside of the Pfizer documents.
As a result of our calls for expert help, we received 2000, then 2500, and finally 3500 responses from volunteers, many of whom are experts in their fields. Biostatisticians, lab clinicians, pathologists, anesthesiologists, sports medicine physicians, cardiologists, research scientists, RNs, and many other related disciplines are represented among these decent, highly-skilled people who offered to read through these difficult, technical documents — pro bono, as a service to humanity (and out of respect as well, in many cases, for their own lifelong commitment to real science, real medicine, and truth in general). Many of them were not only published, peer-reviewed academic authors in their fields, but some were peer reviewers themselves. There was no way, with a group this distinguished in science and medicine doing the labor, that the interpretation of these documents could be dismissed as “fringe,” subjective, or as the work of “conspiracy theorists.”
Of course, managing a project in which 3500 highly trained specialists from all over the world work together virtually on unpacking and reporting on such a massive trove of material, would have been impossible for mere mortals.
At first, indeed, we did not know how to organize the thousands of specialists who offered their help.
Enter Amy Kelly, who is also a heroine of this story. She is a talented project manager, and now DailyClout’s COO; and she has a distinguished background in complex organizational projects in various fields.
Ms. Kelly managed, seemingly effortlessly, to organize the volunteers into six working teams, with subcommittees of expert readers. Under her extraordinary leadership, the thousands of specialists around the globe started to communicate with one another, share their findings, and draft their reports. I trained the volunteers in writing for a general audience, and I also trained our DailyClout editors in editing what was often dense medical language, but with extremely important findings, into accessible reports that anyone with any level of education could follow and understand.
For all of us, but mostly for the volunteers and Ms. Kelly, the next year represented a Herculean effort to turn this material, that one of the most powerful companies in the world trusted would never be made public, into fifty readable reports sharing the most urgent headlines of all — the reports that are now in your hands.
You will see that the 46 reports document what may be a massive crime against humanity. You will see that Pfizer knew, as it appears, that the mRNA vaccines did not work. You will see that the ingredients, including lipid nanoparticles, in the mRNA injections bio-distributed throughout the body in a couple of days, accumulating in the liver, adrenals, spleen — and ovaries. You will see that Pfizer and the FDA knew that the injections damaged the hearts of minors — and yet waited months to inform the public. You will see that Pfizer sought to hire over a thousand new staffers simply to manage the flood of “adverse events” reports that they were receiving and that they anticipated receiving. You will see that 61 people died of stroke — half of the stroke adverse events being within a couple of days after injection — and that five people died of liver damage with, again, many of the liver damage adverse events sustained shortly after the injection. You will see neurological events, cardiac events, strokes, brain hemorrhages, and blood clots, lung clots and leg clots at massive scale. You will see that headaches, joint pain, and muscle pain are rampant as adverse events, though these are not disclosed as routine side effect warnings by our agencies.
Most seriously of all, you will see a 360-degree attack on human reproductive capability: with harms to sperm count, testes, sperm motility; harms to ovaries, menstrual cycles, placentas; you will see that over 80 per cent of the pregnancies in one section of the Pfizer documents ended in spontaneous abortion or miscarriage. You will see that 72 per cent of the adverse events in one section of the documents were in women, and that 16 percent of those were “reproductive disorders,” in Pfizer’s own words. You will see a dozen or more names for the ruination of the menstrual cycles of women and teenage girls. You will see that Pfizer defined “exposure” to the mRNA vaccine as including skin contact, inhalation and sexual contact, especially at the point of conception.
History has not yet concluded its assessment of what Pfizer — and the FDA, who were in custody of all of these documents — has done. We are at the very start of that assessment.
But to me it is clear that the following documents, written by impeccably skilled experts, and linked to primary sources, show that a crime has likely been committed against humanity that is unprecedented in its scale.
We owe the War Room/DailyClout Pfizer Documents Research Volunteers — some named, most of them unnamed — who labored for a year, and do so to this day, and for nothing more than the privilege of serving humanity, science, medicine and the actual truth — a tremendous debt. We thank Mr. Bannon and his team for so often supporting our call for experts and for helping us to announce the results in real time, as the reports came in. We thank all of the other news outlets, of all kinds, who risked reprisals from Big Pharma or even from the government — which recent lawsuits have shown allied with Big Pharma — who have also showcased the work of the Volunteers, in an effort truly to inform their viewers.
Please share this document with your loved ones if you also find it to be important.
Everyone by law deserves informed consent when it comes to medical interventions — it is actually a crime to withhold it (really many crimes appear to be represented here, but history will sort that out as well).
It has been a privilege to report on this team’s work, and to do all I can as CEO of DailyClout, to help sustain their, and the remarkable Ms. Kelly’s, work on humanity’s behalf.
Sincerely,
Dr. Naomi Wolf
CEO, DailyClout.io
March 21, 2023
Salem, Massachusetts

Note: This article is primarily a human story. The most important parts of this article are the videos (if you only have time to watch one, watch Maddie’s, below) that were compiled and edited for this article. The written details are just to provide the necessary context for the significance of their testimonies.
In the first part of this series, I discussed how the gross malfeasance observed by many in the COVID-19 vaccine trials did not come out of nowhere. Rather, it is yet one more occurrence in a chronic pattern of egregious conduct by the pharmaceutical industry, which has progressively worsened because there has not been the political will to address the growing corruption within the biomedical establishment.
There, I focused upon the events within the human papillomavirus (HPV) vaccine trials (and the subsequent red flags which emerged after they entered the market), because many at the time had difficulty believing something like that could even happen and it was possible to sweep the issue under the rug, since the vaccines were only targeted on one segment of the population—women. Now, not only has the exact same thing happened (to a very eerie degree) with the COVID vaccines across the globe, but what is happening now is even worse than what happened less than a decade ago.
The best metaphor I have come up with to describe what I’ve observed in the pharmaceutical clinical trial process is that enrolling in one is akin to entering an abusive relationship. The abuser will initially flatter you and promise you one thing after another in return for your consent to enter their web of deception. Then, once they have you, they will break each promise they made, gradually treating you worse and worse, and gaslight ing you into believing that those issues are not really happening. Finally, once they no longer need you, they will discard you and leave you to pick up the pieces (which is often almost impossible if you have a life-changing medical injury).
Thanks for reading The Forgotten Side of Medicine! Subscribe for free to receive new posts and support my work.
In the previous article , I introduced the concept of two different types of scientific fraud:
- Soft fraud is when the data is presented misleadingly to propose a conclusion that's not supported by the data, or some of the data is intentionally omitted (e.g., you do not publish an incriminating study or you find a way to reclassify an adverse event so it does not show up in the final clinical trial report).
- Hard fraud is when the data itself is just fabricated.
While many are comfortable with committing "soft” fraud, very few will commit “hard” fraud (although this cannot necessarily be said of India or China ). Instead, most of the fraud we encounter is soft fraud (e.g., this characterizes many of the studies used to try to debunk hydroxychloroquine in the treatment of COVID-19). This, in turn, makes it possible for outside investigators (e.g., this community) to read between the lines, identify what actually happened, and determine what the results of a given study should have been, had it not been twisted to provide the results desired by its sponsor.
Conversely, I believe that the general reluctance to commit hard fraud exists because it crosses a line that even the fairly corrupt academic and legal systems still stand behind. However, we frequently see things that come quite close to that line, such as dishonest researchers altering a trial midway through so it arrives at the needed results. Fauci, for example, did this repeatedly with remdesivir to get it onto the market, and similarly, the COVID-19 vaccine manufacturers like Pfizer ended their previously promised long-term placebo groups once they got their emergency-use authorizations (which should have required that long-term follow-up), so the long-term side effects of these vaccines could never be assessed.
Note: Although you can conceal most things by manipulating clinical trials, the one thing that is very difficult to hide is the total number of deaths (as they cannot be reclassified to something else). When Pfizer prematurely ended their trial at 6 months, more people had died in the vaccine group than the placebo group (and I suspect that this would have further worsened with time). The report disclosing this inconvenient fact (which destroyed the entire rationale for vaccine mandates) was released over a year ago .
Much of modern (industry-sponsored) science is designed to conceal things that would create problems for those sponsoring the science. Similarly, an ethos has been installed within our culture to doubt our own observations, and instead defer to the evidence-based scientific consensus, as the former, but not the latter is allegedly highly susceptible to biases that invalidate its conclusions. I disagree with this, and would argue that important things can often only be discerned by perceptive anecdotal observations.
Many organized religions throughout history have sought to control their populations by monopolizing the truth, and modern science is no different, monopolizing the evidence so that only a costly industry narrative can constitute "truth.” All of this is why we repeatedly see situations where someone has an undeniable medical injury, and afterwards, every professional they talk to tells them the injury could not have possibly been linked to the medication because there is “ no evidence ” it could have happened (also known as medical gaslighting ).
With the COVID-19 vaccines, we have seen alarming evidence of their harm across the board. For example, so many people are being harmed that VAERS has received more serious adverse events from the COVID vaccines than all other vaccines in history-- 28% of Americans know someone whom they believe the vaccines killedThe life insurance industry shows an unprecedented spike in deaths amongst working-age Americans following workplace-mandated vaccines being forced upon them. However, all of these safety signals are being ignored and dismissed as erroneous products of cognitive biases because they don’t meet the elusive bar for “evidence.”
Our current society has been conditioned to worship “evidence-based” science, and believes that it should be the sole arbiter of truth. One of the core tenets of evidence-based medicine is that the best available evidence should be used to inform clinical decisions. This is now widely interpreted to mean that large randomized controlled trials (RCTs) or clinical guidelines produced by committees of ( often corrupt ) experts are the “best” forms of evidence, and thus are the only things allowed to inform clinical decisions.
One of my largest disagreements with this dogma occurs when a situation arises where observations suggest something inconvenient to commercial interests, but the question at hand has not been formally assessed by large RCTs. The observations are summarily dismissed because “there is no evidence” for them. In these cases, I believe that the more limited data point (e.g., a series of similar clinical cases) constitutes the best available evidence, and should be treated as such until more comprehensive evidence is arrived at through a clinical study.
Much of my success as a clinician has arisen from utilizing more “limited” forms of evidence to inform my clinical decisions rather than waiting for an RCT (which may take years to be done) to settle the question—unfortunately many doctors become paralyzed and cannot act unless they have something like that to back them up. In contrast, if you read medical journals from earlier eras, physicians regularly made remarkable discoveries utilizing inductive reasoning, which is why I frequently study those ancient documents.
Overall, I believe there are three major issues with relying excessively upon RCTs:
-
The first, summarized in this essay by Harvey Risch, is that the value of (perfect) RCTs is heavily over-emphasized. In my eyes, most individuals who fixate on RCTs view an investigation being randomized and controlled as a necessary box to check off, rather than (like Risch) actually understanding what it entails from a statistical perspective.
-
Secondly, if the magnitude of an effect is small (e.g., this drug might reduce your risk of a heart attack years down the road by 5%), it takes an elaborate and costly trial to detect that faint effect, and it is very likely that you will have a greater chance of being harmed by a side effect than benefiting from the drug. Conversely, if the effect is large (e.g., shooting someone with a gun typically kills them), you don’t need an elaborate trial to detect the effect; a very small one will suffice to identify it. I subscribe to the belief that many useful medical interventions have a large enough magnitude of effect that it is not necessary to do complex testing to tease out their benefits.
-
The third point is that large RCTs are extremely expensive to conduct (meaning that only industry and occasionally vested interests within the government can fund them, which is why many therapies I stand behind have never been able to achieve this gold standard in research performed for them). The rarely considered cost of doing an RCT frequently invalidates the entire RCT model, because study after study has shown that the financial interests of a study’s sponsor heavily influence its conclusion, and that influence is much greater than any benefit that can be obtained through randomization or controlling for the placebo effect.
Because of the “sponsor bias”, large studies need to have a way to arrive at a sponsor’s desired conclusion without committing hard scientific fraud. Over the years, a relatively consistent toolbox has evolved for committing soft scientific fraud, and those familiar with it were able to immediately recognize it being applied throughout the COVID-19 clinical trials
The COVID-19 Vaccine Trials
The essential purpose of the COVID-19 vaccine trials was to do the following:
-
Be completed in a much shorter time frame than normal so that the vaccines could make it to the market before the pandemic ended on its own (which is essentially what has happened in Africa where vaccines were never used ).
Note: The FDA also understood the urgency to open this long-term marketplace and waived a variety of oversights that would normally be required using the present “emergency” as the justification for doing so.
-
Come up with something that could be used to justify that the vaccines were “effective” so that the medical profession would wholeheartedly support and promote them.
-
Conceal any adverse reactions from the vaccines that would make the medical profession reluctant to recommend the vaccines, and, more importantly, ensure doctors would deny any harms they observed in patients during the rollout could be linked to the vaccine (as doctors acknowledging widespread injuries would destroy the public’s willingness to continue vaccinating).
Long before the vaccines entered the market, I started to see the signs that an elaborate publicity campaign was being put together to frame the vaccines as the miraculous “ solution ” to the horrific pandemic situation we were experiencing (which was largely self-inflicted). Once the vaccines became available, that publicity campaign kicked into high gear and became the most aggressive propaganda campaign we had ever witnessed in our lifetimes. I tried to cover some of the most insane examples here:
Not surprisingly, this scheme also led to the vaccine manufacturers having the audacity to use titles like “ Safety and Efficacy of the BNT162b2 [Pfizer] mRNA Covid-19 Vaccine ” for the publications of their trials . Simultaneously, we were hit with the same soundbite over and over “ well we had hoped the vaccines would be effective, but we never imagined they would be this effective .” My colleagues ate that up, and it became nearly impossible to provide any piece of evidence with which to challenge this modern-day miracle.
Problems With Pfizer’s Trials
_Note: I mostly critique Pfizer. This is not because Pfizer is the only bad actor. It’s because I’ve spent the majority of my time reviewing their work (I can’t read everything), and because Pfizer received full approval for their vaccine, it was possible to view many of their regulatory submissions through FOIAs (and their equivalents)_
When I read through the Pfizer trial , a few red flags jumped out at me:
-
The vaccines were never tested for preventing transmission, and based on their design and my knowledge of precisely how previous vaccines failed to prevent transmission , I did not believe you could take it on faith that the vaccine's efficacy in reducing symptoms translated to the benefit all my colleagues ultimately cared about (reducing the transmission of COVID-19).
-
The actual benefits provided by the vaccine were very small. You had to vaccinate 119 people to prevent one minor case of COVID-19 (e.g., a sore throat + a positive test), 2711 people to prevent one “severe” case of COVID-19, and since no deaths were prevented in the trial, well over 21,720 people needed to be vaccinated (21,720 is the total number who were vaccinated in the trial) to prevent a single death from COVID-19.
-
Most of the suspected adverse reactions to these vaccines did not appear to have been amongst the adverse events that were monitored (they were also unlikely to appear in the brief timespan of symptoms being monitored within this trial).
-
The adverse events that were reported were much higher than what has typically been reported in trials for other vaccines [e.g., 59% experienced fatigue after Pfizer's vaccine, whereas around 10-15% experience fatigue after an influenza vaccine].
-
The actual benefit that the vaccines provided was much less than these adverse events that were acknowledged within the trial report. Arkmedic did an excellent breakdown of it here .
-
The noteworthy adverse events about which I remembered reading in the online support groups I had joined in 2020 for vaccine trial participants were not accounted for in any of the trial reports I read (Pfizer included). I had joined these online groups because I was suspicious of the vaccines and felt that doing this would be the only way to find out what the pharmaceutical companies had actually done.
From looking at all of this, my immediate thought was “if this was the best they could do using every possible trick at their disposal to rearrange their data to paint a positive picture of the vaccines, just how bad was the actual trial data ?”
Unfortunately, my physician colleagues (who frequently lectured us on how to skeptically dissect scientific publications) were so enraptured by the “the vaccine is even more safe and effective than we imagined” meme, that all these points fell on deaf ears. Fortunately, some did notice these issues, and Peter Doshi published a series of editorials (summarized here ) in the British Medical Journal (BMJ - considered to be one of the top 5 medical journals in the world ) that explained why the design of the vaccine trials and the evidence for Pfizer’s vaccines was very poor, and could not justify an FDA approval. Sadly, his experience with his colleagues mirrored my own, and his points were almost entirely ignored by the medical profession.
One of Doshi’s many observations was that there were signs in the data that the trial was not blinded, and the entire benefit of the vaccine may have been due to a failure to test vaccinated individuals for COVID-19 (thus creating the illusion that vaccinated individuals were less likely to have laboratory-confirmed COVID-19).
Subsequently, a whistleblower, Brook Jackson , who helped run one of Pfizer’s clinical trials, came forward and testified to the following:
- The COVID-19 vaccine trial she participated in was run in a much more haphazard way than any others she had worked on throughout her career.
•The trial was not blinded, and protocols that should have been followed to ensure blinding were flagrantly violated.
-
Vaccinated individuals with COVID-19 were not being tested for COVID-19.
-
Adverse reactions in vaccinated individuals were not adequately recorded.
Due to a concern that this conduct would violate the FDA’s requirements for clinical trial sites, Brook alerted her superiors about what was happening so that these issues could be addressed. After her pleas repeatedly fell on deaf ears, she eventually notified the FDA directly. Although the FDA did not investigate her concerns, they appeared to have informed her employer, as Brook was terminated the same day.
Note: As detailed by Doshi , there has been a longstanding issue with the FDA providing insufficient oversight for clinical trial sites, and as a separate investigation into vaccine oversight revealed, it was suspected that their laxity in oversight would dramatically worsen during Operation Warp Speed, which was the partnership between the Departments of Health and Human Services (HHS) and Defense(DOD) aimed at helping to accelerate the development of a COVID-19 vaccine.
After these events transpired, Brook submitted her story to the BMJ who corroborated her allegations through documents she provided, and through other employees at the trial site. I would strongly recommend reading the BMJ’s investigation to understand exactly what happened there. Since her termination, Brook filed a whistleblower lawsuit against Pfizer which is presently in the federal courts.
Later, when I reviewed the events with Brook, one of the most interesting things I learned is that most of the data which is collected at clinical trial sites never even makes it to the FDA. Instead the FDA only receive a very small sample of it that is trusted to be representative of everything that occurs. I suspect this is one of the many reasons why the FDA could truthfully claim they had no knowledge any of this happened, although as this article shows they are clearly also culpable since they did not choose to pursue getting the reports for adverse events (like Maddie’s) they knew were happening.
In summary, as you can see from the above information, there was a real risk that soft fraud would occur during the clinical trials. However, unlike the many cases in which this has happened in the past, for the COVID-19 vaccine, we also had the unique opportunity to have numerous whistleblowers come forward and corroborate that this happened for the COVID-19 vaccines.
[

A Midwestern Doctor @MidwesternDoc
Whistleblowers are critical for righting the wrongs in government and healthcare. They always pay a steep price, but still would choose to do it again. Gøtzsche's presentation provides the best explanation I have ever seen on what drives the heroes we need now more than ever.
](https://twitter.com/MidwesternDoc/status/1609225914885476353)
The COVID-19 Vaccine Trial Strategy
Pfizer and Moderna knew quite early on (although exactly how early is a matter of speculation) that there were serious risks involved in using the mRNA spike protein platform for vaccination (this was also most likely the case for AstraZeneca and Johnson & Johnson with their spike protein vaccine). This left them in a bit of a bind; how could the vaccines they were committed to making for Operation Warp Speed be “safe” enough to win the vaccine race and get the market share they wanted?
As far as I can tell from reading the preclinical documents (e.g., this one ), this was initially accomplished by opting out of much of the safety testing on non-human subjects, which would normally be required before proceeding to human studies (e.g., Pfizer was allowed by regulators to exempt itself from testing for autoimmunity or cancer risks). I took this as a tacit admission that it was known that there were serious issues here (given that there were major concerns with these issues and they have since become some of the most common serious complications of the vaccines). In turn, they concluded that their best option was to never formally test for them so they could plausibly deny knowing that the issue existed (this is a common industry tactic) and claim that there was no evidence that the issue exists.
Once the human trials began, the goal shifted to doing everything possible to minimize the number of inevitable adverse events which occurred. This was essentially accomplished by:
-
Making it very difficult for trial subjects to report any complications from the vaccines except for a very narrow subset of symptoms that were not a major publicity issue for the vaccine manufacturers. This characterizes both the limited V-safe data (which was still incriminating enough that a lawsuit was needed to get it from the CDC) and the even more limited list of adverse reactions found within the main section of Pfizer’s clinical trial report [fever, headache, fatigue, chills, vomiting, diarrhea, muscle pain, joint pain, or use of a fever medication along with pain, redness, or swelling at the vaccination site]. Furthermore, all of these symptoms were only monitored for 7 days post- vaccination (many vaccine injuries do not occur within this brief window, which was a well known fact prior to the COVID-19 vaccines).
_Note: the more severe injuries in Pfizer’s study were reported in an extremely vague manner ( see page 9 ), which made it impossible to determine anything._
-
Aggressively reclassifying each serious complication as unrelated to the vaccines (typically by claiming it was in fact due to a pre-existing psychiatric condition or COVID-19).
-
Avoiding any type of long-term followup on patients which could provide incriminating safety data, regardless of prior commitments to do so.
Because of this strategy, the vaccine manufacturers could not acknowledge any complications that research participants experienced as being related to the vaccines. Instead, all they could do was gaslight the patients into believing that the injury was unrelated to the vaccine, and have healthcare providers collude to create the narrative that the injury was not related to vaccination.
One of the cruel complications of this approach was that it required reneging on the promises that were given to the trial subjects at the start of the research study—any medical complications they received would be covered (because providing any type of help would require acknowledging that there were potential complications from the vaccine). The one, possibly unanticipated, downside of choosing not to help with medical expenses accrued in the trial is that it could solicit the outrage necessary for trial participants to speak out publicly about what happened to them, and for the public to listen…which to some extent has now happened.
All of these potential issues were why the BMJ has repeatedly called for the raw data for the COVID-19 vaccine trials to be released. It is almost certain that the scant clinical trial data we have been provided by the pharmaceutical companies is highly misleading, and that lack of information makes it completely unethical to mandate the vaccines on the population. This is especially true because the lack of data acknowledging the injuries makes it impossible for those who are injured to receive any type of medical care or support (hence, why many providers are now labeling vaccine injuries as long-covid, because it represents the best shot they have of getting help).
The COVID-19 Vaccine Trial Participants
When you review these cases, it does appear that they were all coordinated as a very similar playbook was used on each participant. However, I believe this was more of an emergent phenomenon because very similar things to the approaches used here have occurred in the past. Much of what follows is déjà vu from Merck’s HPV vaccine trials, and to a lesser extent these examples also match what friends of mine experienced with complications from other pharmaceuticals that were already FDA approved (as doctors are often very resistant to believing drugs they prescribed could cause harm).
For example, many of the adverse events shown below were reclassified as being a complication of pre-existing psychiatric conditions, and this has been the default strategy for gaslighting patients throughout the history of medicine . I believe the new emphasis on reclassifying injuries as COVID-19 resulted from a climate of hysteria, where anything could be labeled as COVID-19 and there is enough of an overlap between spike protein injuries from COVID-19 to the vaccine itself, that it could be rationalized that many vaccine injuries were actually due to the virus.
Maddie’s story
To expand the market for the COVID-19 vaccines, a case needed to be made that they were safe and effective for children (who had for all practical purposes a 0% chance of dying from COVID-19). For this reason, we saw a variety of predatory advertisements such as this one from Pfizer:
An individual who was severely injured in the above trial has dedicated her life to making her story known around the world:

Much of the time that went into this article came from editing Maddie de Garay’s story on the Highwire into a shorter version (as I recognize that while the entire presentation is extremely compelling, far fewer people will watch a full episode—as you’d guess it was extremely challenging to decide which parts to cut out of it).
Because of how important I felt this story was for the world to see, I emailed it to Pierre Kory for him to share it (he has a lot more followers), and I would request that you both watch this and consider sharing it as well, because it has a really powerful message:
[
Pierre Kory, MD MPA @PierreKory
Pfizer's trial only vaccinated 1,131 children so a single serious injury would have made the vaccine too dangerous. Maddie's story shows just how far medicine will go to betray and gaslight patients who threaten its narrative. We may never know who else was swept under the rug.
](https://twitter.com/PierreKory/status/1613319015178330113)
Most of what is in this video should speak for itself. A few additional things I’d add though:
-
Maddie’s attitude is remarkable. I am genuinely amazed that she is not more bitter about her situation, especially given how healthy and active she was before her injury (it is incredibly difficult for people who have serious injuries to come to terms with what has happened to them, and accept that they can no longer do what they had previously been able to do). Instead, she is almost entirely focused on preventing others from also experiencing her nightmare.
-
One of the issues highlighted in the Real Anthony Fauci is that Fauci has developed a network of principal investigators (PIs) to conduct questionable research trials for his drugs.
-
There is absolutely no question that Maddie’s PI, Dr. Frenck, knew what her injury was the moment it started (as it had previously been reported in many adults), knew what it meant for Pfizer if the injury was acknowledged by the trial (given how few people were in the trial), and that he had enough influence to shape the medical process which Maddie received so that it would not be something that had to go in the clinical trial report. His choice to initiate this coverup resulted in necessary care (which could have prevented her paralysis) being delayed until it was too late, and he is directly responsible for what happened to Maddie.
-
The allergist that Maddie worked with who diagnosed her with a faux condition, Functional Neurological Disorder (FND) to conceal the adverse event, according to Open Payments (a required database for pharmaceutical payments to physicians), from 2015-2021, had received $652,650.65 for associated research funding (with the amount increasing year by year).
-
FND is an extremely disingenuous disease that is frequently used to gaslight patients who have received severe neurological injuries. I wrote much more about it here , including how neurologists lack the insight to recognize what they are doing when they authoritatively throw this diagnosis around.
-
The experience Maddie had at the hospital was awful, and to some extent surreal, but for length considerations, I cut it from the presentation. Amongst other things, Maddie became much worse after she was at the hospital (e.g., she lost her ability to walk), and believes it was due to her MRI. I periodically encounter people with complex issues who get much worse from MRIs (especially the COVID-19 vaccine injuries). I’ve seen a few explanations for this, and of those, the most likely (but not only) explanation is it being due to the MRI’s contrast agent. Gadolinium is quite toxic for some, but this toxicity is rarely considered in medicine.
-
Maddie was very fortunate to have a parent who was a nurse. Similar situations are even worse for those who have no direct experience in health care.
-
They also provided the information at the end of the episode for Maddie’s lifefunder .
Brianne’s story
[
A Midwestern Doctor @MidwesternDoc
Exactly what happened in the clinical trials is critical to uncover as they are the basis for the lie the vaccines are safe and all other evidence is "anecdotal." Dressen (and others she's found) were erased and left to fend for themselves once their reactions raised red flags.](https://twitter.com/MidwesternDoc/status/1613370463958212608)
Many of the key points that needed to be made are contained within the above clip (I put two different presentations together). The key points I had to edit out to shorten it were:
-
Brianne was actively communicating with the National Institute of Health (NIH) as part of a study for treating COVID-19 neurological injuries, which were repeatedly delayed by the NIH for political reasons (but was eventually published). In that study, they eventually settled on using intravenous immunoglobulin to treat the injury (which interestingly, also sometimes helps HPV vaccine injuries, but is also an expensive treatment requiring a large donor pool, and thus has limits to its scalability ). I wrote more about Brianne’s experience with the NIH and their study here .
-
Brianne founded an organization dedicated to helping COVID-19 vaccine injury victims. According to their organization (this was in response to Maddie’s story):

In the longer version of the above presentation, she mentions she and three other individuals injured in the clinical trials (each detailed in this article) all had their injuries classified as something innocuous to conceal them (e.g., Maddie’s injury was functional abdominal pain, Olivia’s T-cell lymphoma was lymphadenopathy). If I find out who the other 3 participants were, I will update the article to include them.
Note: The reason I now post tweets with videos throughout these articles is because Substack only allows videos from a few platforms to be embedded in articles (this matters because most people understandably won’t click through to outside videos). Of those platforms, Twitter is the only one that does not censor or delete controversial videos (I thought Vimeo worked as well, but a month and a half ago Vimeo deleted my entire channel).
Olivia’s story
Olivia’s story is the video at the top of this article (presented in that way due to its length) and in the Rumble video below:

Although her story is very similar to the others, there are a few important takeaway points from Olivia’s story which may not be immediately apparent.
First, for a variety of reasons detailed here, it’s often difficult for doctors to recognize subtle medical injuries unless they have been specifically trained to look for them . Instead, doctors tend to rationalize all of them as being due to psychiatric issues . What is unique about Olivia’s situation is that because everything that happened to her was so unusual, and most importantly, could be directly observed visually (so you could not deny it was happening), outside doctors were actually willing to acknowledge her injuries. Despite that, this is how Moderna’s PI treated her (clipped from the above video):
[
A Midwestern Doctor @MidwesternDoc
If you are injured in a vaccine clinical trial, they will deny your injury, not help you as promised, and not report it. This story is remarkable because Olivia had such strong evidence linking her injury to Moderna, outside doctors agreed, but even then, this is what happened](https://twitter.com/MidwesternDoc/status/1612625075022491648)
Nonetheless, despite it being unambiguous that her injury was due to the vaccine, Moderna did not pay for her medical care as promised, and did not report her injury. Additionally, the clinical trial site director said she would only be able to acknowledge that the cancer Olivia had was linked to the vaccine if “ more research emerged in the future linking it ” even though this happened at the trial that was supposed to determine if this could happen ( note: this example illustrates a common deficit in critical thinking that exists throughout my profession ).
Although her shoulder injury is alarming (and like Maddie, the physical therapy Olivia was forced to go through to “address” it should never have been conducted), the cancer she has is much worse. Based on her history, there is a very strong case that it was linked to her vaccination, and had this been presented in Moderna’s trial report, would have had huge implications for the many patients now developing cancers who are told they cannot possibly be related to the vaccine, and thus these victims are denied the support they need.
Unnamed Moderna Trial Participant’s Story
A while back, I was requested to review 865 vaccine injuries that were submitted in a survey to assess the plausibility thatthe deaths described were due to the vaccine. One of the reports caught my eye since it represented a critical incident that was not reported within Moderna’s trial report (see page 40 ), so I reached out to the doctor (who will remain unnamed) who submitted the report and had good reason to be knowledgeable of this patient’s history.
According to the doctor, the gentleman who passed away was part of the clinical trial at Research Atlanta that was paid for by Moderna. He developed atrial fibrillation after the vaccine, and approximately 3 months after vaccination, he was hospitalized (but never vented or sent to the ICU) at Grady Memorial Hospital (which is very close to the CDC).
At the hospital, he received a CT scan, which revealed blood clots in his lungs. At the time, no one was aware that the vaccine could cause blood clots (both Moderna and the CDC had insisted that the vaccine was safe, and had not revealed it was associated with blood clots). The blood clots were then assessed to have been due to metastatic cancer, as there was no other explanation for them, despite the fact that a full cancer workup was conducted which could not detect any signs of cancer in the patient. The doctor I corresponded with (who I deemed competent to assess this question) is certain that the patient did not have metastatic cancer.
The patient was then assessed to be terminally ill, discharged to hospice, and then died in hospice care (which may have been partly due to respiratory difficulties resulting from the opioids he was given for hospice). As you might expect, the clinical trial contacts were notified of what happened to this patient, but they ignored the report.
Augusto’s Story
Augusto was another clinical trial participant who was abused by Pfizer. Fortunately, he was a lawyer and did everything he could to hold them accountable.
The only direct summary I have found of Augusto’s experience can be found within this (shortened) interview (an article was also written documenting his experience here ):

Although Augusto had the same experience as everyone else (e.g., they tried to say his issues were due to psychological problems and his adverse event never ended up in Pfizer’s final clinical trial report), there were also some remarkable aspects of his case:
-
His hospitalization was initially documented by a senior specialist as an adverse reaction to a coronavirus vaccine (although as the previous examples have shown, this did not ultimately change the course of things).
-
In addition to the team erroneously reporting the hospitalization which Augusto had directly told them about, the PI who was supervising his case fabricated a medical record to claim Augusto had an anxiety disorder. His injury (a pericardial effusion suggestive of pericarditis) was attributed to COVID-19 (even though Augusto had a negative test) and anxiety (even though anxiety cannot to my knowledge cause a pericardial effusion).
-
The PI who was supervising his clinical trial site was also the lead author of Pfizer’s New England Journal of Medicine (NEJM) study . Augusto’s experience and the documentation he had to support the lead author's misconduct is most likely the strongest argument for NEJM retracting Pfizer’s pivotal vaccine study ( note: in addition to the erroneous COVID-19 studies mentioned here, the NEJM also previously published Merck’s highly questionable HPV vaccine study ).
-
Augusto obtained the record of another participant who died from a heart attack at the same hospital to which he was admitted, but was not registered in the final Pfizer clinical trial report.
-
Augusto formally complained to the Department of Justice about this clinical trial conduct, but the government decided to avoid addressing it, despite their conduct being unlawful.
Pfizer vs. Moderna
Although many things could be said about these cases (which I suspect also holds true for the other ones I am not yet familiar with), one of the things that stands out to me from these reports is the differences in how Pfizer and Moderna conducted their trials.
In Pfizer’s case, they had a robust apparatus in place to have a team of physicians immediately neutralize any claims that the vaccine could be harmful. However, in Moderna’s case, they just told the doctors involved that the events could not be related to the vaccine and most doctors took those claims at face value (as they did not want to believe the vaccine could be harmful). Moderna, in effect, succeeded through inaction (by not documenting injuries or paying compensation for medical care they were obligated to).
I suspect this difference in strategies was due to Moderna being a fledging pharmaceutical company without an apparatus like the one Pfizer had developed over decades. Fortunately for Moderna, their laid-back approach ended up working out just as well since the FDA just rubber-stamped both of their vaccines.
Regardless of the approach that was followed though, I hope this examination into their mutual research misconduct helps to explain how these “impossible to predict” side effects that were never detected in the “robust” clinical trials could have suddenly emerged once the vaccines entered the market.
Conclusion:
Typically, it is nearly impossible to identify clinical trial participants and attempt to re-create what happened within a clinical trial. Due to the diligent work of leaders in this area like Del Bigtree , Aaron Siri , and a few clinical trial participants being brave enough to speak out publicly, we have been able to establish that serious adverse events occurred in all of the spike protein-producing vaccine trials.
More importantly, it should be apparent by now that the FDA has deliberately ignored this misconduct and tried to sweep the known adverse events under the rug. Based on all of this, I can state with near certainty there are other significant adverse reactions that did not make it to the final clinical trial reports.
Note: The fact that news stories like the above (the HPV vaccine trial malfeasance was the focus of the previous article ) received mainstream coverage (e.g., ABC news ) a mere decade ago goes to show just how rapidly the censorship of the media has increased in recent years. It also highlights how consequential failing to report the adverse events from a clinical trial can be for everyone injured after the fact .
Although exactly what degree of underreporting research fraud has occurred will probably never be known unless a legal investigation interviews each participant, as the examples in this article demonstrate, what is already known demonstrates that the vaccines are both ineffective and too dangerous to have on the market. On a more human level, what was done to these trial participants was appalling and needs to be prosecuted, and in the future may even happen if it becomes necessary to restore the public’s willingness to participate in the clinical trials which our medical system depends upon.
A major challenge of politics is catering a message to different political tribes, as each one will support certain messages and vehemently reject others. Most of the work we have done on the vaccine issue has been targeted to further convince those who already have doubts about the vaccines or sway those in the middle (which now represents a large portion of America ). Very little work however has been directed to those who are already committed to the vaccines (since it is largely a lost cause to try to change their minds).
For a variety of reasons detailed in a recent article , I believe the message that has the best shot at reaching those already committed to the vaccines (and motivating congress and the courts to do something) is to prove that fraud was committed by the manufacturers. This is why I attempted to present some of the best evidence we have currently for that assertion here (that Pfizer did not report what is actually in their vaccines). An even more important part of proving that case is showing exactly what actually happened in the clinical trials.
My sincere hope is that this article will inspire others who participated in the trials to come forward, and it is something that can be cited when people (especially doctors) try to argue that the clinical trials proved that the vaccines were “ safe .” I also faintly hope that awareness of this issue can inspire congressional hearings (which did happen previously with the disastrous anthrax vaccines that were forced on the military ). Although I doubt it would ever happen, I believe that the best solution to all the issues outlined in this article is to give trial participants the legal right to sue pharmaceutical companies for compensation if the severe adverse reactions they experience are not included in the final trial report.
Because of the videos, this article was an enormous amount of work to put together. I sincerely believe these stories need to be heard, so if you take the time to listen to them and share the ones that speak to you with others, many would sincerely appreciate that.
Lastly, on a lighter note, one of the practices I occasionally do to calibrate my medical intuition is to guess which fortune cookie best fits each member of a group I am with and then see how accurate the pairings were once they are opened. Sometimes I also go a step further and guess what specific subject the future fortune will address. The one I got today tested as being directed at the readers of this article:
”A dose of adversity is often as needful as a dose of medicine.”

In this series, Paula Jardine examines how the Covid vaccine programme was conceived by US defence planners nearly 20 years ago as a 21st century ‘Manhattan Project’ for biodefence.
WHEN Dominic Cummings testified before Parliament in June 2021 and he was asked about the UK Covid Vaccine taskforce, he said: ‘What Bill Gates and people like that said to me and others at No 10 was, “You need to think of this much more like some of the classic programmes of the past – the Manhattan Project in World War Two or the Apollo programme – and build it all in parallel. In normal Government accounting terms, that is completely crazy, because if nothing works out you have spent literally billions building all these things up, and the end result is nothing – you get zero for it, it’s all waste.’
Gates is the promoter, facilitator and profiteer-in-chief of the great vaccine Manhattan Project but he certainly isn’t the originator of it. The call for a biosecurity Manhattan Project dates back to the George W Bush administration.
On July 11, 2019, a think tank called the Biodefence Commission held a panel discussion entitled A Manhattan Project for Biodefence: Taking Biological Threats off the Table. The objective was to ‘create a national, public-private research and development undertaking to defend the United States against biological threats’.
Dr Robert Kadlec, the Assistant Secretary for Preparedness and Response (ASPR) in the US Department of Health and Human Services (HSS) was a panellist. During the discussion Kadlec said, ‘It’s time to say “Go big, or go home” on this issue.’ Covid-19 gave him just the opportunity to implement this Manhattan Project as appears to have been intended.
Kadlec founded the Biodefense Commission in 2014 when he was a consultant to one of its donors, the vaccine manufacturer Emergent Biosolutions. The Hudson Institute, a think tank co-founded by Herman Kahn of the Rand Corporation, the pioneer of war gaming who was satirised as Dr Strangelove in Stanley Kubrick’s film of the same name, is the Commission’s fiscal sponsor.
On Wednesday December 4, 2019, the House Committee on Energy and Commerce held its annual hearing on US public health preparedness and response for seasonal and pandemic influenza. Testifying before it were Dr Anthony Fauci of the National Institute of Allergy and Infectious Diseases, Dr Nancy Messonnier from the Centers for Disease Control (CDC), Dr Peter Marks from the Food and Drug Administration (FDA) and Kadlec.
Seventy-six days earlier,on September 19, 2019, an Executive Order on Modernizing Influenza Vaccines in the United States to Promote National Security and Public Health had been signed by President Trump, directing the National Institutes of Health (NIH), the Biomedical Advanced Research and Development Authority (BARDA), the CDC and the FDA to ‘accelerate the adoption of improved influenza vaccine technologies’. The Departments of Health and Human Services and the Department of Defense were to propose a plan and a budget for this effort within 120 days, in other words, before January 17, 2020.
The White House said: ‘Unfortunately, many of the vaccines we use today are produced overseas, using time-consuming, egg-based technology, which limits their effectiveness and makes production too slow to effectively combat a potential deadly influenza pandemic.’
Fauci may be the best known of the four witnesses but Kadlec is by far the most consequential. Kadlec, a retired US Air Force Colonel, and former Director of Biosecurity Policy in the George W Bush Administration, is the principal architect of 21st century US biosecurity policy. He said in his testimony: ‘ASPR’s mission is to save lives and protect Americans from 21st century health security threats.’
As a member of Bush’s Homeland Security Council he drafted the 2004 National Biodefense Policy for the 21st Century. He was the instigator behind the 2004 Project Bioshield Act that created a strategic national stockpile of anthrax and smallpox vaccines (manufactured by his Biodefense Commission’s funders). In 2005, as staff director to Senator Richard Burr’s Subcommittee on Bioterrorism, hedrafted the 2006 Pandemics and All-Hazards Preparedness Act (PAHPA, pronounced ‘Papa’). This act created the Biomedical Advanced Research and Development Authority (BARDA) and the Assistant Secretary of Preparedness and Response (ASPR) position. The ASPR controls the national stockpile of smallpox and anthrax vaccines and otherpublic health emergency medical equipment such as ventilators. During emergencies this Assistant Secretary has expansive powers enabling him or her to act as the single point of control co-ordinating national response. Kadlec was confirmed as ASPRin August 2017 after being recommended to President Trump by Senator Burr.
At the December 4, 2019 meeting of the House Committee on Energy and Commerce, Kadlec was asked what his department was doing to enhance American manufacturing capacity. He said: ‘On the issue of vaccines alone, I think the key thing is, I can’t go into the particulars but we’re going to have an announcement here shortly that will indicate some investments domestically to expand some of our newer technologies for vaccine manufacturing and I think the key thing there is, we are actively pursuing this in accordance with the executive order.’
Fauci testified that pursuant to Trump’s executive order his agency, the National Institute for Allergy and Infectious Disease (NIAID), was conducting and supporting research into new platform technologies including mRNA. Fauci said: ‘State-of-the-art technologies could be used to develop universal influenza vaccines as well as improve the speed and agility of influenza vaccine manufacturing.’
When Kadlec wasasked what the benefits were to the American people of investing in platform technologies such as mRNA he said: ‘The availability of such platform-based approaches would transform national preparedness against currently known threats as well as newly emerging threats in the future.’ Citing theASPR/BARDA funded development of a Zika vaccine made using mRNA technology he went on: ‘This technology has promise as a rapid platform for a number of infectious diseases, including influenza and novel diseases that may emerge in the future.
The Zika vaccine he referred to was being developed by Moderna, the US-based mRNA gene-therapy biotech. It didn’t have an influenza vaccine in development but it was actively working with Fauci’s NIAID to develop a ‘jointly owned coronavirus vaccine’. A prototype of this vaccine was sent to Dr Ralph Baric, the leading coronavirus expert who has worked collaboratively with Dr Shi Zhenghli of the Wuhan Institute of Virology, for animal testing on December 17, 2019.
Moderna’s European rival BioNTechannounced in August 2018 that it was in collaboration with Pfizer todevelop an mRNA flu vaccine. It was aiming to move this from the preclinical stage to phase 1 trials by the end of 2020. Professor Dr Ugur Sahin, co-founder and CEO of BioNTech said: ‘A significant presence in infectious disease supports our goal of building a global immunotherapy company that provides more effective and precise immune-mediated approaches for the prevention and treatment of serious illnesses, such as the prevention of flu and the treatment of cancer.’
BioNTech diversified from developing cancer therapies – none of which was successfully licensed – into vaccines after a provision in a 2009EU directive intended to enable genetic engineered viruses to be used in vaccines was identified in 2016 and interpreted by them and others as a regulatory loophole enabling gene therapies directed at infectious diseases to circumvent the more stringent and onerous Advance Medicines Clinical Trials protocols. In 2020, this flu vaccine research was pivoted to Covid vaccine research.
Using this regulatory back door, both the UK Medicines and Healthcare Regulatory Agency (MHRA) and the European Medicines Agency (EMA) evaluated BioNTech’s mRNA Covid gene therapies as run-of-the-mill vaccines. The mRNA gene therapies contain no viruses; instead they genetically modify the recipient, reprogramming their cells to produce a protein from the virus that will stimulate their immune system to create a response against the virus, meaning the EU directive should not have been applicable.
During the launch of Coalition for Epidemic Preparedness Innovations (CEPI) at Davos in January 2017, Gates enthusiastically promoted mRNA vaccines. ‘Now there’s a new class of vaccine, DNA / RNA vaccine that we hope we can just change a small part of it, and so the manufacturing facility would already be there, the trials you would go through would be very quick. You would understand what end point, what correlate you want and so in an emergency, the regulators would understand what sort of protocol we’re going to use,’ said Gates.
‘With Ebola we had a scientific challenge that these platforms weren’t ready, we didn’t understand which country, what type of indemnity, and so there was a lot of fumbling around. It’s only by fixing those regulatory uncertainties and using these new platforms that we have a chance of getting that time to be less than a year.’
Gates’s foundation took an equity stake in BioNTech ahead of its October 2019 US stock market launch. When he was asked in 2017 about the danger of these platform vaccines making people less well, he said: ‘You are right that the safety threshold is really, really extremely high because we have to maintain the reputations of all the vaccines, convince parents in all these countries that these shots are really there to help your child out. Anything that you do to healthy people is going to have a tougher standard than, say, a new cancer drug, where if you don’t have the new drug, the outcome is going to be quite negative.’
This tougher standard was soon forgotten. The Pfizer/BioNTech product was pushed into use by the UK Medicines and Healthcare Regulatory Authority (MHRA) on December 2, 2020 using a ‘compassionate use’ mechanism called a Temporary Use Authorisation to bypass the European regulator during the last month that the UK was under European Union law. MHRA reviewed only a few hundred pages of summary data, not the full dossier.
The FDA has a pathway for accelerated approval of ‘vaccines licensed in other countries with competent regulatory authorities.’ p21 Emergency Use Authorisation of the Pfizer/BioNTech vaccine as provided for under the 2004 Project Bioshield Act quickly followed in the US on December 11, 2020 and the European Medicines Authority (EMA) fell into line on December 21. Kadlec’s long-desired Manhattan Project was now detonating.
Part 2 of this series will focus on Dr Robert Kadlec, the principal planner of the US’s War on Microbes and of this biosecurity ‘Manhattan Project’.
Bibi is by nature cautious – even timid. His radical ministers, however, are not, Alastair Crooke writes.
Michael Omer-Man writes: Almost exactly 10 years ago, a young star rising in the Likud party, spoke to an audience committed to the outright annexation of the occupied Palestinian territories, laying out his blueprint. A year later, this same speaker set out certain prerequisites to full annexation: Firstly, a shift in the way the Israeli public thinks about a ‘two-state solution’ for Palestine; and secondly, a radical recast of the legal system “that will allow us to take those steps on the ground … that advance sovereignty”.
What was reflected in this statement is the structural dichotomy inherent within the ‘idea’ of ‘Israel’: What then is ‘Israel’? One side holds that Israel was founded as a ‘balance’ between Jewishness and Democracy. The other says ‘nonsense’; it was always the establishment of Israel on the “Land of Israel”.
Ami Pedahzur, a political scientist studying the Israeli Right, explains that the religious Right “has always considered the Israeli Supreme Court to be an abomination”. He points out that the extremist Meir Kahane “once wrote extensively about the tension between Judaism and democracy and the need for a Sanhedrin [a biblical system of judges] instead of the extant Israeli judicial system”.
In Israel’s attempt to balance these opposing visions and interpretations of history, the Israeli Right sees the judiciary as deliberately having been tilted toward democracy (by one part of the Israeli élite). This simmering tension finally exploded with the 1995 Supreme Court claim that it possessed power of judicial review over Knesset (parliamentary) legislation deemed to be in conflict with Israel’s quasi-constitutional Basic Laws. (An Israeli constitution has been considered since 1949, but never actuated.)
Well, that ‘young star’ of 10 years ago – who asserted so forcefully “We cannot accept … a judicial system that is controlled by a radical leftist, post-Zionist minority that elects itself behind closed doors – dictating to us its own values – today is Israel’s Justice Minister, Yariv Levin.
And with time, Netanyahu has indeed already brought about that first prerequisite (outlined by Levin almost a decade ago): The Israeli public perspective on the two-state Olso formula is radically changed. Political support for that project hovers close to zero in the political sphere.
More than that, today’s Prime Minister, Netanyahu, explicitly shares the same ideology as Levin and his colleagues – namely that Jews have a right to settle in any, and all, parts of the ‘Land of Israel’; he also believes that the very survival of the Jewish people is dependent on the actuation of that divine obligation into practice.
Many on the Israeli Right, Omer-Man suggests, therefore see the Supreme Court as “the central impediment to their ability to fulfil their annexationist dreams, which for them are a combination of messianic and ideological commandments”.
They saw the 1995 Supreme Court ruling as ‘a coup’ that ushered in the judiciary’s supremacy over law and politics. This is a view that is hotly contested – to the point of near civil war – by those who advocate for democracy versus a strict Judaic vision of religious law.
From the perspective of the Right, Ariel Kahana notes that although
“they have continued to win time and again – but they have never held power in the true sense of the word. Through the judiciary, the bureaucracy, the defence establishment, academia, cultural elites, the media, and some of the economic wheelers and dealers, the Left’s doctrine continued to dominate Israel’s power foci. In fact, regardless of who the cabinet ministers were, the old guard has continued with its obstructionist insurgency”.
Today, however, the numbers are with the Right – and we are witnessing the Israeli Right’s counter-coup: a judicial ‘reform’ which would centralize power in the Knesset – precisely by dismantling the legal system’s current checks and balances.
Ostensibly this schism constitutes the crisis bringing hundreds of thousand Israelis on to the street. Prima Facie, in much of the media, at issue is who has the final word: the Knesset or the Supreme Court.
Or, is it? For, beneath the surface, unacknowledged and mostly unsaid, is something deeper: It is the conflict between Realpolitik versus Completion of the Zionist project. Put starkly, the Right says it’s clear: Without Judaism we have no identity; and no reason to be in this land.
The ‘less said’ fact is that much of the electorate actually agrees with the Right in principle, yet opposes the full annexation of the West Bank on pragmatic grounds: “They believe that the status quo of a “temporary” 55-plus-year military occupation is the more strategically prudent”.
“Formally [annexing West Bank] would make it too difficult to convince the world that Israel is not an apartheid regime in which half of the population — Palestinians — are denied basic democratic, civil, and human rights”.
That other unresolved contradiction (that of continuing occupation within ‘democracy’) is also submerged by the prevalent mantra of ‘Right wing Orbánism versus democracy’. Ahmad Tibi, an Palestinian member of the Knesset earlier has wryly noted: “Israel indeed is ‘Jewish and democratic’: It is democratic toward Jews – and Jewish toward Arabs”.
The mass of protestors gathered in Tel Aviv carefully choose to avoid this oxymoron (other than around the kitchen table) – as a Haaretz editorial a few days ago made clear: “Israel’s opposition is for Jews only”.
Thus, the crisis that some are warning could lead to civil war at its crux is that between one group – which is no longer content to wait for the right conditions to arrive to fulfil the Zionist dream of Jewish sovereignty over the entire Land of Israel – versus an outraged opposition that prefers sticking to the political tradition of buying time by “deciding not to decide”, Omer-Man underlines.
And although there are ‘moderates’ amongst the Likud lawmakers, their concerns are eclipsed by the exultant mood at their party’s base:
“Senior Likud officials, led by Netanyahu, have incited Likud voters against the legal system for years, and now the tiger is out of control. It has its trainer in its jaws and threatens to crush him if he makes concessions”.
The flames lick around Netanyahu’s feet. The U.S. wants quiet; It does not want a war with Iran. It does not want a new Palestinian Intifada – and will hold Netanyahu’s feet to the flames until he ‘controls’ his coalition allies and returns to an Hebraic ‘quietism’.
But he can’t. It’s not possible. Netanyahu is held limp in the tiger’s jaws. Events are out of his control.
A prominent member of Likud’s central committee told Haaretz this week:
“I don’t care if I have nothing to eat, if the army falls apart, if everything here is destroyed … The main thing is that they not humiliate us once again, and appoint Ashkenazi judges over us”.
The ‘second Israel’ genres have wailed against ‘the ten Ashkenazai judges’ who discredited their leader (Arye Dery), whilst breaking into a song of praise for the ‘only Sephardic judge’ who was sympathetic to Dery. Yes, the ethnic and tribal schisms form a further part of this crisis. (A bill that effectively would reverse the Supreme Court decision barring Dery from his ministerial position over previous corruption charges is currently making its way through the Knesset).
The appeal of Religious Zionism is often attributed to its growing strength amongst the young – particularly ultra-Orthodox men and traditional Mizrahi voters. What became abundantly clear and unexpected in recent weeks, however, is that the appeal of a racist such as Ben-Gvir, is spreading to the young secular left in Israel. Among young Israelis (ages 18 – 24), more than 70% identify today as Right.
Just to be clear: The Mizrahi ‘underclass’, together with the Settler Right, have ousted the ‘old’ Ashkenazi élite from their hold on power. They have waited many years for this moment; their numbers are there. Power has been rotated. The fuse to today’s particular crisis was lit long ago, not by Netanyahu, but by Ariel Sharon in 2001, with his entry to the Temple Mount (Haram al-Sharif).
Sharon had earlier perceived that a moment would arrive – with a weakened U.S. – when it might prove propitious for Israel to complete the Zionist project and seize all the ‘Land of Israel’. The plans for this venture have been incubating over two decades. Sharon lit the fuse – and Netanyahu duly took on the task of curating a constituency towards despising Oslo and the judicial system.
The project’s content is explicitly acknowledged: To annex the West Bank and to transfer any political rights of Palestinians remaining there to a new national state to the east of the River Jordan, on the site of what now is the Hashemite Kingdom of Jordan. In the confusion and violence which would accompany such a move, Palestinians would be ‘persuaded’ to migrate to the ‘other bank’. As Hussein Ibish warned two weeks ago:
“We’re getting awfully close to the point where the Israeli government, and even Israeli society, could countenance a big annexation – and even expulsion [of Palestinians] – done in the middle of an outbreak of violence, and it would be framed as a painful necessity,” Ibish said. Such a move, he added, would be justified “as the government saying ‘We’ve got to protect Israeli settlers – they are citizens too – and we can’t let this go on anymore. Therefore we have to annex and even expel Palestinians.’”
To be fair, the unspoken fear of many secular protesters in Israel today, is not just that of being politically deposed, and their secular lifestyle circumscribed by religious zealots (though that is a major driver to sentiment), but rather, by the unspoken fear that to implement such a radical project against the Palestinians would lead to Regional war.
And ‘that’ is far from an unreasonable fear.
So there are two existential fears: One, that survival of the Jewish people is contingent on fulfilling the obligation to establish ‘Israel’ as ordained; and two, that to implement the consequent exodus of the Palestinians would likely result in the demise of the Israeli State (through war).
Suddenly and unexpectedly, into this fraught situation – with Netanyahu buffeted by a whirlwind of external and internal pressures – arrived a bombshell: Netanyahu was stripped of his ace card – Iran. In Beijing, China had secretly orchestrated not just the resumption of diplomatic relations between Saudi Arabia and Iran, but laid down the framework for a regional security architecture.
This represents a nightmare for Washington and Netanyahu – particularly for the latter, however.
Since the early 1990s, Iran has served both these parties as the ‘bogey man’, by which to divert attention from Israel and the situation of the Palestinians. It has worked well, with the Europeans acting as enthusiastic collaborators in facilitating (or ‘mitigating’ – as they would see it), Israel’s ‘temporary’, 55-year occupation of the West Bank. The EU even financed it.
But now, that is blown away. Netanyahu may ‘huff and puff’ about Iran, but absent a Saudi and Gulf willingness to lend Arab legitimacy to any military action against Iran (with all the risks that entails), Netanyahu’ s ability to distract from the domestic crisis is severely limited. Any call to strike Iran’s nuclear facilities is an obvious non-starter in the light of the Iranian-Saudi rapprochement.
Netanyahu may not want a show-down with Team Biden, but that’s what is coming. Bibi is by nature cautious – even timid. His radical Ministers, however, are not.
They need a crisis (but only when the ‘prerequisites’ are all lined up). It is clear that the wholesale stripping of Palestinian rights, in tandem with the emasculation of the Supreme Court, is not a project that can be expected to quietly proceed in normal circumstances – especially in the present emotive state across the global sphere.
No doubt, the Israeli Right has been watching how the Lockdown ‘Emergency-crisis fear’ in Europe was used to mobilise a people to accept a compulsion and restrictions to life that in any other circumstance they would never rationally accept.
It won’t be a new pandemic emergency, of course, in the Israeli case. But the new Palestinian Authority-led ‘SWAT-squads’ arresting Palestinian resistance fighters in broad daylight is bringing the West Bank ‘pressure-cooker’ close to blow-out.
Ben Gvir may simply decide to follow in Sharon’s footsteps – to allow and participate in the Passover ceremony of sacrificing a lamb on Al-Aqsa (the Temple Mount) – as a symbol of the commitment to rebuild the ‘Third Temple’, permission for which, hitherto has always been denied.
So what happens next? It is impossible to predict. Will the Israeli military intervene? Will the U.S. intervene? Will one side back-down (unlikely says ex-Head of Israel’s National Security Council, Giora Eiland)? Yet even if the ‘Judicial reform’ is somehow halted, as one exasperated Israeli forecast, “Even if this time the attempt does not succeed, it’s likely that they [the Right] will try again in another two years, another five years, another 10 years. The struggle will be long and difficult, and no one can guarantee what the result will be.”
The Jewish radicals have waited decades to reach office. They have the numbers now, and are loath to let this window of opportunity slip their hands.
-

Both Sides in the Region Now See ‘Big War’ as Possible
Events in the Middle East have been moving fast -- a ‘decade of change’ has been compressed into barely a few months: A world-shaping Entente has been sealed between Putin and Xi Jinping; China has mediated an accord between Iran and Saudi Arabia. President Raisi will meet King Salman after Eid; serious ceasefire talks have begun in Yemen. China, and Russia, have persuaded Turkey and Saudi to rehabilitate President Assad; the Syrian FM has visited Riyadh. Saudi Arabia has shifted towards China; OPEC+ has shrunk crude supplies. And everywhere from the Global South to the Middle East, the US dollar as a trading currency is being dropped in favour of national currencies.
A new paradigm is consolidating.
At the geo-political plane, the humpty-dumpty of western hegemony in the Region has fallen from the wall and lies shattered on the ground. All the ‘king’s (neo-con) men’ will not put humpty together again.
And, at another higher plane, an axis of voices across the region (on Al-Quds day) spoke compellingly, and with one united voice, that the Israeli ‘egg’ had better be careful, lest it fall and break, too.
The Israeli security establishment -- albeit in coded terms -- sees the prospect in a matching dark vein. Moshe Yaalon, a former defence minister, recently said that the ‘radicals’ within the Israeli government want a ‘big war’; and when "Israel" wants a war, it usually gets one; and that war will come on the back of the Palestinian issue, Yaalon suggested. ‘Coincidentally’, Israeli military Intelligence says the same: chances of ‘real war’ this coming year will spike.
Put simply, events in "Israel" are no longer in any one person’s ‘control’. The ‘newly’ empowered forces of Settler Zionist zealotry and of the religious Right to enact ‘Israel’ on the ‘Land of Israel’ are not about to ‘vanish’ the scene. They are pursuing no rational Enlightenment geo-political project, but the ‘Will of Yahweh’. And that constitutes an altogether different dynamic.
The Jewish radicals have waited decades to reach office. They have the numbers now, and are loath to let this window of opportunity slip their hands.
The US is putting enormous pressure on PM, Netanyahu, to abandon the Judicial ‘Reform’, which however constitutes the key-stone undergirding the whole ‘Land of Israel’ edifice: A project that is predicated upon ‘re-taking’ all of the West Bank from Palestinian ‘hands’. An enterprise that has the potential to shake the region to its very core -- and to trigger war.
It is an enterprise into which, the Israeli Right suspects, and the Supreme Court very well could insert a ‘wrench’. And they would be right.
President Biden however, needs a Middle East ‘conflict’ on top of the war in Ukraine, at this juncture, like a ‘hole in the head’. Former PM Sharon was prescient some two decades ago in foreseeing that US power in the Region would wane and that the US ultimately would prove powerless to block "Israel" from ‘seizing’ the biblical Land of "Israel". That insight probably has become actualised in this precise ‘moment’.
It is possible of course that Netanyahu will try to back down. The PM often has preferred caution. But realistically, can he retreat?
He is hostage to his coalition partners – should he wish to avoid jail – from which only his present government line-up can shield him. Absent that protection, court proceedings inevitably will result. There is no sign of other coalition partners willing to partner with Netanyahu -- almost at any price.
It is not difficult to understand the origins to the radical Mizrahi intransigence over the Supreme Court. Those favouring a Jewish state, rather than a (secular) balanced ‘democratic’ state, have the numbers. They had them in the 2019 election cycle. The Haredim, the national-religious, and Mizrahim should have had enough votes to secure 61 Knesset seats (a majority).
But over the course of four election campaigns, the ‘Right’ failed to materialise their majority -- as the Palestinian Arabs Knesset members entered the coalition-forming game to block the Right (which includes the Mizrahim) from capitalising on their numerical superiority.
Minister Smotrich wrote at the time in a Facebook post that were this situation to persist, the Right would forever remain a minority.
It is the desire for ensuring the majority achieves power that lies behind the agenda to neuter the Supreme Court and expel Arab parties from the Knesset. Then -- and only then -- can the Ashkenazi secular-liberal Establishment be overcome (in this perspective), and a Jewish State on the biblical Land of "Israel" be instantiated.
If that State also happens to be ‘democratic’, that’s okay -- but any democratic attribute would be entirely subsidiary to its ‘Jewishness’.
Most sane people believe that the burden of proving safety should lie on the party conducting a questionable action, rather than their victim. For example, if a criminal shot someone, the prosecution would not be required to prove that the victim’s sudden death after the gunshot wound was not just a spontaneous coincidence, a result of extreme stress from the situation, or due to a pre-existing medical condition.
Unfortunately, the pharmaceutical industry has been able to establish a special type of privilege within the legal system which has made it very difficult to demonstrate that vaccines (along with many other pharmaceuticals) can ever be at fault for anything. Because of this, we recently had a flood of experimental vaccines mandated upon the population, which were never tested for safety (despite many serious concerns with their design), whose (likely fraudulent) clinical trial data was never made accessible to the public.
We then had, as far as I know, the most aggressive propaganda campaign in history, and I watched the majority of my colleagues lose the ability to recognize any problems related to the vaccines. Instead, they developed an almost surreal religious devotion to the coming salvation of the vaccines becoming available.
Once the vaccines entered the market, a variety of red flags began going off indicating that these vaccines were killing people, and rather than address these concerns, the government—in concert with the media—chose to deny any of this was occurring. Instead they mandated the vaccines upon the entire population. I was understandably worried that the vaccines would cause problems and tried to do my part to head this off in 2020, but I did not expect anything on the scale of what we have encountered since then.
I personally became involved in all of this because soon after the vaccines entered the market, I began to have many friends and patients reach out to ask me if the vaccine could kill as someone they knew had had a tragic sudden death after vaccination. Once the magnitude of the problem dawned on me, I realized that even though my available options were limited, I could at least do my best to document each case sent my way so that someone would bear witness to what had happened. Otherwise, the dead had no voice. Beyond knowing I had a duty to compile this list however, I was not sure what to do with it. Later after someone kindly helped launch this Substack, I decided to post it, it ended up being seen by a lot of people…and that is how I ended up writing here.
Because of how long it took to verify each case, I realized that I had to end it a year in (at which point I knew of 45 individuals who had either critical or fatal injuries of a similar nature in close proximity to vaccination). Since that time, I still continue to hear reports I periodically document and discuss.
For example, a good friend is a nurse in a cardiac unit and has told me many of the patients she sees now with heart failure are much younger than they were a few years ago. I previously advised her against getting the vaccine due to her history of rheumatic fever (a condition where the immune system attacks and damages part of the heart). This was because I had noticed both COVID-19 and especially its vaccine seemed to cause inflammatory flares at previous sites of injuries or inflammation (Lyme is also known for doing this). The vaccine also has a remarkably high rate of exacerbating pre-existing autoimmune conditions—such as the 24.2% rate found in a recent Israeli survey which is comparable to what a few colleagues have observed, and I suspect exacerbation of preexisting inflammation within the circulatory system, like what this study of 566 patients found, is a key mechanism behind vaccine deaths.
A month ago, the nurse informed me that she had decided to vaccinate and had subsequently developed a heart condition. Additionally, she shared that the same had also happened to her mother following vaccination and that her sibling's partner is suffering longterm complication from a large stroke that immediately followed receiving a booster.
Looking back on it, the thing I found the most disappointing about my own documentation project was that once it went viral, it should have triggered the drug regulators evaluating the vaccines to take preventative action. Instead, due to the meticulously planned campaign of mass censorship that we all found ourselves in, more red flags than I can count were ignored by the “very rigorous” vaccination surveillance systems that were allegedly ensuring there were no safety issues with these vaccines.
Because of the immense power behind the medical-industrial complex, those debating this program have been stuck fighting an uphill battle. However, despite the immense degree of corruption, withholding of critical data, and censorship, these vaccines are dangerous enough that more and more evidence is nonetheless emerging of their danger, and the public is beginning to recognize it (e.g., consider how resistant the public has been to get COVID boosters). The previous article here discusses polling that shows this appears to be happening:
We Now Have A Clear Estimate Of The Rate Of Vaccine Injuries
Throughout my entire life, I’ve always found that trying to argue against Big Business is like fighting with one or both hands tied behind your back because large industries can always co-opt and buy out every authoritative source on the subject, and then censor any inconvenient facts that still persist. This is an immensely challenging situation.
Immediately after it was published, I was informed by a reader that possibly the most important dataset over the last two years was released today. For those interested, much of the context for today’s article can be found in the article above.
Thanks for reading The Forgotten Side of Medicine! Subscribe for free to receive new posts and support my work.
German Data
One of the depressing realizations one gains from studying the evidence-based literature is discovering how many issues exist within it and how difficult it is to know which data sources can be trusted. One of my favorite authors, Dr. Malcom Kendrick, devoted a book to addressing this subject and shared a pertinent anecdote for today’s events:
“In truth, the figures on vaccine damage are exceedingly difficult to analyse, because causality is very difficult to prove on a case by case basis. However, when it comes to negative findings I always like to go to Germany. It has been demonstrated many times that the Germans are the most likely to report negative findings accurately. Yes I know, terrible racial stereotyping, but a fact is a fact. What do the Germans have to say on the matter?
“Between 1978 and 1993 approx. 13,500 cases of undesired effects resulting from medications for vaccinations was reported to the Paul Ehrlich-Institute [PEI]…the majority was reported by the pharmaceutical industry. In 40% [5,400] of these cases the complications were severe, 10% [1,350] pertained to fatalities on account of effects.”
Additionally, as I learned from Kendrick, since early 2001, the federal infection protection law has mandated that specific severe vaccine injuries be immediately reported directly to the PEI (Germany’s equivalent of the FDA for vaccines and biologics). The German’s list of reportable injuries is much broader than what I have seen acknowledged by many other countries (e.g., those which are possible to receive compensation for within the United States) and includes the previously discussed complications of DPT along with many of the reactions typically associated with the COVID-19 vaccines. However, while that historical trend exists, Germany has not been one of the best countries for reporting COVID vaccine injuries (which I suspect is due to the political direction their government has moved in).
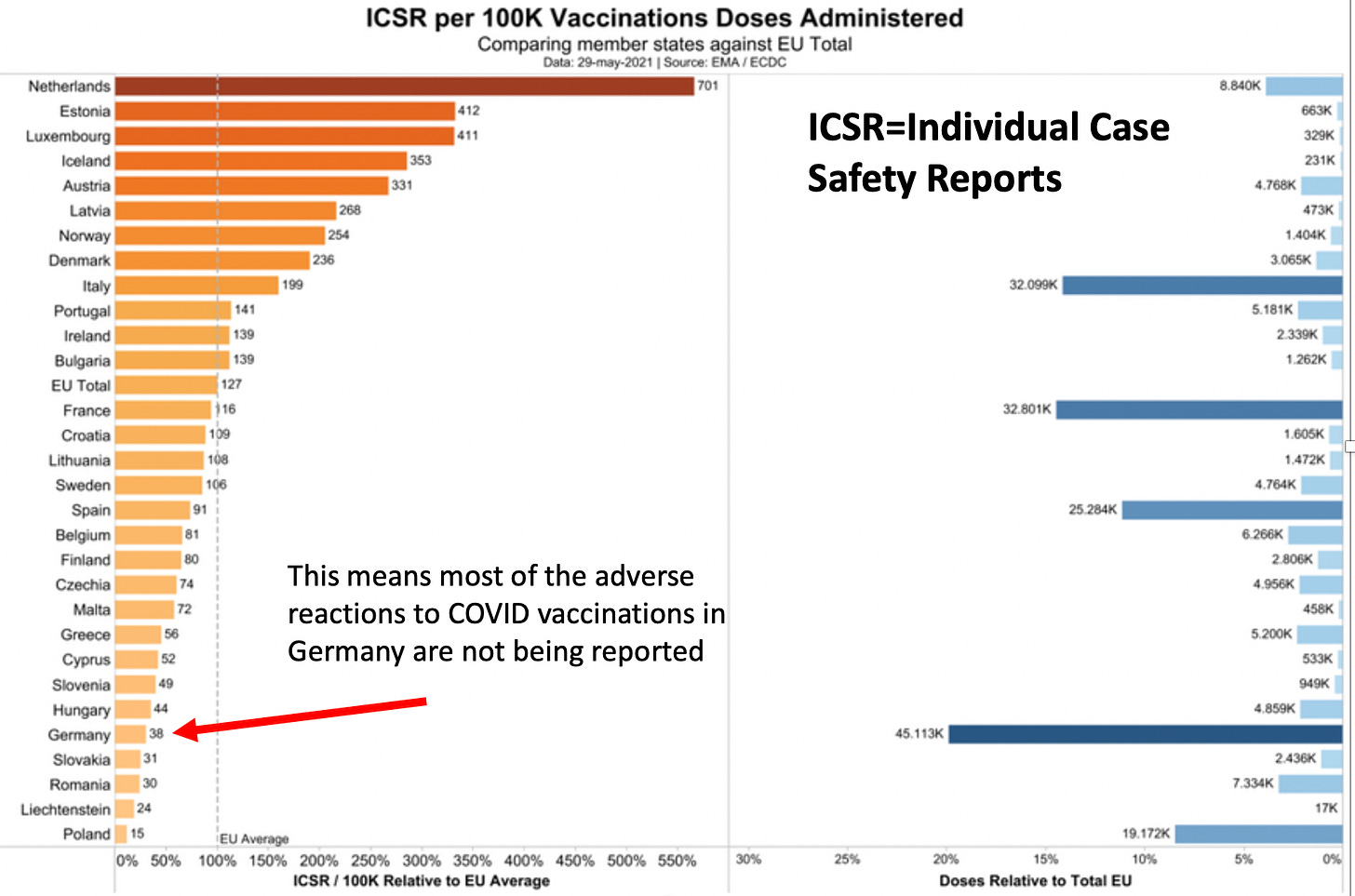
(The above graph illustrates why many of my German friends are not happy with their government)
Because of their tradition of reporting adverse reactions to vaccination, Germans (or at least some of them) have been more resistant to toeing the party line on concealing the dangers of the COVID-19 vaccines than citizens of many other countries (my friends there are enraged by the egregious concealment of critical safety data by the German government). In turn, some of the most critical vaccine data available comes from the German people as many of them have retained their intellectual integrity throughout the pandemic.
For instance, although autopsies should always be conducted on those who died suspiciously after vaccination, due to the global climate of intimidation against conducting any type of research that challenges the COVID vaccine program, it is rarely done. Instead, almost every autopsy has been performed by a few brave pathologists in Germany, and I have tried to detail the pathologist’s work throughout my postings (e.g., see here).
Some of the most important contributions of these autopsies include:
- Demonstrating that there is highly unusual tissue inflammation in those who died after vaccination. Pathologists had not observed this phenomena before the COVID-19 vaccines, and stated the inflammation they observed would likely be fatal.
- Demonstrating that the COVID spike protein could also be found in the tissues of those who died.
- Demonstrating that another key part of the SARS-CoV-2 virus was not present, meaning that the only possible source of the spike protein was the vaccine.
The most definitive study on this subject was recently completed. It examined 35 individuals who died within 20 days of vaccination, and after a lengthy examination excluded 10 who had a potential cause of death other than vaccination. Of the remaining 25, most had causes of death that frequently been linked to vaccination, and of those, 5 were found to have myocarditis potentially linked to the vaccine, and in 3 cases the vaccine was determined to be the definitive cause of their myocarditis and death. These results are very important for convicting the vaccines if it can also be proven that a large number of unexpected deaths are occurring following vaccination.
The Religion of Data
Every group needs to have some type of ideology to unite behind. Presently, one of the fixations within the Western world is on more and more data being the solution to everything. In turn, there are many concerns with this approach (e.g., it dehumanizes people, its “necessity” is used to justify violating citizen’s right to privacy while collecting it and it is being used to build an infrastructure that controls every aspect of our lives).
Although data is often claimed to be our salvation, and I will admit sometimes is quite helpful, in many other cases, it fails abysmally to address our problems. A major reason for this failure is that no one wants to critically analyze data this is gathered if that data suggests we should stop supporting an entrenched financial interest.
I am most aware of this in healthcare, as I know of numerous systems which were designed to analyze electronic medical records and either identify which pharmaceutical worked best for a condition, or if a pharmaceutical (or vaccine) was unsafe. Not surprisingly, all of these systems were never adopted, and the endless data we collect in healthcare (e.g., all the diagnostic coding data which medical insurance providers provide as a condition of reimbursement to healthcare providers) is rarely utilized to improve the public good. However, while prevailing biases frequently produces flawed analyses of data, data itself does not lie and has immense potential to expose dangerous health care practices if people are willing to look at it.
The largest insurance provider in Germany, BKK, provides coverage to approximately 10.9 million Germans. A board member, Andreas Schöfbeck, observed some very concerning signs in their data, and unlike everyone else, had the courage to disclose it in a letter to the German government (e.g. he addressed the PEI), after which, he was dismissed from his position. The BKK dataset (discussed by Jessica Rose) was the one which showed 2.05% of vaccine recipients subsequently sought medical care with a healthcare provider (others estimated it demonstrated 3.5% were struggling with persistent vaccine side effects).
This concerning safety signal prompted one German Political Party, the AFD (a controversial right wing party that has gained appeal through opposing the mandates) to file the German equivalent of FOIA for the rest of the insurance data (note: a few friends in Germany who are lifelong liberals joined AFD told me they believe “conservative” is a more appropriate label for AFD). Recently AFD obtained AOK Sachsen-Anhalt’s data, which once analyzed, demonstrated that many of the conditions we associate with COVID-19 injuries noticeably increased when the vaccination campaign initiated. According to this interview and Google translate, the conditions which rose five-fold or more were:
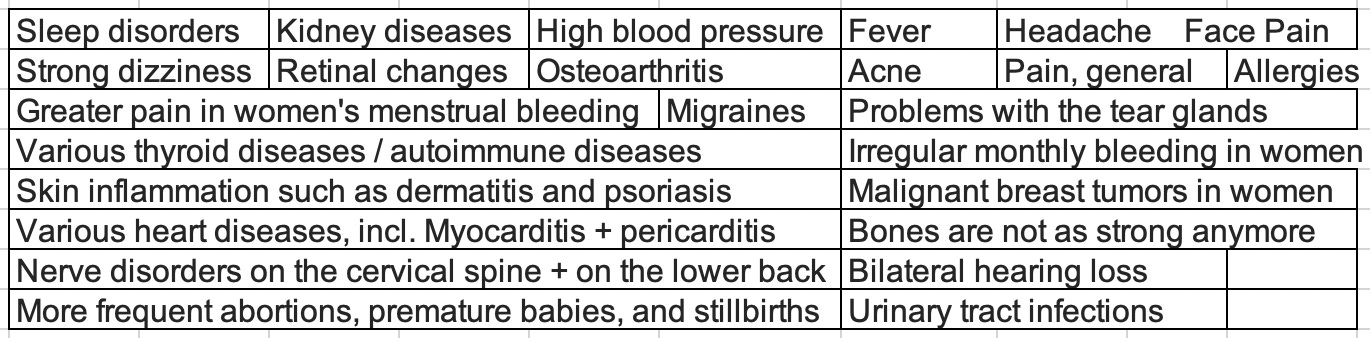
AFD’s FOIA Request
AFD also submitted a FOIA request to KBV, the association which represents all physicians who receive insurance in Germany and thus the largest insurance dataset available. The official response to their FOIA request reads as follows (this was my attempted translation):
”Dear Mr. Sichert,
With an e-mail dated October 27th, 2022 you have submitted an application to the KBV after the Freedom of Information Act (IFG) on access to data of the diagnostic codes by law health-insured patients.
You have asked for the following data packages to be sent by email:
Package 1: Filtering of all insured persons who will have an ICD coding in 2021 had vaccine side effects. You have applied for the codes T88.1, T88.0, U12.9 and Y59.9 apply.
Package 2: You request the transmission of a list of the frequency of all ICD codes of the insured persons from package 1 for the period 2016 to 2021, if proportionately available also for 2022, by quarter. The data query should after your request with V and G.
Package 3: You request the transmission of a listing of the frequency of all ICD codes of all insured persons - without the number of insured persons from package 1 - for the period from 2016 to 2021, if proportionately available also for 2022 quarters. The data query should be done with V and G.
The KBV corresponds to your application and includes a tabular overview as an attachment with the desired information about the frequency of at.
The abbreviations used in the table have the following meaning:
nw= number of patients with “vaccination side effects” (defined according to requested Filtering 1 in 2021)
onws= patient numbers "without vaccination side effects" (defined according to requested Filtering 2 in 2021)Quarters of the reporting period are set as YYYYQ (e.g. 20214=Q4 2021).
The small font size in the printout is again unavoidable, since we want to make it easier to compare wanted to show all quarters of the two comparison groups on one sheet (the pdf document). However, like last time, it can be enlarged.
Today, the AFD hosted a press conference to unveil the data of those 72 million patients (the 90% of Germans with statutory health insurance) AFD had obtained from KBV. This data summarizes the number of times all ICD-10 (an international standard) diagnostic codes were used by German healthcare providers for these patients (outside of hospitals) from the first quarter of 2016 to the first quarter of 2022.
Tom Lausen is a data activist who had previously revealed the PEI and the RKI (the German equivalent of the CDC) were concealing concerning vaccine safety data and was allowed to analyze both BKK and AOK’s data. For this presentation, Lausen was able to provide a preliminary summary of the KBV data a few days after it was released:
A rough translation of this presentation can be found here (additionally YouTube now will translate the subtitles). If this video is deleted it can also be found here.
A few of the points emphasized in this presentation include:
- The [PEI](http://Paul Ehrlich Institute), the RKI and the German government have failed in their duty by federal law to evaluate COVID-19 vaccine injuries. Many of my friends and readers likewise believe they have done an atrocious job by attempting to conceal the vaccine injuries, and these agencies are frequently chastised by the German people for their conduct. Many of the arguments against the validity of this data must be viewed in the context of the fact it would be very easy to the government agencies to access and analyze this data, but despite many requests to over the last two years, they have all adamantly refused to, which is why AFD had to force them to act with its FOIA.
- It is estimated that 90% of the suspicious deaths that occur after vaccination are not reported to the PEI, and approximately 90% of those reported come from the patient themselves or their relative (which again demonstrates that German healthcare providers are failing in their duty to report vaccine injuries).
- The PEI has nonetheless received over 3,000 reports of suspicious deaths following vaccination, but has refused to perform any autopsies on those deaths. The excuse the PEI has used for their inaction is not having the explicit authority to order the autopsies (which is a spurious excuse). Fortunately as noted above, other groups without any official authority to order autopsies have nonetheless taken the initiative to perform them.
For this press conference, a presentation was put together detailing Lausen’s preliminary findings and the correspondences with the regulatory agencies, all of which can be found here. To the best of my ability, I translated and slightly modified the key portions of the presentation so that they could be accessible to English speakers, but I am certain more will be translated in the upcoming days.
The KBV Data
All of the KBV data can be reviewed with a simple search tool here, although it does not seem to work for certain ICD-10 codes. Due to the importance of this data, for data preservation purposes, I am also providing a copy of the raw data the AFD received:
Germany Total Icd 10 Code Submissions 2016 2022 1.87MB ∙ PDF File
This PDF file was supplied in a manner that makes the data quite difficult to analyze. Fortunately, one of my readers was able to move the above file into an easily sortable spreadsheet and thereby address some of the challenges with the PDF:
German Data Sortable Sheet 3.06MB ∙ XLSX File
Finally, the above sheet was sorted by that reader into a smart spreadsheet which allows you to easily observe which codes had the greatest increase in 2021-2022 (e.g. to sort them or create graphs). For those of you who are data inclined, you will likely want to create this sheet yourself, but for everyone else this is an excellent reference to start with). They were also able to use a script to put about one third of the names for the ICD-10 codes, but since there are fifteen thousand of them, it wasn’t practical for us to manually add in the rest and you will frequently need to directly look up the codes themselves (if a group wants to add the other codes in, I will be happy to repost that).
When Lausen presented the data, for each time period (e.g., 2016 quarter 1), he chose to add two different values together (code_20161 and nocode_20161). As best as I can tell from reviewing the FOIA request and the provided data, these categories represent those who also received a vaccine injury code and those who did not (as a result the majority of Germans belong to the “nocode” category).
I believe Lausen’s rationale for presenting the data in this manner was that a large number of vaccine injuries will go unreported and many vaccine injured patients are thus within the “nocode” category. Conversely, the total number of medical conditions observed in the country is not dependent upon accurate recognition of vaccine injuries.
Separating the patients by (the somewhat inaccurately classified) vaccine injury status is nonetheless a helpful means for evaluating vaccine injuries (I saw a variety of interesting trends in my preliminary examination). However, for the reasons outlined in this article, for the initial spreadsheet presented below, those result are combined.
Additionally, some of the extreme outliers exist because new ICD-10 codes are added each year and thus did not exist prior to 2021/2022. Finally, some of the codes you would expect to have large changes may not show in this dataset if they are codes typically used in a hospital setting as this dataset does not include hospital code submissions.
Kbv Data Sorted Into Accessible Excel Sheet - 9.46MB ∙ XLSX File
In the coming days, I know many will use this data to verify our work identifying which codes in 2021-2022 had the greatest increase (you can also do that piece by piece with the already available tool), and then cross reference those to the increases reported in VAERS or other datasets. There is an immense amount to be ascertained here, and I believe it represents the credible evidence we have been looking for since the start of the pandemic to have an objective metric for quantifying the impact of vaccine injury. However, it is also critical we determine which of the observed trends are not due to artifacts within the data.
Lausen’s Presentation of the KBV Data

This is probably the most important graph of Lausen’s presentation. We have all heard stories of individuals dying suddenly after vaccination (I’ve even read a report of an individual who appeared to be in good health making a thump in another room and being found dead shortly after by their spouse).
This issue was recently brought to the public’s attention with Died Suddenly, a documentary that effectively brought attention to this issue, but also had factual errors which were counterproductive for persuading the public that this issue is real. However, while some of the proof that Died Suddenly provided to assert the existence of the sudden death phenomenon could not stand up to outside scrutiny, the same cannot be said of the KBV data.
Additionally, one way that individuals have analyzed the unusual changes in health following the vaccination campaigns has been to assess how far they fall outside of the expected range of variation (this was also done for the final spreadsheet). I did a quick calculation for the above graph and found that 2021’s increase from 2016-2020 was 37.7σ, while 2022’s was 41.0σ. This is quite a big deal (the rarity of an event happening by chance increases exponentially as the σ increases). For context, a 7σ event has a 1/390,632,286,180 chance of spontaneously occurring (it is thought to occur once in a billion years), a 10σ event happens spontaneously once every 5.249e+020 years, and a 25σ event happens by chance every 1.309e+135 years (I was not able to find a reference on the probabilities for the even higher σ events observed here).
Given these numbers, it is very difficult to argue that these events were not caused by something. In this regard, we are also quite fortunate that while the vaccines were rushed to the market over a period of time far too short to establish safety, that process still took a year. Because of this lag, it is possible to refute the reflexively cited counterargument that these changes were due to COVID-19 or the lockdowns, as these only occurred in 2020 (the only possible exception I can think of is that Delta emerged near the end of 2020, but the spike started well before Delta became prevalent in Europe later in 2021).
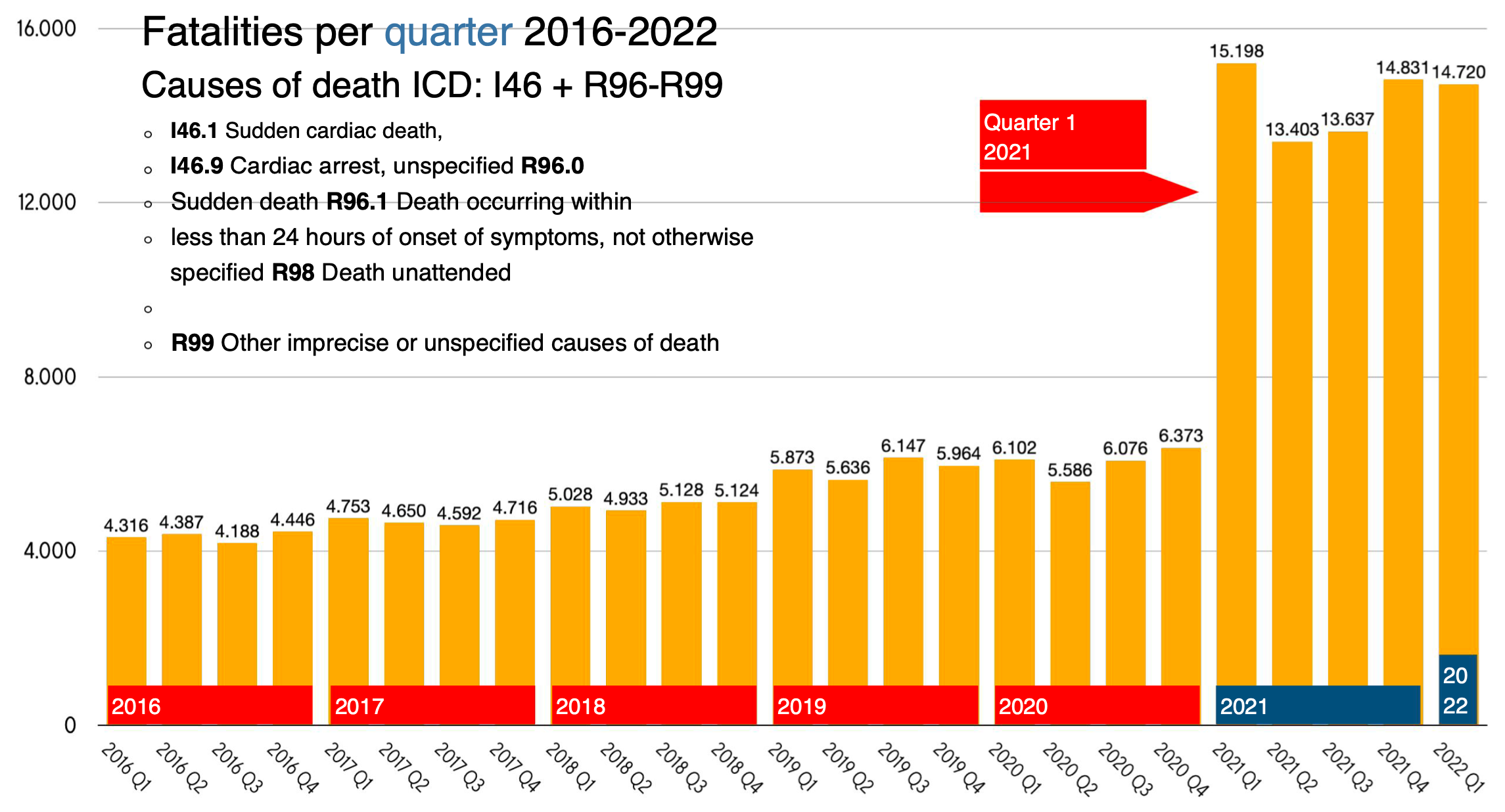
This is a similar graph to the previous one, but include sudden cardiac death, which as many of you know also “unexpectedly” increased. Many authoritative sources have argued Lausen made a mistake to correlate vaccine injuries with the spike in sudden death because very few vaccines were given at the start of 2021 and thus if a correlation was there, it should have been not emerged until the second quarter.
For context, this was the rate of COVID vaccination in Germany:
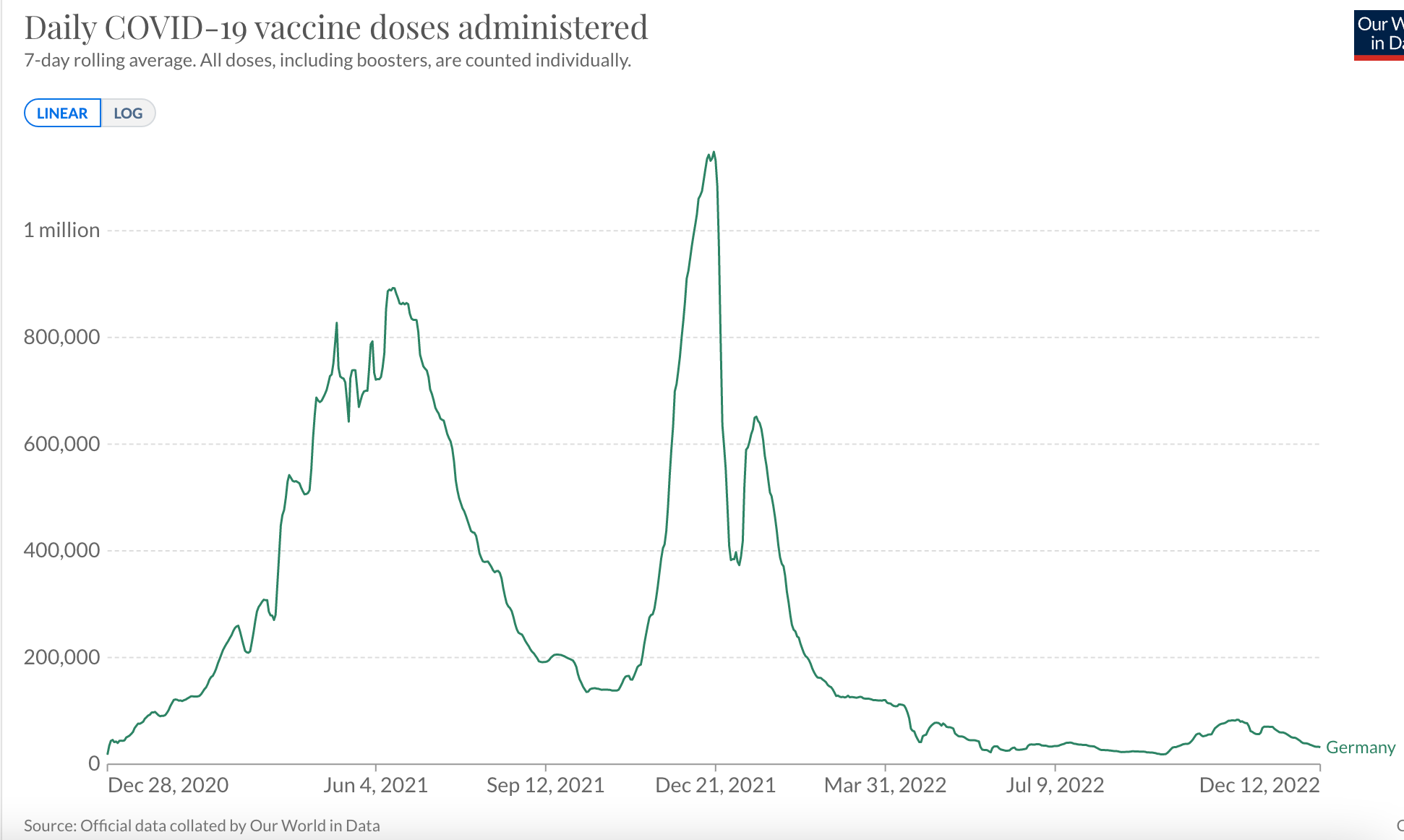
As you can see, many vaccines were given in the first quarter of 2021.
COVID-19 is not the only vaccination regularly received. For example in Germany in 2019, it was estimated that 39% of those 65 and older received an influenza vaccination. However, unlike previous vaccines, the introduction of the COVID-19 vaccine caused far more people to require medical care for a vaccine side effect.
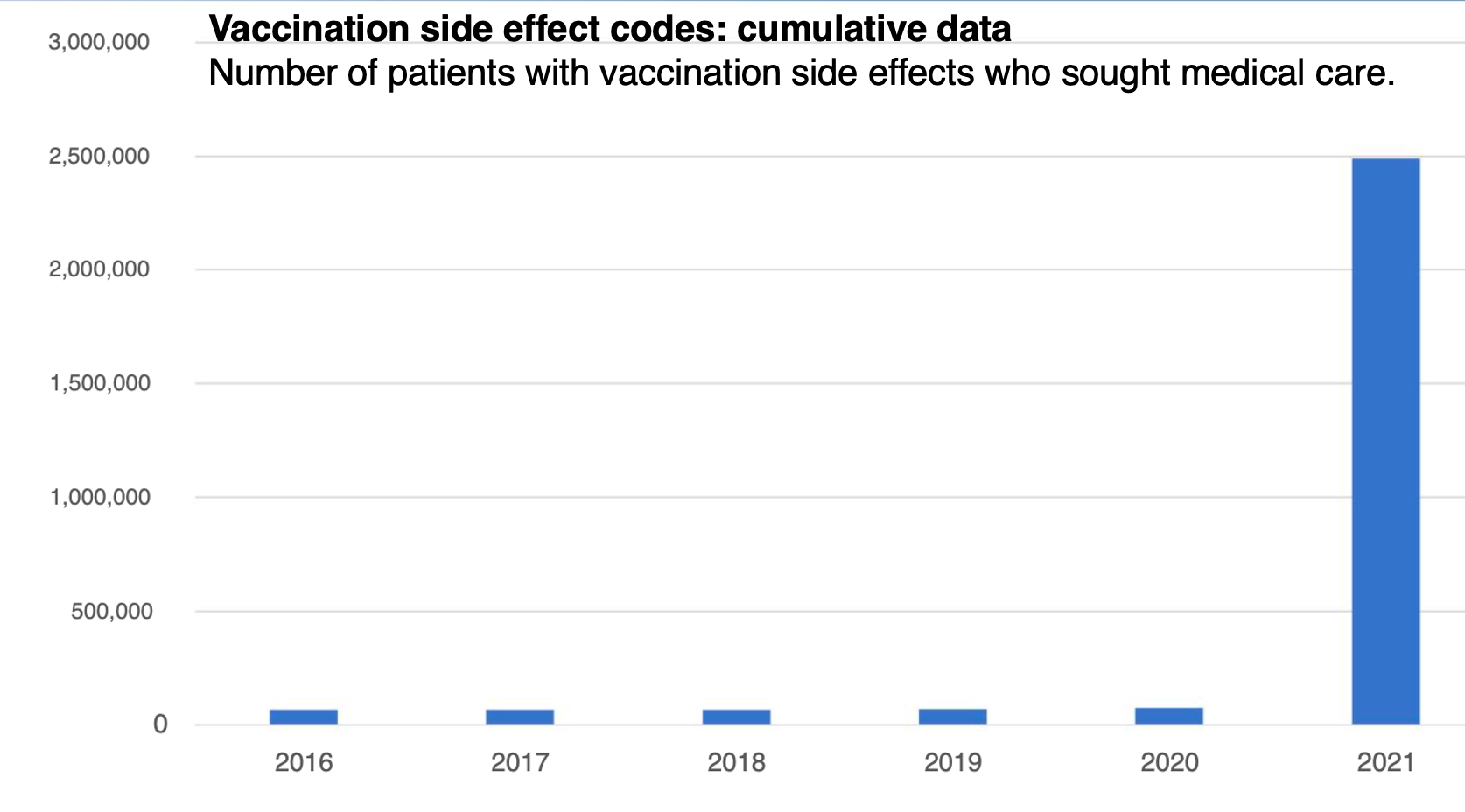
Given that Germany has a longstanding practice of evaluating vaccine injuries, this graph makes a very important point. An actual increase in vaccine injuries is occurring and it is not a result of a bias leading to over-reporting; it is a result of the vaccines being dangerous and patients needing medical care for the injuries.
Additionally, an outside team which looked at this data concluded approximately 5% of vaccine recipients subsequently required medical care, which is in line with the 7.7% discovered in V-Safe’s data and required a court order to be released as the CDC understandably did not wish to disclose this information. Note: I believe this discrepancy could be partially explained by the undercounting of vaccine codes highlighted in this article.
The general correlation between these two datasets is important. V-safe monitored 10 million vaccine recipients for a few specific things and was arguably the best surveillance system in place for tracking the side effects of these vaccines as it had a large but defined sample who were provided an easy way to report the chosen side effects. Since one of its key metrics matches the KBV data, this argues that at least some of the KBV data is valid.
Note: I am not sure if this specific dataset is referring to the total number of patients who sought care or the total number of times codes were submitted for vaccine injuries (which would mean a smaller number in total were injured).
Given that there are thousands of ICD codes that I could search the database for (many other increases, such as those of certain cancers, were highlighted in Lausen’s presentation), I had to put some thought into which of those many increases would be the best to show for this article (there were a lot of compelling candidates).
Previously, I proposed a model for the unusual fibrous clots observed in Died Suddenly that revolved around spike proteins causing protein misfolding. In support of this model, I highlighted an observed increase of an extremely rare protein misfolding disease which continues to be reported in VAERS.
Creutzfeldt-Jakob disease typically develop over years and occurs in approximately one in a million people annually, making its occurrence immediately after vaccination rare to the point that suggests causation (and as Jessica Rose noted, new reports are continuing to arrive in VAERS). The increase I proposed was a key point of contention for those who did not agree with my misfolded clot hypothesis, so I was eager to see if a current dataset could evaluate what was occurring.
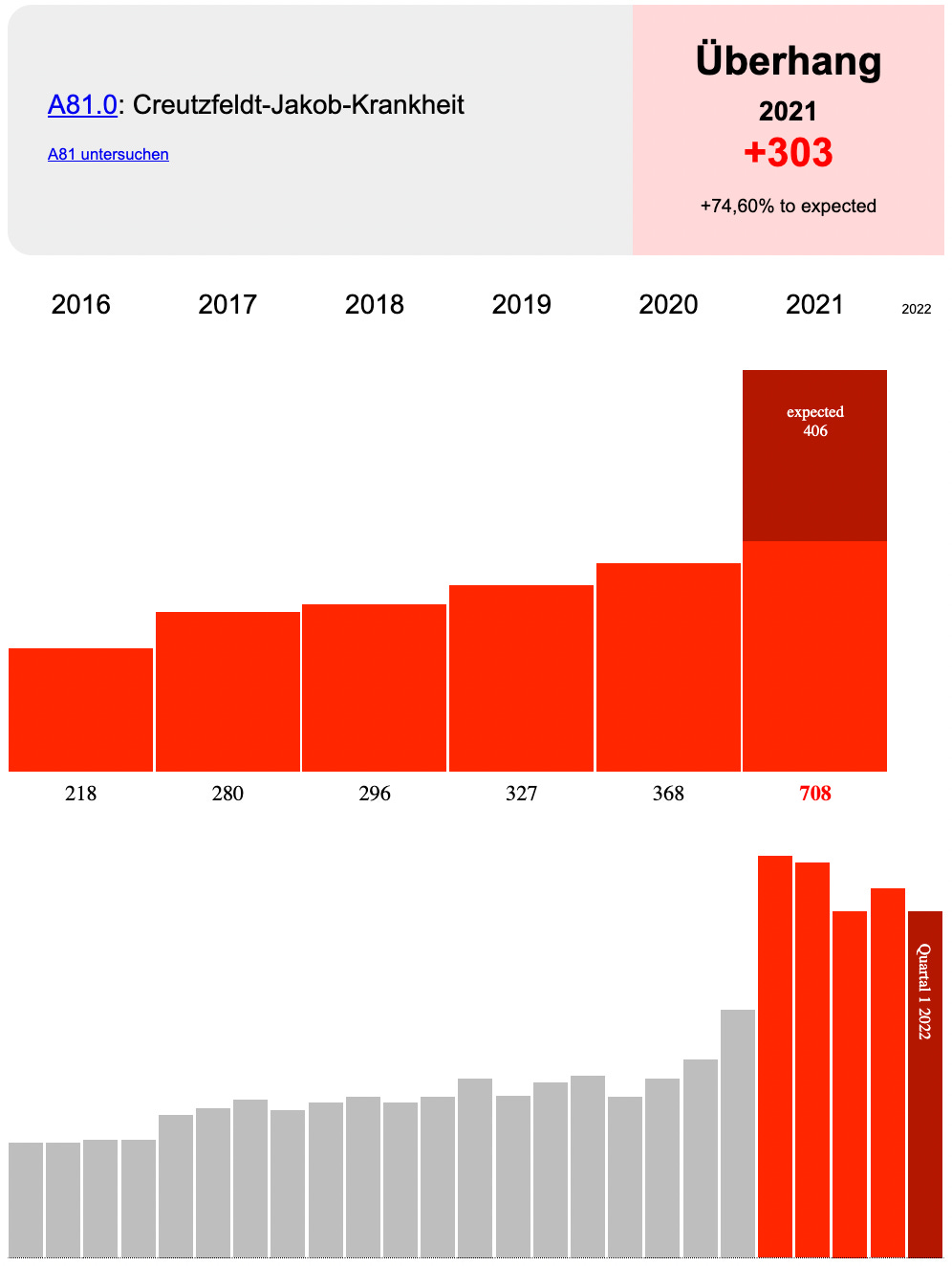
This increase is also quite large, and for all practical purposes impossible to have occurred by chance (although I will mention the authors who published the original case series linking COVID vaccination to 26 cases of CJD also determined that Delta appeared to have an increased capacity to trigger protein misfolding but I do not believe that can explain the above trend).
Since this article was published, one reader has now attempted to present a longer analysis of this data which shows multiple interesting trends (e.g., many of the side effects commonly attributed to COVID vaccination appeared to have increased) along with raising additional questions about this data. It is my hope others will also do so!
Finally, the presentation on the KBV data proposes a fatality rate for the COVID vaccines. This chart was compiled by Lausen from the officially reported adverse events to the vaccines and likely are significantly undercounting the vaccine fatality rate.
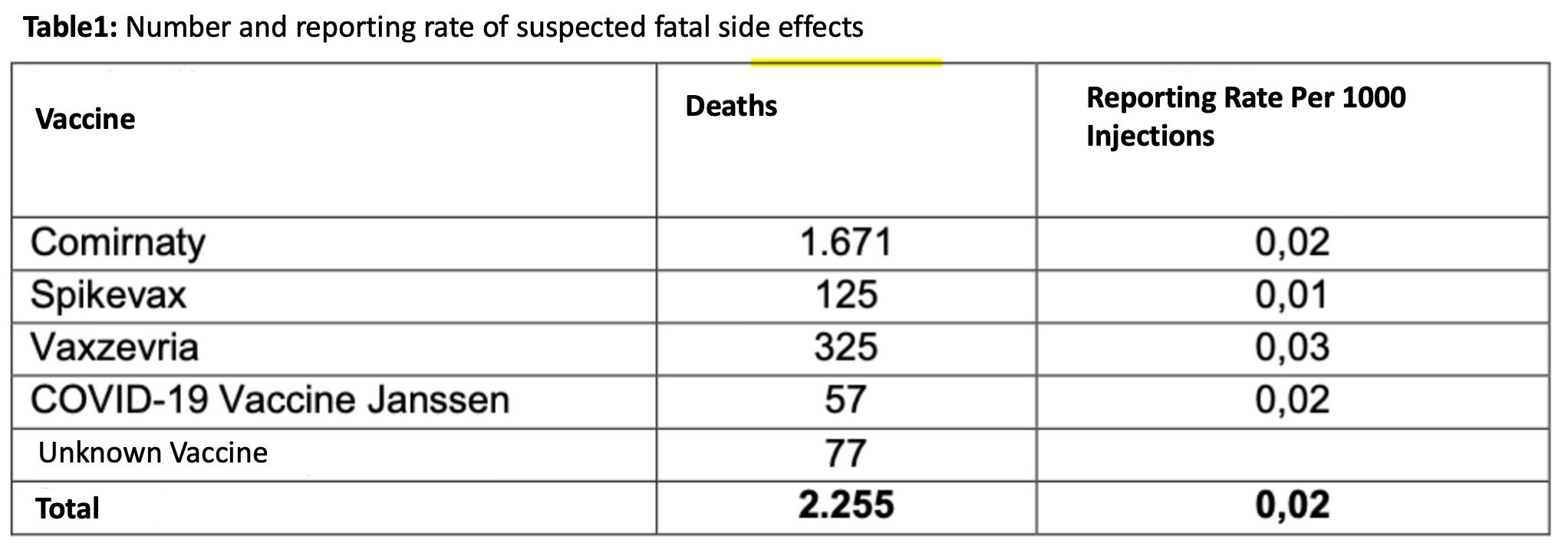
Is This Data Valid?
Following the AFD’s press conference, the leading medical research institute in Germany, ZI, acted as a third party to present a rebuttal of how AFD interpreted KBV’s data. I did not agree with their argument (that there results were an artifact of AFD also requesting for everyone who specifically died in 2021), but did note that their response acknowledged the authenticity of this data.
The primary argument presented by ZI was that since the FOIA request selected for all patients who were vaccine injured in 2021-2022, the rise in deaths observed in 2021-2022 was simply due to the fact anyone who was vaccinated in 2021-2022 could not have died prior to 2021-2022 and thus the increase in deaths observed in 2021-2022 compared to what occurred prior to this time was due to the cohort effect.
On the surface this seems like a credible way to dismiss anyone who would make such an elementary mistake and believe in this data. However, the German authorities have a long track record of attempting to cover up evidence of COVID vaccine harm (in addition to the points discussed above, the German government has been perpetually delaying releasing the death statistics for 2021), so these arguments require a critical evaluation. In turn, there is a few major issue with it:
First, the “nocode” group should not suffer from the cohort effect and it was this group that comprised the majority of the increase in sudden deaths (review the wording of the FOIA request shown above). If the “code” group were to be removed (which potentially suffers from the cohort effect), an almost identical trend would still be present. Lausen presented his data by merging the code and nocode groups together which invalidated this counterargument, and I cannot see how a “cohort effect” is present in the combined data unless KBV failed to fulfill the FIOA in the manner that was requested (Lausen also subsequently provided an interview addressing the government criticisms of his analysis).
An outside analyst also looked at this data and demonstrated that other fatal conditions (which should be vulnerable to same the cohort effect ZI is asserting) did not have the same 2021 spike:
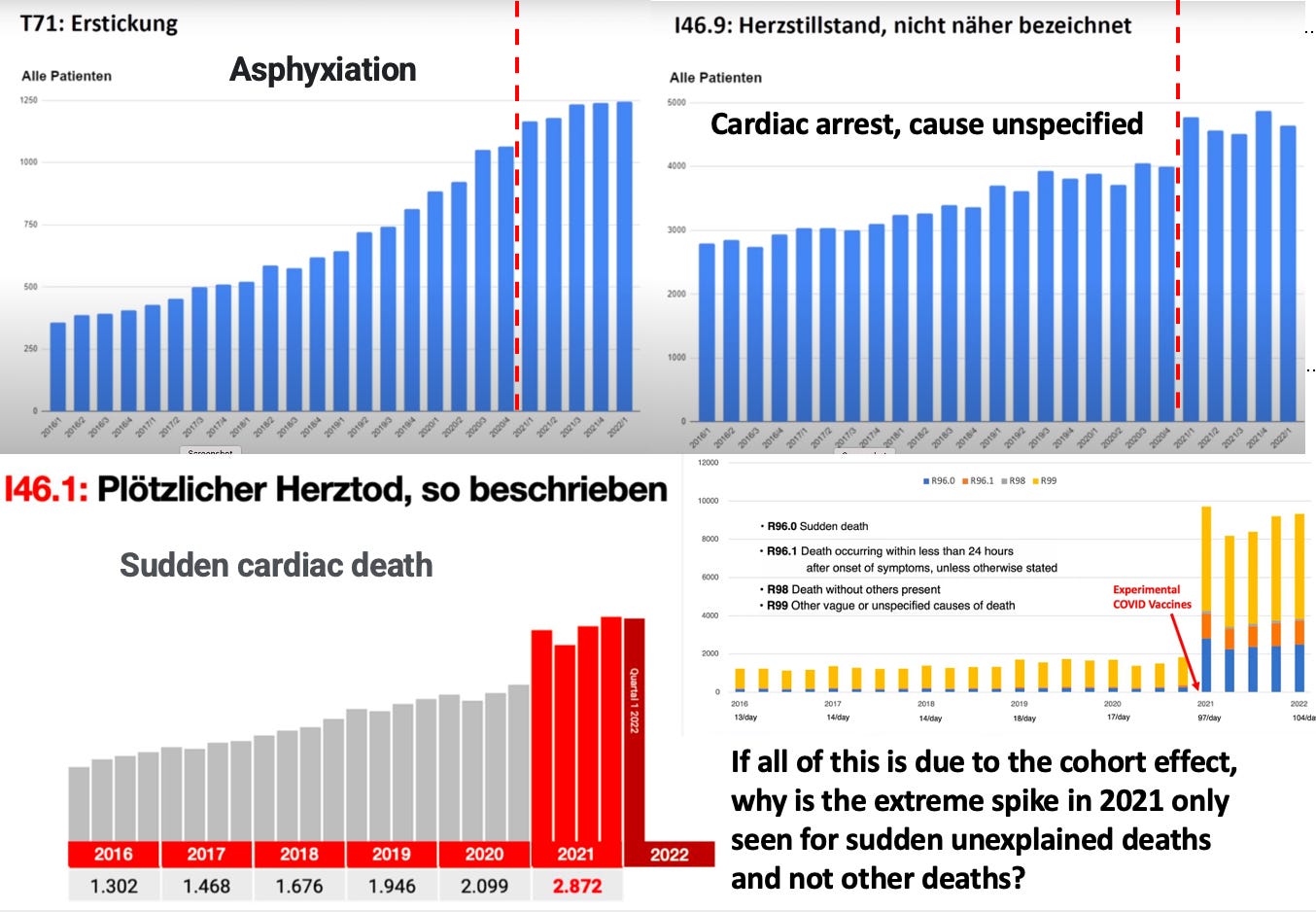
Second, the large σ found for many, (but by no means all) non-fatal conditions in the dataset indicates that something besides artifacts relating to time of death is causing the changes observed. I acknowledge that it is very possible some of the discrepancies present are due to not yet identified artifacts within the data, but at this point in time I have not been able to identify them. I believe that since KBV was focused on debunking the rise in sudden death codes, they did not focus on the rise in other codes for conditions associated with COVID vaccine injuries that were also observed. However, while this was not their focus, this point must nonetheless be considered since it does negate their counterargument.
Additionally, The death argument ZI made was also inconsistent with the death codes in question nonetheless being reported prior to 2021, which they attributed to “coding errors or unaddressed billing fraud.” To some extent this is hand-waving that many others have contested (and something any type of auditing algorithm should have caught years before), but I do not believe it is as important as the first two points.
Conversely, the strongest argument ZI put forward to establish that a cohort effect was occurring for the reported deaths was this spreadsheet. I have not yet been able to discern how the data in it was derived as it does not match the other things I looked at, so I cannot comment on if this is correct (an independent analyst arrived at the same conclusion I did). This spreadsheet is the one source of data that could refute AFD’s argument so I would greatly appreciate any additional thoughts on this one). However, I must also note that if this data is actually correct, it still does not negate the non-fatal complications of vaccination being observed.
A German rebuttal of ZI’s arguments was posted here. AFD also discussed the above rebuttal in a thread here stating:
"Hello all. The death-numbers that we have published are being hotly debated right now. Now the Central Institute for the KBV has joined in has said that the data we presented were quite easy to explain: 'The data is only for people who have accessed a medical service in 2021 and only such people had been billed and therefore would be in the data and everything in the years before are statistical runaways. There are also different causes of death that were significantly higher in the years before such as I46.9 (heart attack without successful reanimation). ' All together 104 000 people have been coded as deaths in the years 2016-2020 of whom the Central Institute of the KBV now says that they were billed medical services in 2021. Now we have a question: If this is really true, we demand an explanation from the Central Institute of the KBV how 104 000 persons that have died in the years 2016-2020 have been billed medical services in 2021.” [Translated courtesy of a reader]
The following was also written in the tweet: “Allegedly, the figures from the KBV are only for patients with health insurance, for whom services were billed in 2021. However, the causes of death were coded for 104,000 patients in previous years. Do we have a data scandal or a billing scandal?”
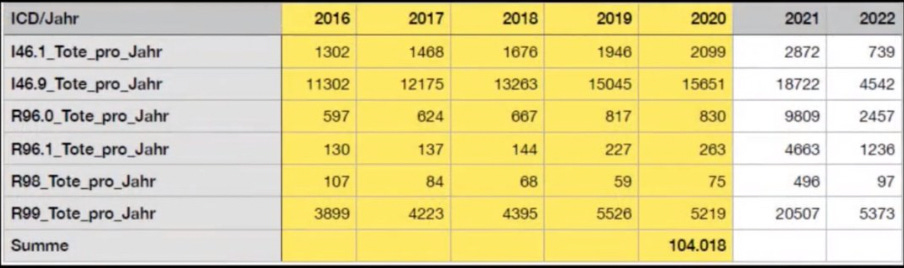
This table also refutes ZI’s argument that only those who were able to see a doctor and thus were alive in 2021 comprised the cohort of the insurance data.
Many of the German commentators I saw online were also skeptical of the official rebuttals to this data. I was recently sent a detailed summary of the events after the press conference which demonstrated that the rationale for debunking the data changed as time went forward. As best as I can tell, no clear reason was presented for why Lausen’s analysis was flawed given. Instead it was insinuated either that Lausen incorrectly filtered the data (my team and others however arrived at the same results Lausen did) or that there was a data transmission error from the KBV (which is possible but would have had to have been deliberate or inconceivable incompetence).
KBV also issued an astonishing statement refuting AFD’s presentation:
The KBV board clarifies: Based on the billing data transmitted by the KBV to the AfD or. ICD-10 codes cannot be used to establish causal relationships between COVID-19 vaccinations and deaths. From the KBV's point of view, the increase in deaths shown in quarters I-IV 2021 and quarter I 2022 is largely pandemic-related mortality. This once again illustrates the importance of COVID 19 vaccination as an effective measure to prevent serious forms of progress up to deaths. Without the vaccination, mortality would probably have been much higher.
This statement also cited the previously referenced ZI letter and another one which noted:
-
The codes in this database do not include codes entered on death certificates and thus cannot be assigned as the cause of death [however all of these codes cannot be entered unless the patient died; also as the statement above shows KBV is admitting an increase in deaths did occur].
-
The codes in this database cannot be correlated with vaccination status because many people received the COVID vaccines in settings that did not result in codes being submitted and coding for COVID vaccination has not yet been included in the dataset due to special regulations [I agree with this point, but it fails to refute this dataset since Lausen chose to combine the code and nocode groups; instead, it simply argues that vaccine injuries are underreported in this dataset].
-
This database was not created for the purpose of conducting medical research and therefore no conclusion can be drawn from it [I don’t believe this is a valid argument; a lot can be inferred from it and it is the best available database we have, so until the government chooses to make a better database available, it is “the evidence.” Additionally, this is a very similar argument to what is said for VAERS, but unlike VAERS there is not an over or underreporting issue present with this dataset].
I do not believe any of the above points refute the sudden increases in submitted billing codes (hypothesized to correlate with vaccine injuries) that occurred a year after the pandemic started at the exact same time the vaccination campaign began. However, I also believe some type of not yet identified artifact could account for at least some of what was observed and I have spent the last week revising this article to account for the additional information I come across. If anyone can provider a stronger refutation of the data presented here (preferably, at the pinned comment), I would greatly appreciate it. We need to help each other stay honest and I will gladly retract this article if a critical mistake was made.
Note: An independent analyst who reviewed the entire dataset found that it showed many other signs of being plausible.
Conclusion
Given the extremely concerning implications of the German data, it is not surprising that governments around the world and healthcare systems or insurance providers have been reluctant to release their own data. It is my sincere hope that this release will open the flood gates to additional disclosures and I am in complete agreement with the conclusion of this presentation:

I wish we had an American political party stating the same. There are signs of hope however; today Ron DeSantis did something incredible and requested a grand jury against Pfizer and Moderna, an essential step a few leaders in our movement have been working to lay the groundwork for over the last two years. I am also hopeful that this grand jury will compel the state of Florida to release similar data that can be used to assess the safety of these vaccines.
I strongly encourage those of you who who are able to begin looking through the KBV dataset and identifying important trends that can be correlated to other observations we have made over the last two years. I believe there are many excellent articles that could be written on them. I sincerely thank all of you for your continued support!
My primary goal is to draw attention to this data so numerous independent parties can objectively analyze it and independently verify if the trends it shows correlate to “controversial” increases observed in other datasets like VAERS. This data is extremely important as it is the only access we have ever been given to observe the changes in illness that follow the COVID vaccination campaigns. I also suspect the most important use of this data **will be to establish causality for specific vaccine injuries.
**This matters because typically when someone suffers a pharmaceutical injury, it is not acknowledged by the the government and the courts because “there is no evidence the product is associated with that injury,” and as you might expect, the pharmaceutical industry work tirelessly to make sure the evidence that could implicate their product never emerges.
At this point I’ve lost track of how many sad instances I’ve seen where this happened to a medically injured patient (in some cases to the point the gaslighted victim gives up and ends their lives), so I greatly support having an independent means to assess causality for vaccine injuries. Those injured by the COVID-19 vaccines are profoundly suffering and they really need help (on the bright side however, recently Senator Johnson and shortly after Governor DeSantis gave a voice to these victims).
Postscript: It appears a similar rise in unexplained deaths is occurring in Canada.
The question posed at this point is: Is the collective West nearing the end of a cycle? Or are we still in mid-cycle? And is this a four-generational mini-cycle, or an epochal point of inflection?
Is Russo-Chinese Entente and the global tectonic discontent with the ‘Rules Order’ – on the heels of a long trajectory of catastrophes from Viet Nam, through Iraq to Ukraine – sufficient to move the West on to the next stage of cyclical change from apex to disillusionment, retrenchment and eventual stabilisation? Or not?
A major inflection point is typically a period in history when all the negative components from the outgoing era ‘come into play’ – all at once, and all together; and when an anxious ruling class resorts to widespread repression.
Elements of such crises of inflection are today everywhere present: Deep schism in the U.S.; mass protest in France, and across Europe. A crisis in Israel. Faltering economies; and the threat of some, as yet undefined, financial crisis chilling the air.
Yet, anger erupts at the very suggestion that the West is in difficulties; that its ‘moment in the sun’ must give place to others,and to other cultures’ ways of doing things. The consequence to such a moment of epochal ‘in-betweeness’ has been characterised historically by the irruption of disorder, the breakdown of ethical norms, and the loss of a grip on what is real: Black becomes white; right becomes wrong; up becomes down.
That’s where we are – in the grip of western élite anxiety and a desperation to keep the ‘old machinery’s’ wheels spinning; its ratchets loudly opening and closing, and its levers clanging into, and out of place – all to give the impression of forward motion when, in truth, practically all of western energy is consumed in simply keeping the mechanism noisily aloft, and not crashing to an irreversible, dysfunctional stop.
So, this is the paradigm that governs western politics today: Doubling-down on the Rules Order with no strategic blueprint of what it is supposed to achieve – in fact no blueprint at all, except for ‘fingers crossed’ that something beneficial for the West will emerge, ex machina. The various foreign policy ‘narratives’ (Taiwan, Ukraine, Iran, Israel) contain little of substance. They are all clever linguistics; appeals to emotion, and with no real substance.
All this is hard to assimilate for those living in the non-West. For they do not come face-to-face with western Europe’s repeat re-anactment of the French Revolution’s iconic secular, egalitarian reform of human society – with ‘the specific timbre, flavour and ideology’ shifting, according to prevailing historic conditions.
Other nations unafflicted by this ideology (i.e., effectively the non-West) find it perplexing. The West’s culture war barely touches cultures outside its own. Yet, paradoxically, it dominates global geo-politics – for now.
Today’s ‘flavour’ is termed ‘our’ liberal democracy – the ‘our’ signifying its link to a set of precepts that defies clear definition or nomenclature; but one, that from the 1970s, has drifted into a radical enmity towards the traditional European and American cultural legacy.
What is singular about the present re-enactment is that whereas the French Revolution was about achieving class equality;ending the division between aristocracy and their vassals, liberalism today represents a modification of ideology” that U.S. writer Christopher Rufo suggests, “says that we want to categorize people based on group identity and then equalize outcomes across every axis – predominantly the economic axis, health axis, employment axis, criminal justice axis—and then formalize and enforce a general levelling”.
They want absolute democratic levelling of every societal discrepancy – reaching even, back into history, to historic discrimination and inequalities; and to have history re-written to highlight such ancient practice so that they can be routed out through enforced reverse discrimination.
What has this to do with foreign policy? Well, pretty well everything (so long as ‘our’ liberalism) retains its capture of the western institutional framework.
Bear this background in mind when thinking of the western political class’s reaction to events, say, in the Middle East, or in Ukraine. Although the cognitive élite contends that they are tolerant, inclusive, and pluralistic, they will not accept the moral legitimacy of their opponents. That is why in the U.S. – where the Cultural War is most developed – the language deployed by its foreign policy practitioners is so intemperate and inflammatory towards non-compliant states.
The point here is that, as Professor Frank Furedi has emphasised, the contemporary ‘timbre’ is one no longer merely adversarial, but unremittingly hegemonic. It is not a ‘turn’. It is a rupture: The determination to displace other sets of values by a western inspired ‘Rules-Based Order’.
Being a ‘liberal’ (in this strictly narrow sense) isn’t something you ‘do’; it is what you ‘are’. You think ‘right thoughts’ and utter ‘right speak’. Persuasion and compromise reflect only moral weakness in this vision. Ask the U.S. neocons!
We are used to hearing western officials talk about the ‘Rules-Based Order’ and the Multi-Polar System as rivals in a new global framework of intense ‘competition’. That however, would be to misconceive the nature of the ‘liberal’ project. They are not rivals: There cannot be ‘rivals’; they can only be recalcitrant other societies that have refused the analysis and the need to root out all cultural and psychological structures of inequity from their own domains. (Hence, China is hounded on its alleged deficiency in respect to the Uyghurs).
The cognitive privilege of ‘awareness’ is what lies behind the western ‘doubling-down’ on imposing a global Rules-BasedOrder: No compromise. The moral enterprise is more intent on its elevated moral station than on coming to terms with or managing, say, a defeat in Ukraine.
Just yesterday, the Bank of America in London was forced to cut short a two-day, online conference on geopolitics; andapologised to attendees following the outrage expressed at a speaker’s comments that were deemed ‘pro-Russian’ by some attendees.
What was said? Professor Nicolai Petro’s remarks at the session where he said: “Under any scenario, Ukraine would be the overwhelming loser in the war: Its industrial capacity devastated … and its population shrunk as people departed to look for employment abroad. If this is what is meant by removing Ukraine’s capacity to wage war against Russia, then it [Russia] will have won”. Professor Petro added that the U.S. government had no interest in a ceasefire, as it had the most to gain from a prolonged conflict.
No compromise is allowed. To speak thus, to inhabit the western moral high ground creating ‘villains’, clearly is more important than coming to terms with reality. Professor Petro’s comments were condemned as “rolling through Moscow’s talking points”.
Yet, these cultural revolutionaries face a pitfall, Christopher Rufo writes,
“Theirs is actually, not an easy task. This is very difficult, and, in fact, I think is somewhat impossible. If you look at even the Chinese Cultural Revolution in the 1960s … They had a program of economic and social levelling that was more totalitarian and more drastic than anything that had ever happened in the past. [Yet] after the Revolution collapsed, after the period of retrenchment, social scientists looked at the data and discovered that a generation later, those initial inequalities had stabilized … The point is that forced levelling is very elusive. It’s very difficult to achieve, even when you are doing it at the tip of a spear or at the point of a gun.
The levelling project being essentially nihilistic becomes captured by the destructive side of the revolution – its authors so absorbed with dismantling structures that they do not attend to the need to think policies through, before launching into them. The latter are not adept at doing politics: at making politics ‘work’.
Thus, discontent at the welling string of western foreign policy flops grows. Crises multiply, both in number and across different societal dimensions. Perhaps, we are closening to a point of beginning to move through the cycle – toward disillusionment, retrenchment, and stabilization; the prerequisite step to catharsis and ultimate renewal. Yet, it would be a mistake to underestimate the longevity and tenacity of the western revolutionary impulse.
“The revolution does not operate as an explicit political movement. It operates laterally through the bureaucracy and it filters its revolutionary language through the language of the therapeutic, the language of the pedagogical, or the language of the corporate HR department”, Professor Furedi writes. “And then, it establishes power anti-democratically, bypassing the democratic structure: using this manipulative and soft language – to continue the revolution from within the institutions.”
Alastair Crooke

One of the things that the plague chronicle aims to do, is draw back the curtain on the institutional or cultural roots of particular malignancies, which seem at first to be contingent on specific bad actors. While I understand that some of you find this irritating, it’s not my purpose to let anybody off the hook. It’s rather to point out that the very real villains we’re all concerned about are mere expressions of much deeper forces, and that fixing things will involve a lot more than rounding up all the Anthony Faucis of the world and trying them for crimes against humanity.
One vein of Corona analysis sees the entire pandemic as the plot of globalist conspirators who are interested in reducing the world population. There are many variations on this theory, but the most basic would hold that lockdowns and the rest were a means of driving us to accept harmful vaccination, which will cause a massive die-off among the vaccinated in the coming years and prepare the way for whatever netzero sustainable future Klaus Schwab has planned for the survivors.
My readers often send me links to podcasts, videos and other media providing proofs of this Global Depopulation Agenda. Clip compilations like this one constitute an important genre in this area. They generally feature globalist goons – in this case, Bill Gates – saying ominous things about the overabundance of humans at different interviews and panel discussions.
I have a look at almost everything you send me, and by now I’ve seen enough to note that the internet case against Gates rests heavily on the same dozen or so video statements. Some of these items, for example the third one in that link (where Gates is talking about reducing childhood mortality), are deliberately deceptive, and it’s an important question, why this area is so awash in clearly manipulated media . The rest of the clips are more or less accurate representations of Gates’s arguments, the only problem being that they’re presented too narrowly.
The fourth at that link, for example, is from a TED talk, where Gates opines that
The world today … is headed up to about nine billion [people]. Now if we do a really great job on new vaccines, healthcare, reproductive health services, we could lower that by perhaps ten or fifteen percent.
The fifth is very similar. Here, Gates pleads:
The problem is that the population is growing the fastest where the people are the least able to deal with it, so it’s in the very poorest places that you’re going to have a tripling in population by 2050. And so their ability to feed, educate, provide jobs, stability, protect the environment, in those locations means they’re facing an almost impossible problem.
If you read these statements carefully, you’ll see they don’t actually support the idea that Gates wants to reduce the world population by vaccinating people to death. First, he could hardly be expected to air such plots in a public forum; and second, Gates almost always pairs his remarks about population with other concerns about healthcare, food and education. These are strange scruples for a homicidal maniac bent on killing billions.
These statements only begin to make sense, when you realise that they’re rooted in the sociological theory of demographic transition . This theory observes that, as societies advance technologically and economically, they shift from an order of high birth rates and high death rates, to an order of low birth rates and low death rates. Gates, who like all globalist elites is worried about environmental impacts from there being too many humans, believes that he can reduce the total peak population in places like Africa by introducing medical interventions to lower mortality and thereby guide populations to a low-birthrate, post-transition demographic pattern. Whether this theory is right, or whether this makes Gates’s interventions morally defensible, are separate questions. What is beyond dispute, is that this is what Gates is arguing and what everybody in his audience understands him to be arguing.
The banal truth is that Gates is an unoriginal flabby Western liberal. He’s worried about the environment, about population and about disadvantaged brown people, and he thinks he can solve all these problems by improving healthcare. This isn’t a defence of him. I happen to think he’s a malign influence and that if we can’t rein in the Gates’s of the world we’re finished, but that’s not because he’s bent on using mRNA vaccines to decimate humanity.
Those concerned about the Global Depopulation Agenda will not be appeased by these clarifications, of course. They’ll point to anti-natalist messaging and policy in Western nations, and also to organisations like the Club of Rome and establishment intellectuals like Paul Ehrlich , who have openly railed against the spectre of overpopulation. They’ll argue – rightly – that our entire political culture is in thrall to a green movement which opposes any technology that might further human flourishing via reliable energy, regardless of its carbon impact. They’ll say I myself have frequently complained that countries like Germany are doing permanent damage to their economies by pursuing an energy transition which will make no difference in the longer term, because future carbon emissions are almost entirely a function of increasing prosperity and population growth in the developing South and East.
If there isn’t a Global Depopulation Agenda, what’s going on, and how are all these ominous developments to be explained?
The answer is very important, and it lies in the peculiarities of postwar political ideology and the moral instincts which this ideology expresses.
There are many ways to illustrate this, but the most efficient is probably this classic Nature paper on Ideological differences in the expanse of the moral circle .
Among other things, the authors asked study participants identifying as “conservatives” and “liberals” (in the American sense) to indicate their spheres of primary moral concern. “Conservatives” tended to emphasise those spheres nearest to themselves – their immediate family, their more extended relatives, their friends – as bearing the greatest moral weight. “Liberals,” meanwhile, expressed the greatest moral interest in those spheres furthest from themselves – “all people on all continents,” for example, or “all mammals.”
Plotted as heat-maps on 16 concentric circles, where the first circle is “immediate family” and the sixteenth is “all things in existence”, the comparative results look like this:
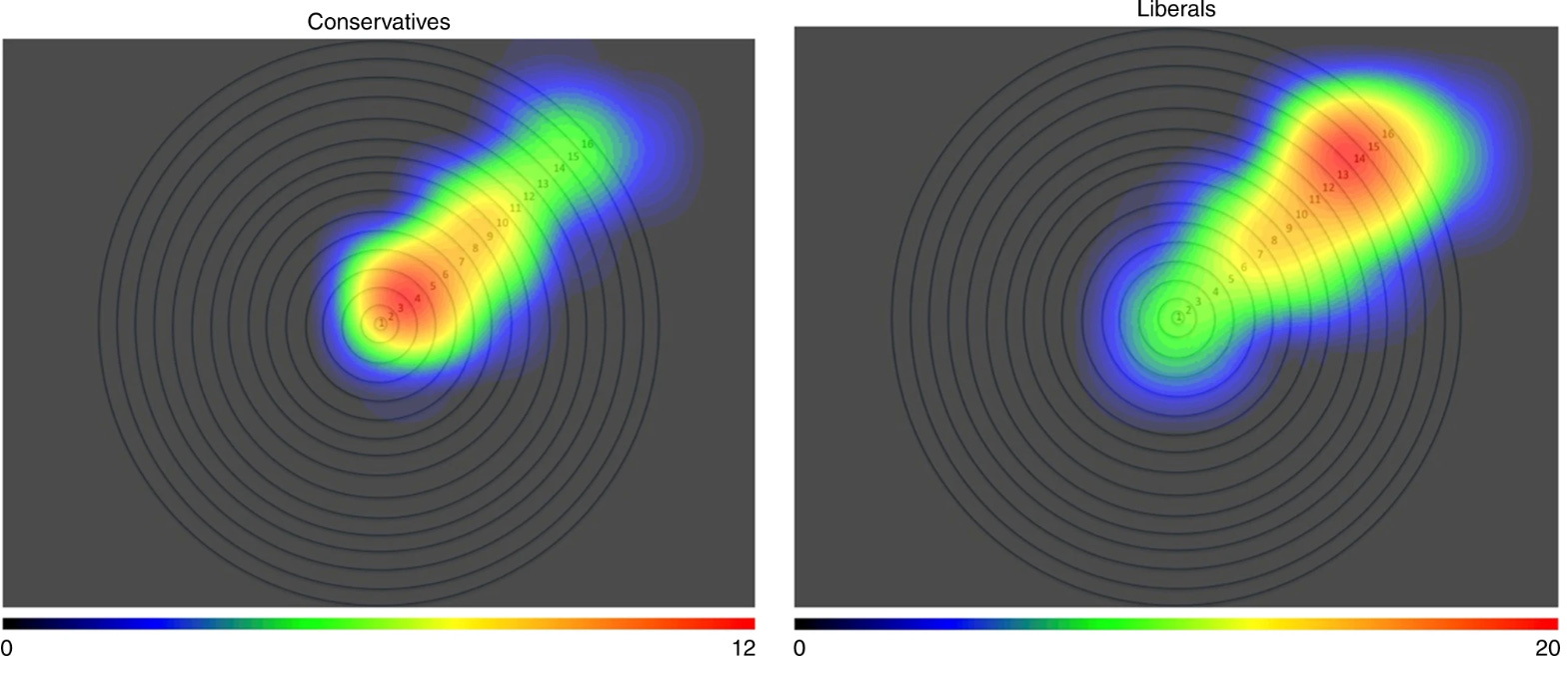
Because the future survival of humanity is at stake here, we should drop the dumb “conservative” and “liberal” labels.
The heatmap on the left is not “conservative.” It reflects the ordinary, unremarkable moral orientation of almost all human beings who have ever lived, and almost all currently living humans across the entire world. Without a moral orientation that somehow prioritises your progeny and your relatives (however widely understood), your genes will get nowhere.
The heatmap on the right, meanwhile, represents the anomalous exogenous moral orientation (EMO) of politicial and cultural elites in the developed West, which “liberal” cannot even begin to describe, and which applies primary moral emphasis to circles 13 and 14. These are “all animals in the universe, including alien lifeforms” and “all living things in the universe including plants and trees.” Substantial moral value is also attached to things in the twelfth circle, “all animals on earth including paramecia and amoebae,” and in the fifteenth circle, “all natural things in the universe including inert entities such as rocks.” These are people who, strictly speaking, claim to feel morally bound to family, friends and relatives primarily to the extent that these fall within the “living things” or “things in existence” categories.
While we aren’t exactly governed by shape-shifting lizards , we are governed by completely insane ideologues who would do the bidding of shape-shifting lizards – if necessary at our dire expense – were these ever to be discovered.
Now, it’s not quite as bad as it seems. Remember above all that these are moral aspirations and ideals; they are how study respondents claim to feel. Revealed preferences show that most of these people, in their personal lives, still attach substantial moral weight to their immediate friends, family and community. They probably feel qualms about this, however, and when the context is not so immediate – when, for example, they’re making policy decisions for millions of citizens – they’ll compensate by caving to their idealised EMO wherever possible. Put another way: Bill Gates likes the convenience of his private jet , even as he hopes to discourage people from flying.
Remember also that it is the dose which makes the poison. Some degree of EMO isn’t bad. It’s one reason that we look down on littering, for example. An important expression of growing Western EMO would be the European interest in other peoples and cultures, including much-maligned colonialism and the less-maligned British campaign to abolish the slave trade after the later eighteenth century. Particularly since 1900, however, the EMO of Western governing elites has grown ever more extreme, to the point that it has begun to constitute an existential threat for human civilisation.
How this radical and historically unprecedented EMO came to be so ingrained is a complex question. Putting it down to the media or to propaganda is not fully satisfying, because we’d have to ask where the media and the propagandists got these ideas in the first place.
A prerequisite is technology and our growing alienation from nature. Anyone who has spent a rough week or two on the face of a mountain will come away from the experience personally enriched, but perhaps also doubtful that unmanaged unmitigated nature is every bit as friendly, good and deserving of moral concern as his immediate family. Tropes which locate wisdom in distant indigenous peoples and on foreign continents likewise betray a naivete about the realities of hunter-gatherer existence and a lack of experience with life beyond the prosperous West.
A more important, immediate causal factor, is the upset in established social orders since the Industrial Revolution, which has coincided with the rise of liberal democracy, and the replacement of the traditional aristocracy with new managerial elites. The latter have frequently pursued tactical alliances with outsiders or the lower classes to displace prior establishments – including, as the quiet revolution continues, prior managerial establishments. This is the primary function of Diversity, Inclusion and Equity initiatives in America today, and it obviously encourages and depends upon both orchestraters and beneficiaries to engage in radical EMO rituals.
As the problem seems to be growing worse over time, self-reinforcing selection effects probably also play an important part. The more pronounced EMO is favoured by the governing elite, the more all politicians and persons of prominence in the West are specifically selected for this trait, or at least for their willingness to pantomime it. While people with these moral tendencies have always existed, they’ve never been so heavily concentrated in positions of influence before, and the more concentrated they become, the more aggressively they filter for like-minded radicals like themselves, even in the absence (and in excess) of any specific objective.
Once you have seen this simple dynamic at work, you cannot unsee it.
It explains the increasing prominence of animal (and even alien) protagonists in entertainment media, the overt preference for fringe sexual minorities, the predilection for supranational global political bodies and non-governmental organisations which transcend borders and national institutions.
It explains, in particular, why governing elites are so open to insane unprecedented policies like mass immigration. They no longer have particular national moral categories at all, and so they reluctantly embrace all of humanity, and preferentially all living things everywhere. Similarly, it explains why mainstream liberal policies happily enlarge the carbon footprints of millions of third-world immigrants by welcoming them into the industrialised West, while simultaneously waging war on all aspects industrial society for their supposed negative impacts on nature.
Less obviously, the radical EMO of our leaders and their supporters explains the increasing willingness of elites to tolerate suboptimal and actively harmful policies at home. The moral world of the people who run our countries has grown enormously in size, leaving the spheres of their direct jurisdiction almost microscopic in comparison. Why not shut down all of society in an effort to kill (a likely man-made) virus? Why not inject poorly tested mRNA novelty vaccines in billions and suppress all evidence of negative population-wide effects? That elites increasingly treat their populations like cattle is a direct expression of their expanded moral universe. They have so many other things to care about.
It took a while for these moral sentiments to find their proper ideological articulation. In the early 1970s, people with radical EMO signalled, for a brief time, about the dangers of human overpopulation, and there ensued a moment of moral hysteria in which people like Paul Ehrlich wrote books like The Population Bomb . The years since have seen the emergence of a more differentiated ideological system, which extends lesser but still privileged consideration to third-world populations. Thus antinatalist systems are confined mostly to the West, where the most zealous environmental policies are also implemented. That Europe could disappear tomorrow with minimal effects on long-term global population projections or the future composition of the atmosphere is irrelevant. It is the fact that this is the circle of least moral concern, which is determinative.
In the nineteenth century, somebody like Bill Gates would be far more likely to run domestic charities, but in our present hyper-EMO world, he spends every waking moment thinking about Africa, and how he can help Africans, and in the process also save nature by hastening the African transition towards lower birthrates and bringing the netzero ideal closer to reality. All the policy documents and aspirational statements produced by the World Economic Forum, the United Nations and other bodies are animated by a similar spirit.
A globalist cabal plotting the depopulation of the world would be a grave problem, but one with a clear enough solution. We’re facing, instead, an entire moral and ideological system, with very deep roots in prosperous Western culture. This isn’t a universe where everybody wakes up tomorrow, elects to put Bill Gates on trial for his crimes against humanity, and returns thereafter to sensible public health policy. It’s a world where millions of people share the ideological anxieties of eccentric children like Greta Thunberg, manifest escalating indifference to adverse policy outcomes in their own countries, and dream of a future earth devoid of humans like themselves. Because the driving forces operate at the level of moral instinct and emotion, no amount of evidence or appeals to reason that can stop this. Probably the best hope lies in its naivete and idealism. Worsening conditions will ultimately deprive these ideologies of their cultural appeal; how bad things have to get before this happens, is the terrifying question.
UPDATE: A lot of comments are querying Gates’s sincerity, suggesting ulterior motives, and so forth. I have no direct insight into the man, but I suggest that his interior state is a peripheral matter here. The problem is to understand under what moral orientation he is claiming to operate, and why that moral orientation resonates so broadly with elite Western culture.

I asked the AI Chat Bot “What was the role of the DoD in covid-countermeasures?” Here is what it wrote:
“The Department of Defense (DoD) played a significant role in the development of countermeasures against COVID-19, the disease caused by the novel coronavirus. The DoD worked closely with other federal agencies, such as the Department of Health and Human Services (HHS), to respond to the pandemic.
One of the main roles of the DoD in the COVID-19 response was to provide logistical support and medical resources to help healthcare workers and first responders on the front lines of the pandemic. The DoD also worked to develop and distribute personal protective equipment (PPE) and other supplies to support the response efforts.
In addition, the DoD provided funding and resources to support the development of vaccines and treatments for COVID-19. The Defense Advanced Research Projects Agency (DARPA), a research arm of the DoD, played a key role in this effort by funding and supporting the development of treatments and vaccines through its "Rapid Response Research" program.
Overall, the DoD played a vital role in the response to the COVID-19 pandemic by providing logistical support, medical resources, and funding for research and development efforts to combat the disease.”
AI Chat Bot gets a “F” - for a highly controlled narrative answer, which was fed to all MSM sources, while the “alternative” media did not examine it very much, with some exceptions. It wasn't just logistics or even just lots of funding, and certainly nobody was “combatting disease”.
The truth is much more interesting than fiction:
All Covid countermeasures, including the biological warfare agents marketed as “Covid-19 vaccines”, were ordered by the US DoD as a “large scale manufacturing demonstration” via Other Transactions Authority contracts.
Hundreds of Covid countermeasures contracts became available via FOIA and SEC disclosures in redacted form. Review of these contracts indicates a high degree of control by the US Government (DoD/BARDA) and specifies the scope of deliverables as “demonstrations” and “prototypes” only. In other words, the US Government and DOD specifically ordered a fake theatrical performance from the pharmaceutical manufacturers. Just to make extra certain that the pharmas are free to conduct the fakery, the contracts include the removal of all liability for the manufacturers and any contractors along the supply and distribution chain under the 2005 PREP Act and related federal legislation.
The contracts are structured under Other Transactions Authority (OTA) - OTA method of contracting allows federal agencies to order otherwise-regulated products bypassing any such regulations, as well as financial accountability mechanisms that cover standard government contracting, and other laws that regulate disclosure and Intellectual Property (IP) derived from publicly funded research.
“Other” is a catchall category that is not a contract, not a research grant, not a procurement, etc.: not any normally regulated/accountable government contracting.
Here is a typical contract scope for “vaccines”:
While the DOD/BARDA countermeasure contracts refer to safety and efficacy requirements for vaccines and mention current Good Manufacturing Practices (cGMP) compliance, these items are explicitly carved out as not being paid for nor ordered by the US Government.
This gets even more interesting when we examine some of the redactions in contracts:
I know what is in the redacted part of the above paragraph and it was not hard to figure out. The first redaction under 1.1.1 BACKGROUND is “Fosun Pharmaceuticals”, so the sentence reads “Fosun Pharmaceuticals”, Pfizer and BioNTech entered into an agreement for the co-development\u2026”
Note: the only journalist I am aware of in either “mainstream” or “resistance” who mentioned Fosun was Naomi Wolf, kudos to her. I was in touch with The Epoch Times to try to publish this information, and even they decided to bury the story (but they published my other materials). I did discuss this on Dr. Jane Ruby's show, and kudos to her as well for not being afraid to cover the truth.
Pfizer-BioNTech is really a 3-party R&D alliance: Fosun-Pfizer-BioNTech, and by “party” I mean that one of the three is the Chinese Communist Party. Fosun is a huge Chinese conglomerate that owns a large number of global companies, and its chairman Guo Guangchang is a very high ranking member of the CCP. It is curious that the US DoD awarded $10 billion (Pfizer's Operation Warp Speed/DoD/BARDA contract) to a venture whose substantial equity (and IP) holder is the the Chinese Communist Party. For avoidance of doubt:
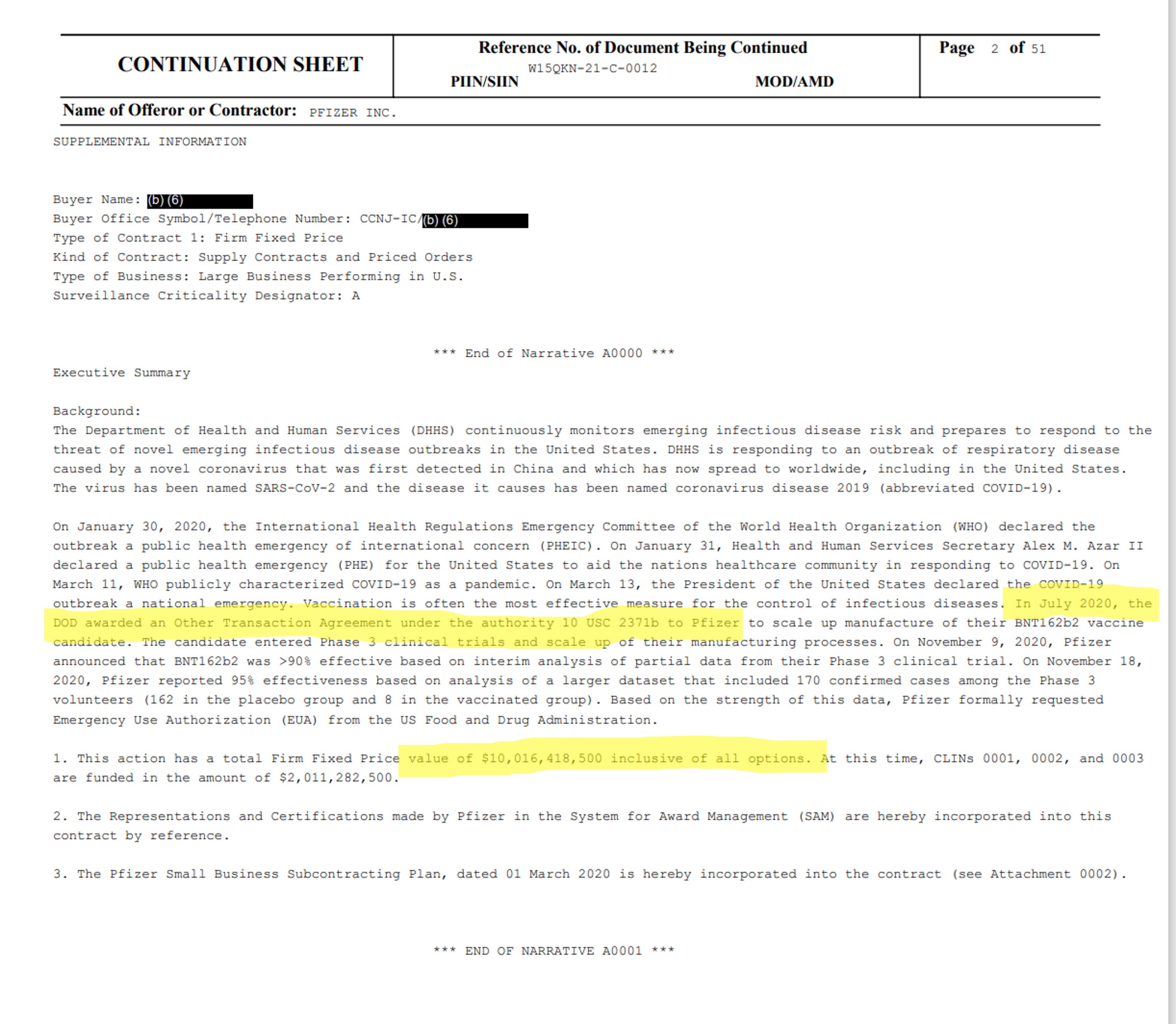
Below is the timeline of some of the key investments and R&D deals I was able to identify from public SEC shareholder disclosures, immediately preceding and following the “pandemic”:
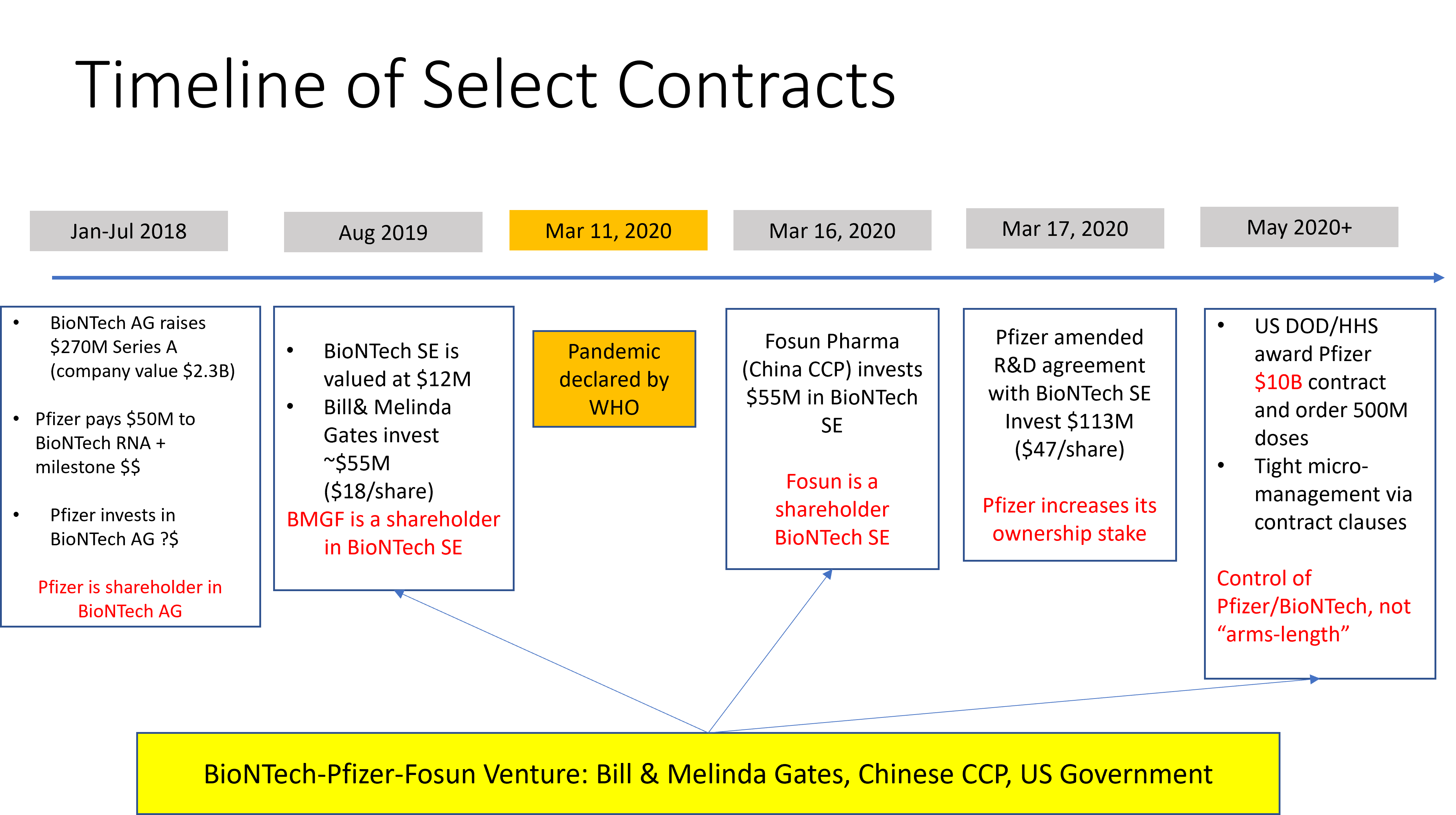
Just to make sure, we are talking about the exact technology in the mRNA shots. Here is the definition from March 17, 2020 agreement between Pfizer and BioNTech (p. 4):

The same document describes a data sharing agreement, “pharmacovigilance” globally among the 3 parties. They will count the bodies and share the data with each other:
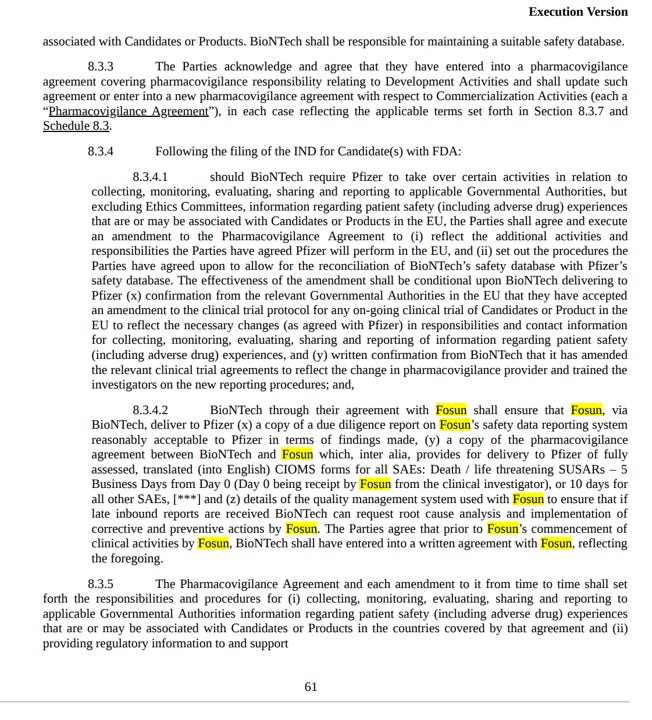
On the “pharmacovigilance” aspect, there is a 4th participant in this arrangement - the Israeli Ministry of Health, which entered into a data sharing agreement with Pfizer on January 6, 2021 and gave Pfizer (and by extension, US DoD and anyone who controls it, BioNTech and anyone who controls it, Fosun and anyone who controls it, i.e. CCP) access to all their citizens' centralized electronic health records. But don't worry, Benjamin Netanyahu promised to keep the data de-identified. Right.
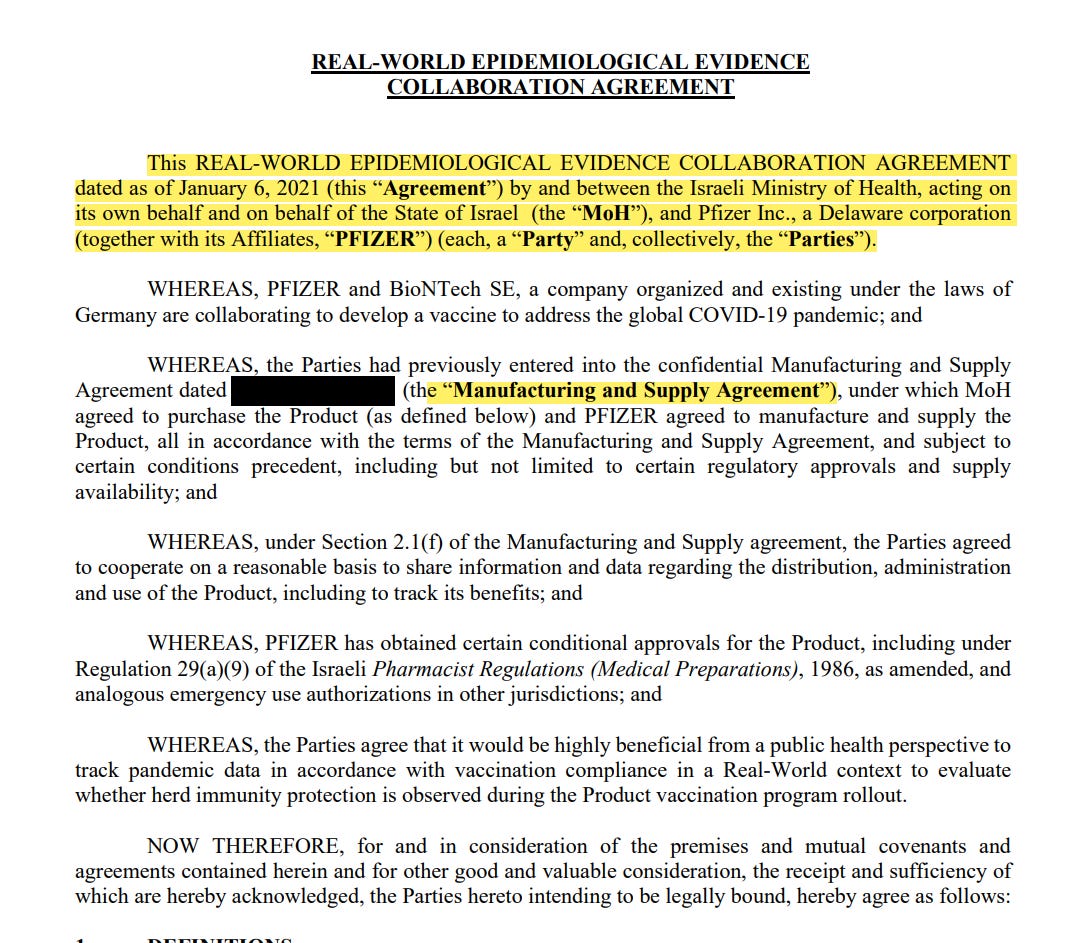
Side note - Israeli government recently “misplaced” the Manufacturing and Supply Agreement with Pfizer mentioned in the data sharing agreement above (so we know for sure it exists). The government sadly cannot find it for some reason\u2026
This gets even larger and more interesting when looking at the sources of “R&D” financing. Turns out, there were numerous financial backers and co-investors in the BioNTech “venture” in the years preceding the global fraud and mass murder exercise. According to Crunchbase, BioNTech, a tiny company with just a handful of employees and NO PRODUCTS or scale manufacturing, raised $1.7B in 9 rounds of investments since around 2008. Large portion of the money, $1B+ was raised before 2020. What was it for, since no big clinical trials or scale manufacturing was happening then? That's a good question, worth examining at some point. Cursory review of some of the investment rounds indicates wide and very international involvement of a variety investors from US, Europe, UK, Australia, South Africa, mainland China, Hong Kong and Singapore among others. These likely included many government actors: “sovereign” funds, pension funds and the like who often do these investments by allocating money to “private venture funds” (limited partners in a private venture funds are confidential). Maybe I will do a separate article on this at a later date.
Note, many people ask me “what about China and Russia?” when I talk about our own government and DoD engaged in mass genocide of Americans. I answered about China - they are allied with the US DoD on this. The CCP is profiting from the financial windfall of the US government printing dollars and throwing them into the mRNA furnaces where they are driving masses of the brainwashed citizens to suicide themselves. China claims to use “traditional vaccines” - if you believe what the Chinese say, I have a bridge to sell you.
I have not seen evidence of any similar alliance with Russia. This makes sense, because ultimately this boils down to the war of US vs Russia using proxies and alliances (as it always does). This does not mean that Russia are “the good guys”. Simply that the owners of Russia (whoever they are, not necessarily based in Russia) disagree with the owners of the US (whoever they are, not necessarily based in the US). Russia is running the same “covid script”, using knock off RNA/DNA injections, probably buying materials from the same suppliers, and also using war to kill off their own younger population. It's just that they are doing it for THEIR OWN interests, not that of the US and their allies.
Back to this western continent - we have already established that “Covid-19 vaccines” are biowarfare agents, legally not medicines, not pharmaceuticals, and not regulated as such.
Use of Emergency Use Authorized (EUA) covered countermeasures under a declared Public Health Emergency cannot constitute a clinical investigation (21 USC 360bbb-3(k)), therefore these countermeasures could not be tested for safety or efficacy in accordance with US law (21 CFR 312 and 21 CFR 601), nor could compliance with current Good Manufacturing Practices (cGMP) or Good Distribution Practices (GxP in general) be enforced by the FDA.
This legal fact was known to the US Government, DOD, BARDA, FDA, CDC, HHS officials signing the contracts, involved in the OWS, and it was also known to Pfizer, Moderna and other pharma companies. mRNA technology has always been designated dual-use, a category of bioweapons:
From the start, “covid pandemic” was treated by the US Government as a national security matter (i.e. war) and covid policy was set by the National Security Council (assemblage of Defense and Intelligence heads), not HHS.
March 13, 2020: “PanCAP Adapted U.S. Government COVID-19 Response Plan” (PanCAP-A) states that United States policy in response to SARS-CoV-2 is set not by the public health agencies designated in pandemic preparedness protocols (Pandemic and All Hazards Preparedness Act , PPD-44 , BIA), but rather by the National Security Council, or NSC. NSC does not have regular attendees from public health agencies and its focus is national security and foreign policy matters.\"
Below is the organization chart from the PanCAP-A document, p.9:
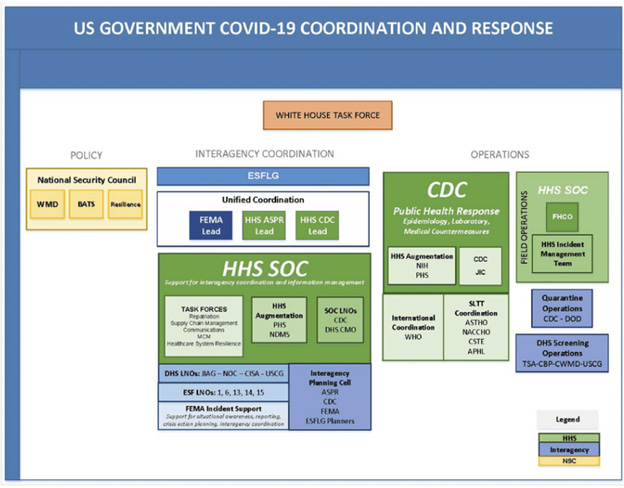
When a known weaponizable tech is given a liability-free, extrajudicial status shielded from all regulations, it's not hard to put 2 and 2 together. The national security, DoD and Intelligence officials absolutely knew all of this. They went ahead and authorized a $10 billion purchase order of this weaponizable tech from the Fosun-Pfizer-BioNTech enterprise (backed by numerous foreign governments including the Chinese), to deliver and deploy it onto Americans, during the time of war.
I think by now it should become clear that the “5th gen warfare” is not just the use of psyops and total control of social media by the FBI and CIA (that's so last century!) It's also not “profits over safety”, “bad FDA overlooked myocarditis” or “big pharma pays politicians for election campaigns”. We are way, way past that. I keep pointing out that if the motive were JUST PROFIT, then the most profitable strategy would have been to ship placebo. They would not be violating any laws by doing so, there would be no adverse events and deaths, the product would look perfectly cGMP compliant, while covid would have gone away quickly by itself. Yet, the governments (plural)-pharma cartel insists on killing and injuring millions of people, obviously limiting the profit potential by doing so.
The current war is the war of the global governments (plural), that only pretend to be at odds with each other, marketing themselves as “left”, “right”, “communists”, “green”, “capitalists”, “socialists”, “populists”, “conservatives”, etc. etc. in a never ending clown show of the political theater. Behind the scenes, the “official enemies” are partners and co-investors into “joint ventures” against us, people of the world. They use taxpayers' money to fund, develop, then “approve”, purchase and deploy prohibited biowarfare agents for killing and injuring their own civilian population, their own armed forces, first responders, healthcare workers, pregnant women and children . To stop this every one of us must start using correct precise language, start calling things what they really are.
This is the fourth part of a series in which Paula Jardine examines how the Covid vaccine programme was conceived by US defence planners nearly 20 years ago as a 21st century ‘Manhattan Project’ for biodefence. You can read Part 1 here, Part 2 here and Part 3 here.
BILL Frist was the 2003-2007 US Senate majority leader who championed the USA’s biodefence projects and promoted the concept of a ‘Manhattan Project’ against a pandemic, described in Parts 1, 2 and 3 of this series. He was also the politician who sponsored the Public Readiness and Emergency Preparedness Act (PREP) Act of December 2005 as soon as the World Health Organisation’s International Health Regulations had been amended to include a provision enabling WHO to declare Public Health Emergencies of International Concern (PHEIC). Critically it was this Act that established indemnity for the manufacturers of therapeutics, vaccines or diagnostics released during the course of a public health emergency against any and all harm caused.
Also working to influence US national biosecurity policy was Dr Robert Kadlec, described in Part 3. Working with him, and principally under the auspices of the Johns Hopkins Centre for Health Security (founded by Dr Tara O’Toole in 1998) were other participants in Operation Dark Winter, the code name for a senior-level situational simulation conducted on June 22-23, 2001, designed to wargame a covert and widespread smallpox bio-terrorist attack on the United States. These biosecurity hawks included O’Toole and Tom Inglesby of the Johns Hopkins Center for Civilian Biodefense Strategies (CCBS).
When O’Toole was nominated some years later to serve in the Department of Homeland Security in 2009, critics warned of her paranoia. Microbiologist Dr Richard Ebright, one of the scientists who, in May 2021, called for a full and unrestricted international forensic investigation into the origins of Covid-19, said it was a disastrous nomination: ‘O’Toole supported every flawed decision and counterproductive policy on biodefense, biosafety, and biosecurity during the Bush Administration. [She] is as out of touch with reality, and as paranoiac, as former Vice President Cheney . . . It would be hard to think of a person less well suited for the position . . . She was the single most extreme person, either in or out of government, advocating for a massive biodefense expansion and relaxation of provisions for safety and security’. Dr Ebright concluded: ‘She makes Dr Strangelove look sane.’
It was Kadlec who formed the Bipartisan Commission on Biodefense in 2014 and began the planning his Manhattan Project in earnest. Those involved with him in this commission included Tom Ridge, the first Homeland Security Secretary, Donna Shalala, a former Health and Human Services (HHS) Secretary, Dr Margaret Hamburg, a former Food and Drug Administration (FDA) commissioner, Scooter Libby, formerly of Project for a New American Century (PNAC), William Karesh, the vice president of EcoHealth Alliance and an adviser to the WHO on reforms to the International Health Regulations (IHR), and Kenneth Wainstein, now the Under Secretary of Homeland Security for Intelligence and Analysis.
The Commission’s National Blueprint for Biodefense published in2015 called for major ‘reform’. Consider it the blueprint for Kadlec’s Manhattan Project, for the CEPI (Coalition for Epidemic Preparedness Innovations) strategy and for the subsequent changes to the WHO IHR required to make the plan work.
The list of the BioDefense Commissions ‘we must’ demands follows:
· revolutionise the development of Medical Countermeasures (MCM, which are vaccines and therapeutics) for emerging infectious diseases;
· fully fund and incentivise the MCM enterprise;
· remove bureaucratic hurdles to MCM innovation;
· develop a system for environmental detection that leverages the ingenuity of industry and meets the growing threat;
· overhaul the Select Agent Program (which oversees the possession, use and transfer of risky biological agents and toxins) to enable a secure system that simultaneously encourages participation by the scientific community;
· help lead the international community toward the establishment of a fully functional and agile global public health response apparatus.
Three years later in May 2018 when Johns Hopkins ran Clade X, a table top simulation around a novel parainfluenza virus, O’Toole was involved once again. Johns Hopkins CHS also co-hosted with the Bill and Melinda Gates Foundation the better-known coronavirus simulation Event 201 in October 2019.
It was during a Clade X discussion on manufacturing capacity sufficient to end the fictitious pandemic through vaccination that O’Toole said: ‘Industry are more than willing to help but vaccines are very specific creatures that are difficult to turn to new purposes. We’re going to have to go to innovative manufacturing methods that will require a lot of leniency from the FDA and the understanding of the American people that we’re doing things on an emergency basis so every box in terms of safety and risk assessment may not be checked. But the vaccine is the only way forward.’ [My emphasis]
This was clear advocacy for vaccines as the exit strategy for the Clade X novel parainfluenza virus pandemic, and later once the Covid pandemic was underway, was to be the only exit offered to lockdown.
Today, O’Toole is an executive vice-president of the CIA spin-off venture capital firm In-Q-Tel in charge of a strategic initiative called BiologyNext. In April 2020 in a presentation to the Centre for Strategic and International Studies (CSIS) she said: ‘The bio-revolution is really founded on several core technologies that I’m going to simplify greatly. But it is all about being able to read, write, and edit the code of life. One of the most important recognitions of the past century in science, at least, is that life is written in code. And as Jason Kelly of Ginkgo Bioworks has put it: Biology is essentially programmable . . .
‘Ron Weiss, who is a synthetic biologist, predicted in 2014 that an RNA-based delivery method that allowed you to use RNA as a kind of platform to deliver new bits and pieces inside the cell would be a game-changing inflection point in synthetic biology. And the Covid-19 pandemic is giving us a chance to test that out. You may know that one of the vaccines that is coming on very quickly is made by Moderna. And it is a messenger RNA-based vaccine. So if that works, Ron Weiss’s prediction may come true.’ [My emphasis]
In August 2019 Kadlec’s department ran yet another table-top simulation, the Crimson Contagion. It simulated the impact of and response to the arrival in the US of an avian flu from China. It was a scoping exercise to identify legal authorities, US federal government funding resources and manufacturing capabilities for vaccines. It concluded that $10billion would be required to respond to a novel pandemic influenza strain.
A month later on September 19, 2019, President Trump signed the Executive Order on Modernizing Influenza Vaccines which launched the Manhattan Project by directing various US government departments and the US Department of Defense to propose a plan and a budget within 120 days – by January 17, 2020, to be precise.
Anthony Fauci’s diary, released following a freedom of information request, notes a teleconference concerning the ‘Global pandemic’ taking place on January 15, 2020, a date at which a global pandemic existed only in some people’s imaginations.
On January 23, 2020, after the Moderna vaccine announcement in Davos, Fauci had a conference call with Dr Richard Hatchett, CEPI’s CEO, and the following day, a Saturday, he had a senior leadership update with Dr Kadlec in advance of a meeting with Stephane Bancel of Moderna on Monday January 27. Perhaps Kadlec, Hatchett and Bancel were amongst the unnamed people on Fauci’s January 15conference call.
On January 30, 2020, when the WHO declared a SARS CoV2 Public Health Emergency of International Concern, just 7,818 patients were said to be sick with Covid, of whom only 82 were outside China. As far as Kadlec was concerned, this was now a shooting war.
Following CEPI’s announcement in Davos on January 23, US-based manufacturers Innovio Pharmaceuticals were miraculously ready to begin developing a Covid vaccine, and Moderna already had its funding to begin manufacturing the first batch of the vaccine co-owned and co-developed with Anthony Fauci’s National Institute of Allergy and Infectious Diseases (NIAID) for use in a human clinical trial.
The legislation that he and Frist had shepherded through Congress between 2003 and 2005 had concentrated power in the hands of the US Health and Human Services Secretary (and the US Administration for Strategic Preparedness and Response) during public health emergencies.
The basic goals of the architects had been achieved. These, the American investigative paralegal Katherine Watt has argued, were to set up legal conditions in which all governing power in the United States would be automatically transferred from the citizens and the three constitutional branches into the hands of one person, the Health and Human Services Secretary, ‘effective at the moment the HHS Secretary himself declared a public health emergency, legally transforming free citizens into enslaved subjects’.
The HHS Secretary Alex Azar, to whom ASPR’s Kadlec reported, was the senior legal counsel at HHS when the PREP Act was passed in 2005. Azar co-operatively declared a public health emergency on January 30, 2020, backdating it to January 27.
He then made a PREP Act declaration on February 4, enhancing liability protection for any person or firm involved in developing countermeasures, including Innovio and Moderna.
The announcement said: ‘The world is facing an unprecedented pandemic. To effectively respond, there must be a more consistent pathway for Covered Persons to manufacture, distribute, administer or use Covered Countermeasures across the nation and the world.’
HHS Secretary determinations are unreviewable by the US courts.
Further research by Katherine Watt into another PREP Act declaration for medical countermeasures by Azar in March 2020 shows it effectively sidestepped the Nuremberg Code by stipulating that the ‘use’ of any counter measures ‘shall not be considered to constitute a clinical investigation’ while also removing the right to informed consent. As there is, by decree, no clinical trial, there are no stopping conditions for the use of said countermeasures.
It is startling how Dr Kadlec and his few associates have, over a period of more than 20 years, managed to orchestrate an undemocratic and unethical bio-security coup with global reach.
The Manhattan Project was renamed Operation WarpSpeed when it was launched in May 2020. The involvement of the US Federal Government which through the NIAID owns the patent for the spike protein used in the vaccines, and its Department of Defense that ran and financed Operation WarpSpeed, arguably elevates this War on Microbes Manhattan Project to an unprecedented bioweapon attack on humanity using an under-tested novel injectable pharmaceutical.
This is the third part of a series in which Paula Jardine examines how the Covid vaccine programme was conceived by US defence planners nearly 20 years ago as a 21st century ‘Manhattan Project’ for biodefence. You can read Part 1 here and Part 2 here.
WHEN it comes to the business of vaccines and biosecurity, the land of free enterprise is all up for large-scale state intervention to create and prop up markets. Some of the generals behind the biosecurity ‘Manhattan Project’ believe the War on Microbes is too important to leave to politicians or Adam Smith’s invisible hand.
In June 2020, former Senator Bill Frist appeared before the Senate Health, Education, Labor and Pensions (HELP) Committee, reminding them he’d argued the need for this project fifteen years earlier.
‘I called for and had outlined “a greater than Manhattan Project for the 21st century” with no less than “the creation, with war-like concentration, of the ability to detect, identify and model any emerging or newly emerging infection, natural or otherwise; for the ability to engineer the immunization and cure, and to manufacture, distribute and administer whatever may be required to get it done and to get it done in time”,’ Frist told the Senate in his testimony.
‘We have a dangerously inadequate vaccine manufacturing base in the United States. This must be rectified. Bottom line: there’s so little profit and so much uncertainty in vaccine manufacturing today. We must establish longstanding public-private partnerships with industry that are sustained and are not at risk of disappearing with each [Congressional] appropriations cycle. We cannot expect the private sector to independently invest billions of dollars developing antivirals and vaccines for novel viruses that we hope we’ll never need to use. That’s not a sustainable business model.’
For some years to come, Frist asserted, this should be the chief work of the nation, ‘for the good reason that failing to make it so would be to risk the life of the nation’.
Whether this idea originated from Senator Frist is another matter. Dr Robert Kadlec, the ‘General Ripper’ behind this new Manhattan Project, was at that time the leading biosecurity official in President George W Bush’s administration. He was at the April 2005 National Academy of Sciences Pandemic Influenza Symposium where an unidentified participant called for funding for a Manhattan-like Project to protect against a pandemic, calling it an insurance policy.
But the groundwork for this Manhattan Project was being laid even earlier. In June 2001, two months before the 9/11 atrocity, the Johns Hopkins Center for Health Security (CHS) held a table-top exercise it called Dark Winter, simulating a smallpox bioterrorism attack on the US orchestrated by Osama bin Laden’s Al Qaeda. Dr Tara O’Toole, who founded the CHS in 1998, was the principal designer of the exercise, butKadlec is credited with giving it its name. AColonel Randall Larsen, who’d hired Kadlec to work at the Air War College in the mid-1990s, was another designer of the exercise along with Tom Inglesby, the CHS’s current director.
Kadlec became the Homeland Security Director of Biosecurity Policy in January 2002 and soonafter attempted to restart the smallpox vaccination programme. In 2004, he launched Project Bioshield, a $5.6billion ten-year programme which created BARDA, the Biomedical Advanced Research and Development Authority. This was intended to motivate US pharmaceutical companies to start developing biodefence products (medical countermeasures which are principally vaccines) ‘by providing a substantial guaranteed market, expediting governmental contracting practices and clarifying FDA regulatory requirements for products used in a public health emergency’.
Project Bioshield funding enabled the US government to stockpile smallpox and anthrax vaccines manufactured by the companies Bavarian Nordic and Emergent BioSolutions. Both companies and the industry lobby group Biotechnology Innovation Organization were amongst the funders of Kadlec’s Bipartisan Commission on Biodefense he founded ten years later, in 2014, when he was working as a paid consultant to Emergent BioSolutions.The company, founded by Fuad El-Hibri and originally known as BioPort Inc, purchased a vaccine factory and the rights to manufacture anthrax vaccine for the US military in 1998.
On his appointment as Assistant Secretary for Preparedness and Response (ASPR) in 2017, Kadlec failed to declare a conflict of interests on his ethics forms, that in 2012 he and El-Hibri had co-founded an international biodefence company called East West Solutions LLC or that he had been employed by Emergent BioSolutions as a consultant. https://www.help.senate.gov/imo/media/doc/05062020%20Kadlec%20Ethics%20Letter%20Updated%20signed%20pdf.pdf In September 2019, when Kadlec was ASPR and in control of the US national stockpile, Emergent BioSolutions was awarded a ten-year $2billion contract to replenish the US national stockpile of smallpox vaccine.
Emergent BioSolutions was later subcontracted to manufacture Covid vaccines for AstraZeneca and Johnson & Johnson in the US. However the company’s poor manufacturing standards led to a Congressional investigation being launched in 2021.
Since Covid, the ‘war on microbes’ has not let up: attention simply moved on to the next opportunity to promote a vaccine. Each outbreak seems to follow the oft-repeated pattern of having been preceded by a Strangelove-like situational simulation based on a fictional scenario. Outbreaks of disease, requiring the WHO to declare a public health emergency of international concern (PHEIC) and public health authorities to announce a vaccination campaign, have a strange knack of occurring soon after the simulation exercises, ensuring the public health community is well prepared in advance.
In December 2020, the Nuclear Threat Initiative (NTI), whose interim vice president is the former US Department of Health and Human Services Secretary Margaret Hamburg, conducted a consultation with experts for a table top exercise on ‘reducing high-consequence biological threats’ in preparation for the exercise to run at the Munich Security Conference in March 2021. The scenario involved a fictitious monkeypox outbreak. Hamburg was herself a player in the June 2001 Dark Winter smallpox table top exercise and is a member of the Biodefense Commission. At the 2021 Munich monkeypox simulation she was joined by a familiar roster of biosecurity figures including the ubiquitous Sir Jeremy Farrar, his old friend George Gao, the then head of the China CDC, Dr Chris Elias of the Bill & Melinda Gates Foundation, US Senator Sam Nunn who played the President in Dark Winter, Luc Debruyne, Vice President of CEPI, Dr Michael Ryan, Director of the WHO Emergencies Programme, with whom Anthony Fauci was in weekly contact in early 2020 during the time that Covid was escalated to a pandemic, and Arnaud Bernaert the WEF’s Head of Shaping the Future of Health and Health Care.
Bernaert, Gao and Elias were involved in Event 201, the coronavirus table top exercise co-sponsored by the Johns Hopkins Centre for Health Security, the Gates Foundation and the WEF in October 2019. In the WEF press release for Event 201 Bernaert said, ‘We are in a new era of epidemic risk, where essential public-private cooperation remains challenged, despite being necessary to mitigate risk and impact. Now is the time to scale up cooperation between national governments, key international institutions and critical industries, to enhance global capacity for preparedness and response.’
In May 2022, the WHO declared a monkeypox outbreak which was escalated to a full-scale Public Health Emergency of International Concern in July 2022. Bavarian Nordic, the Danish headquartered vaccine manufacturer belonging to a Washington-based consortium called the Alliance for Biosecurity, signed a contract with an unnamed European country to supply smallpox vaccines for use as a monkeypox vaccine. The company is a sponsor of Kadlec’s Biodefense Commission, and its largest shareholder is ATP, Denmark’s national pension fund. Other notable entities amongst its top five shareholders include Vanguard Asset Management and Norway’s sovereign wealth fund Norge Bank.
In Part 4 I will examine how Kadlec began preparations for his Manhattan Project two years before the 2016 US Presidential election.

This is the second part of a series in which Paula Jardine examines how the Covid vaccine programme was conceived by US defence planners nearly 20 years ago as a 21st century ‘Manhattan Project’ for biodefence. You can read Part 1 here.
THE name Robert Kadlec may mean nothing to you, but anyone who has watched Stanley Kubrick’s Cold War era satirical masterpiece Dr Strangelove will quickly get the idea of who this man is.
Colonel Kadlec is the General Ripper of the War on Microbes. It is no small irony that the Biodefense Commission that Kadlec set up in 2014 is funded by the Hudson Institute, which was co-founded by Herman Kahn, the Rand Corporation war gamer. Kahn’s theory that nuclear war could be deterred if the Soviet Union believed the United States had second strike capability was the inspiration for Kubrick’s Dr Strangelove character and the film.
Kadlecbegan his career as an Air Force physician before he diverted into the world of biological weapons during the first Gulf War of 1990-91. He became an intelligence analyst for the US Joint Special Operations Command (JSOC) on chemical and biological weapons. He subsequently became a member of the UN Weapons Inspection team in Iraq led by Dr David Kelly, who was found dead in 2003.
Kadlec was later (2014) to tell the House of Representatives Committee on Homeland Security that ‘while the United States was victorious in 1991, the scale and scope of Iraq’s biological weapons programme remained elusive despite the most intrusive inspection and monitoring regime ever conceived and implemented by the United Nations Special Commission (UNSCOM).’
No conclusive proof was ever found that Iraq had biological weapons, but testimony in 1995 from a defector, Saddam Hussein’s son-in-law Colonel General Hussein Kamel Hassan al-Majid, intelligence which was later assessed as being of limited content and value, maintained the belief of Kadlec and others that they did exist, providing the pretext for the 2003 Iraq War which removed Hussein from power. This belief was no doubt bolstered in part because in the 1980s the Iraqi Technical and Scientific Import Division had (quitelegally) bought samples of an anthrax strain developed by US germ warfare researchers at Fort Detrick, from the American Type Culture Collection, a non-profit organisation in Manassas, Virginia, that provides samples of bacteria and viruses for scientific study. (Arguably the absence of concrete evidence reinforced rather than diminished this belief in the graveness of the threat.)
Between 1993-96 Kadlec served on the US Delegation to the Biological Weapons Convention. His thinking on biowarfare is set out in his contribution to a 1995 Air War College book called Battlefield of the Future.
In it he argued that biological weapons are the poor nations’ nuclear bombs: they could be made cheaply and easily in facilities with other legitimate purposes, are invisible and, if aerosolised, could be spread over wide areas using an agricultural crop duster. His contention was that they uniquely offered the possibility of ‘plausible deniability’ to the perpetrators because pathogenic agents could be mistaken for naturally occurring epidemics. His particular concern was that vaccines, which are highly specific in what they protect against, take ten to 15 years to develop.
Wired magazine reported on the US military’s desire for genetic vaccines to make soldiers ‘immune to all known pathogens’ in 1996. As if that wasn’t enough of an aspirational Pandora’s Box, it also reported the military’s desire for the capability of targeting enemy leaders using genetically engineered super pathogens ‘so selective in their behaviour they’re capable of targeting specific individuals, verifying their identities by means of their DNA sequences’.
It was immediately after 9/11 in 2001 thatKadlec became a special adviser to Defense Secretary Donald Rumsfeld and subsequently appointed Director of Biosecurity Policy in the Homeland Security Department of President George W Bush, where he drafted a document calledNational Biodefense Policy for the 21st Century. This, in April 2004, became the Homeland Security Presidential Policy Directive 10. Kadlec wrote that theUnited States ‘will continue to use all means necessary to prevent, protect against, and mitigate biological weapons attacks perpetrated against our homeland and our global interests’.
Speaking about the need for a Homeland Biosecurity Policy,President G W Bush said: ‘Armed with a single vial of a biological agent, small groups of fanatics, or failing states, could gain the power to threaten great nations, threaten world peace. America, and the entire civilized world, will face this threat for decades to come. We must confront the danger with open eyes, and unbending purpose.’
Notably Kadlec’s 2018 update of this policy went much further. It declared the extraordinary intent to apply the US approach to countering weapons of mass destruction to all infectious disease outbreaks, naturally occurring or otherwise.
Returning to 2005, this was the year that saw Kadlec attending a National Academy of Sciences Symposium on Pandemic Influenza. This centred on the belief of American public health authorities thatthe recurrence of an influenza pandemic with high mortality was both inevitable and posed a grave threat to humanity. Becauseinfluenza rapidly mutates and is not usually particularly lethal it provideda good research model for biosecurity purposes, not to mention a useful tool for advancing policy objectives. The ubiquitous Imperial College London modeller Neil Ferguson told the symposium that disease containment required ‘a concerted international response – probably with teams on the ground chasing cases’, effectively laying the groundwork for ‘all means necessary’ not to stop at the US border.
Though the 1918 influenza pandemic was originally said to have been caused by H1N1 swine flu, today the US Centers for Disease Control (CDC) says it was caused by ‘H1N1 with genes of avian origin’. This is based onUS Army researchers who claimed in 1999 to have fully sequenced ‘Spanish Influenza’ (using PCR) from autopsy samples taken in 1918 and a sample retrieved from a victim buried in permafrost since 1918. They said the illness was more closely related to avian flu than any mammalian species.
Ferguson’s modelling on avian flu was published in August 2005, claiming that ‘if targeted action is taken within a critical three-week window, then an outbreak could be limited to fewer than 100 individuals within two months’, but if unchecked up to 200million could die. This was just one of his wildly improbable and spectacularly wrong forecasts.
It was claimed that if bird flu mutated to more readily infect humans, the mortality rate would be more than 50 per cent. Bird flu, which first appeared in Thailand’s huge commercial poultry flocks, serendipitously appeared just as an eight-year marathon effort to have the World Health Assembly of the WHO agree key amendments to the International Health Regulations was coming to a close. The significance of these amendments, finally adopted in 2005, is that they included a new provision toenable the Director General to declare Public Health Emergencies of International Concern (PHEIC) on the recommendation of the WHO Emergency Committee. This mirrored the Public Health Emergency provision added to American public health law in 1983. Covid was declared a PHIEC by the WHO on January 30, 2020.
From 2003 to 2007, only 216 people died from bird flu. The threat and the headline fatality rate appear to have been overstated. Dr Nguyen Tuong Van of Hanoi’s Institute for Clinical Research, who treated some bird flu victims during the 2004 outbreak said, ‘Most people who die of bird flu are poor and not in the best physical condition in the first place.’
Jeremy Farrar’s 2004 paper on the Vietnamese outbreaks says rapid antigen testing was ‘less sensitive than PCR for diagnosis of influenza H5N1.’ Patients were given anti-viral drugs, mainly Tamiflu, which was developed by Gilead Sciences, a company chaired by Donald Rumsfeld, and almost all were mechanically ventilated, which itself elevates the mortality rate. Tamiflu may have been part of the problem. As a recent review of Tamiflu concludes: ‘A cocktail of pandemic panic, publicity propaganda, and scientific misconduct turned a new medicine with only modest efficacy into a blockbuster. It appears that the multiple regulatory checks and balances gave way as science lost its primacy and pharmaceutical enterprise lost no time in making the most of it.’
The 2005 WHO report Avian Influenza: Assessing the pandemic threat itself makes curious, and occasionally implausible, reading. According to this account, the ‘highly pathogenic’ bird flu, as it was usually described, was being spread asymptomatically by wild waterfowl (airborne bioterrorists to Kadlec’s way of thinking) to the small domestic free-range flocks kept by rural families in Asia, and that these birds were transmitting it to people. The real problem according to the business end of the report was that H5N1 bird flu was so ‘highly pathogenic’ that it was killing the chicken embryos used for flu vaccine manufacture. This made finding new methods of manufacturing them all the more desirable. Even better if these new methods could produce more vaccines, faster.
Another conundrum, Dr Jesse Goodman of the FDA told the NAS symposium, was the markets. ‘Markets – that is demand and sales – are the main drivers of manufacturing. No one is going to build factories just for a possible pandemic,’ he said.
The WHO had convened a meeting in November 2004 with all the major vaccine manufacturers to explore ways in which industry, regulatory authorities, governments, and WHO could collectively speed up the development of pandemic vaccines that could be made rapidly and in as large a quantity as possible. It was argued that wider use of seasonal vaccines would make the vaccines more commercially viable and the resulting increased production capacity would enable manufacturers to pivot production to pandemic strains whenever they should be needed.
Senator Bill Frist, the Republican Senate Majority leader at the time Kadlec was the leading bioterrorism expert in the Bush Jr Administration, full-throatedly echoed Kadlec’s thinking at the 2005 WEF at Davos, saying: ‘The greatest existential threat we have in the world today is biological. Why? Because unlike any other threat it has the power of panic and paralysis to be global.’ He also asserted: ‘We need to do something that even dwarfs the Manhattan Project,’ the codename for the US effort to devise an atomic weapon during the Second World War.
Next: Kadlec’s simulation exercises and his conflicts of interest.

This performance was March 28 1983, exactly 40 years ago! English lyrics:
If you have some time for me
Then I'll sing a song for you
Of 99 balloons
On their way to the horizon
If you're thinking of me
Then I'll sing a song for you
Of 99 balloons
And that something comes from something
99 balloons
On their way to the horizon
Thought to be ufos from outer space
So a general sent
Sent an air squadron after them
To sound the alarm, if it were so
But there on the horizon
Only 99 balloons
99 jet planes
Each one was a great warrior
Thought they were Captain Kirk
There was a big fireworks show
The neighbors didn't get it
And felt like they were being picked on
And on the horizon they shot
At 99 balloons
99 ministers of war
Matches and gas cans
Thought they were smart people
They smelled a fat prey
Shouted war and wanted power
Man, who would have thought
That it would come to this
Because of 99 balloons
99 years of war
Left no room for victors
There's no more ministers of war
And no more jet planes
Today I make my rounds
I see the world in ruins
I found a balloon
Think of you and let it fly

Introduction
Recently, there is a lot of talk about where the escalating spiral will end. Will it conclude in World War III? Will there be a nuclear war? What are the determining factors? And what would indicate World War III is imminent? I'll go through these questions in detail from a strategic perspective.
But, before I do, I'd like to write another short dedication to an author and analyst, that I value very much. I'm talking about Andrei Raevsky, better known under his pseudonym “The Vineyard Saker”. I've read his blog regularly since 2015, and before that for years occasionally. I learned in this time a lot from him with regards to strategic and comprehensive thinking. This is what he does wonderfully. Unfortunately, but understandably, he decided to stop maintaining and writing his blog. Thank you, Andrei, for everything, for recommending my blog and for all the analysis I/we have been able to read for years and even decades. All the best for you and your family, going forwards.
So, will there be a third world war? I would say yes, with absolute certainty. But there are a few questions left that need to be clarified before we start to panic. I personally, currently, see no need for panic. Yet. But about which questions do I speak? About the following:
-
When will WW3 break out?
-
Under which circumstances?
-
Which alliances will participate?
-
Where will the main battlefield be?
-
Ultimately: Will the big three powers directly clash on a large scale against each other?
I don't have answers to these questions. But you can see that these are strategic questions, not operational questions, such as those we are currently considering in Ukraine. I don't think that the operational questions, whether 100 tanks will be supplied to Ukraine, or even 200 fighter jets, will decide anything about the likelihood of World War III.
What I hope to do here is to help readers develop their strategic thinking so that they can see past the short-sighted operational questions I mentioned before.
Preconditions
We at BMA developed a strategic and operational picture that is still valid. In fact, we can say that from my last operational update, there is nothing to add. I can go even further. I see now, step by step, all the major and well-known podcast analysts jumping on my train. All are now talking instead of big arrows, of methodical grinding on several theatres, to put as much pressure as needed on the Ukrainians so they can collapse. That's perfectly fine for me.
For people, that haven't read my analysis yet, I strongly recommend reading the following articles in this sequence:
Further weapon shipments
Let's start with weapon shipments. We will see later in this article, that I assume, that the war has escalated far more than both sides would have ever thought. From my personal standpoint, I assume, and it could have been observed in my former articles, that Russia planned with escalations up to the destruction of the third iteration of the “Ukrainian” army.
-
First iteration:
Destruction of the initial Ukrainian army. (Until April 2022)
-
Second iteration:
Destruction of the Ukrainian army, equipped with Western light equipment, designed to buffer off Russia, until the “third iteration” has been trained and equipped abroad. The second iteration had been defeated until the end of July 2022.
-
Third iteration:
Soldiers trained abroad and equipped with all the weapons, that countries with old Soviet stockpiles could have spared.
Destroyed at the day, General Gerasimov took over command of the SMO. 11th of January 2023.
-
Fourth iteration:
This army is currently in the making and is already partially fed into the battle to prevent the frontlines from collapsing. Which exactly is their purpose. To keep the battle (Scorched Earth) up as long as physically possible.
This army consists of two components, which should make sure, that this goal will be achieved.
- Professional army:
People that are mobilised since a few months and trained abroad, will make the professional part of this army. These are mainly “ideologically confused, highly motivated” people. There is also one single word for this.
They will be trained on new western weapons and equipment. There is a high probability, that the initial plan, a few months ago, has been, to use them for another offensive, to produce another “defeat” for the Russians before the total collapse of Ukraine. But as it looks, the events have been faster.
There certainly is no room any longer for any kind of offensives. This units will most likely be used for operational mobile defence. In other words, they will be used, where it hurts the most, to slow down the collapse. See BMA's five theatres. The big question is, will this army be used wisely on the West side of the Dnieper in a mobile way, to inflict the most possible damage to the Russians, or will it simply be fed into the Donbass meatgrinder and be buried along with the Ukrainian state?
- Forced conscript army:
As far as I can remotely judge it, I have the feeling that all “ideologically confused highly motivated Ukrainians” are “depleted” or in the process of being depleted within the fourth iteration fire brigade. See above.
One of the reasons of course is, that the government's propaganda, that the Ukrainian army had almost no losses, has fallen apart. It is now very well known within Ukraine that everyone who is drafted will either die, be seriously wounded or, in the best case, become a Russian POW.
There won't be anything else left, because one of the goals of the Russians is the full physical annihilation of the Ukrainian army. Which will be achieved until summer 2023. Until then everyone will be dead, wounded or captured. There may be some hardcore “ideologically confused and highly motivated” people that continue fighting, but they will only act on their own, not as part of an organized military.
Having said that, we can come back to the conscripts. Since no one wants to die for a lost cause (they know now that it is over and only the dying is left to be done), Ukrainian men are now hiding or otherwise trying to evade the draft. There are now mobile “conscription” teams scouring every city to catch men under any circumstances. The goal of depleting every able-bodied male Ukrainian is still active.
Well, these unmotivated people, to put it mildly, will be thrown into trenches to buy time. They have no other prospects than to either be killed or, if they are lucky, captured by the Russians.
This is the fourth iteration of the Ukrainian army. The last stand, so to say. One component should buy time by trading blood, the other component should inflict damage on Russia.
This is the last iteration. There are no more human resources left, after this “Volkssturm” mobilisation, to carry on the fight. As I pointed out several times, Ukraine will experience this collapse by summer 2023.
What does it have to do with further weapon deliveries?
Well, the war can only be continued if these last Ukrainians have armoured vehicles. The “confused” Ukrainians are still believing in a victory with Western equipment. They wouldn't continue the fight or charge Russian positions on their bare feet, without armoured assistance.
The following circumstances apply:
-
The whole Soviet stock of NATO and Ukraine is depleted.
-
The biggest part of the Ukrainian manpower is depleted.
So, a new “Frankenstein” army is being built with all kinds of NATO stuff, to keep the Ukrainians motivated to die for the West. Frankenstein, because it is an incompatible mix of everything, that has no battle value without combined arms ability.
Considering the current state of the Ukrainian army, nothing can help. In fact, it doesn't matter anymore what the West is delivering. It has zero impact on the outcome of the war. It is only a motivator and enabler for the Ukrainians to keep up the fight, until the last “mobilizable” men are killed or captured. It will fully achieve its goal.
Moreover, it will mean far more dead Russians, since the prolongation of the war means far more dead Russians. Which is NOT good.
Red lines
What about red lines? There are red lines indeed. But I don't think that Russia is measuring them by the amount and quality of tanks or planes, that are being sent by the West.
I'm personally convinced that the red lines were agreed by Sergei Naryshkin and William Burns in Ankara on November 14, 2022. And these red lines, from my point of view, concern the control and security of territory after the war.
In fact, I assume that all kinds of weapon deliveries would be “tolerated”, but not with pleasure, by the Russians, as long as there is no risk of lost territory. And Ukraine as a whole, except for places that could be negotiated away to other countries, is being considered as Russian territory.
Why is it accepted? The Ukrainian army is mostly defeated. Russia is fighting against the fourth and last iteration. The best people are already dead or have fled. And there is another major reason. I will cover it in the chapter “Wounded animal”.
The last point, I want to cover in this chapter is Germany. Germany of course is being forced to send its tanks to Ukraine. It will have no military consequences, but the calculation is, that Russia would escalate and break up relations with Germany for all times, because of history. The United States desperately wants to destroy the relations between Germany and Russia forever. So, Germany would depend on America and wouldn't benefit from the new BRICS/SCO-oriented multipolar world order.
Here are some personal thoughts and assumptions:
-
Germany wants Ukraine to collapse ASAP, so they come out of the hellish situation, on which they are forced in, by America.
-
Russia knows this and keeps backchannel doors open to Germany to manage the transition away from the American grip. I assume the tank deliveries won't change much if there are no further escalations. However, if NATO troops are part of the escalations, we are in WW3.
The West
The West is currently in sharp decline. Economically, militarily and politically.
Nevertheless, we mustn't forget, that the West has been the dominant power for decades. So, of course, it accumulated a lot of wealth and a large military. And now we come to the problem. Russia, more or less, openly worked on implementing the new multipolar world order around BRICS and the SCO. The Americans were aware of this. At the same time, the American empire, carrying on the work of other empires before it, has been working for the destruction of Russia. Therefore, the strategy to turn all former allies and Soviet States around Russia against them and then trigger the internal collapse in Russia.
Well, both Russia and America activated their corresponding plans in 2022. Everyone wants something, but only one side will prevail. Who wins in Ukraine will achieve its geopolitical goals. At least, that's what the parties believe. As of now, it should be clear to the politicians and secret services of all Western states, that it is over. Ukraine will soon fall, and with it, the single-polar American-centric world order.
Russia won't be destroyed.
Goals
What now? Well, the Americans know very well about their fate since their plan in Ukraine failed. Which doesn't need to be the end of the USA. They can become normal and powerful members of the future multipolar world order. Sitting at the table with the other great powers. I think, there are two possible outcomes.
-
Exactly this scenario. America becomes a “normal” multipolar power at the table with others. A single new world system emerges, which is controlled by an organisation and not by states. Either a new kind of UN/League of Nations, or a fundamental reconstruction of the UN and purge of “Western” “influence” and “Influencer”. Hence, the “De-Westernification” of the world.
-
America could decide, to stay an “opposite-pole”, against the multipolar world order. Then we would have two systems at the same time, competing against each other. The rest of the West and the BRICS/SCO states, competing and struggling for the contested bloc-free markets, until there is no bloc-free nation left.
Unfortunately, I assume, that option two will prevail. Which is the worse option for the world and humankind.
What are the goals of such an America (The West)?
-
Completely draining power from all its colonies and making them completely dependent on themselves. To secure markets and territory, for the future struggle against the powers of the Heartland. At the same time weakening the Heartland, since Europe is an integral part of it, with a huge potential, if managed correctly.
-
The depletion of the weapon stocks of Europe has the positive side effect that all these weapons will need to be replenished. Since the industrial production costs rose sky-high, for example, because of the blowing up of the gas pipelines (what a coincidence) and many other self-defeating reasons, Europe will struggle to reproduce these stocks themselves. The rationale is, that they will come to America and beg for “cheap” weapons.
In fact, America is raping Europe and is forcing them to come back to them and beg for more. Perversion. Or how does Scott Ritter say? Odious!
Wounded animal
Most likely the West didn't expect that the war would develop as it did. I wrote several times about it. First, they expected that Ukraine would fall within days and then they would organize a guerrilla war. Then, after they saw that Russia was not waging a strategic doctrinal offensive but a SMO, they thought, the West will win.
But none of it is true. Neither did Russia win within days, nor will it lose. In fact, it is defeating the West, its armies and economies in Ukraine. Who would have thought that?
America knows very well what its new role will be, so they are preparing for it by making Europe totally dependent on them, deindustrializing it and draining it for the next decade. Not only Europe, but all other colonies as well, including Canada, Australia, Japan, South Korea, etc.
Here is the problem. Since America is well aware of its impending downfall from a superpower to a normal but powerful nation, it struggles with a certain syndrome. When everything is well, all are happy and are competing to claim the success for themselves. When things go south, then the opposite applies. Everyone tries to blame the other. Which is currently the case in America. I will write a separate article about America. So, I'll go here quickly over it.
There is not one single power that is determining the course of the United States. The ruling oligarchy (the politicians are only “sponsored executioners” of the oligarchy) doesn't know exactly which way to go. There are powers that want to choose option 1, away from the empire and towards multipolarity and there are also powers who don't want to go down without a fight. Unfortunately, the majority of the establishment or oligarchy are supporters of the second option. And here we are. America is acting exactly as a wounded wild animal. It is biting, fighting and scratching everyone around it. Which is extremely dangerous for humankind. One mistake, and everyone dies.
This is what we see in Ukraine. Now, everything short of nuclear weapons will be delivered, what could be handled by the few capable Ukrainians left. And it would be idiotic by Russia to make a big deal out of it. It will be managed. Escalation management. Yes, a few thousand Russians more will die. Or if you count the Ukrainians as Russians, a few tens or hundreds of thousands more. But still, the world will survive.
It is up to Russia and the other civilized people to handle the rage of this wounded animal and contain it, so we won't need to use nuclear weapons or kick-off WW3. That's why Russia is taking many hard punches, without responding.
Challenge
The challenge is for Russia to win the war in Ukraine without escalating too much, to not trigger any reactions from the West, that could still trigger WW3, over Ukraine.
Currently there is no potential for such an escalation if we consider only the Ukrainian and the Russian army. The Ukrainian Army is soon (by the end of the summer 2023) gone. But the Americans could decide to sacrifice the European armies against Russia as another proxy force. Without American involvement.
It is not impossible, even though I think that the probability is very low.
Think of Polish and other European countries sending own troops to defend Western Ukraine, Odessa or Kiev.
People don't want it? There is not such a mood? There are no weapons? Who cares?
Create enough false flag operations within the EU and NATO, activate a large media campaign and you will have fanatical Europeans cheering for war and volunteering to march on Moscow.
Such a scenario needs to be avoided. It is called “escalation management”.
Why did I write that Americans would use the Europeans as a proxy force? Well, Europe is no longer interesting for America. They are pivoting to the new hot spot for trade, Asia. Europe is done. It can be used like a used condom, to further weaken Russia. Throwing old stuff and human waves against the Russians is creating losses for Russia. Both, in people and economically. Learn about opportunity costs. These are costs or revenues, that you did not achieve since you chose to do something less favourable. Hence, Russia could prosper by developing trade and relationships with the “New World”. But instead, it would need to fully mobilize and put a huge part of its resources, money and welfare into the military and war. While other market actors are exploiting the absence of Russia on the world markets.
Horror scenario? Yes, but I don't believe that it will materialize.
Indicators
But we need to discuss it. We are talking about a wounded wild animal. Its actions are totally unpredictable. And it is always doubling down. So, nothing can be excluded. We should be aware of it. And that's why I decided to write down some important indicators, which would indicate, that a threshold has been crossed, where there is no return.
-
Overt or covert mobilisation efforts within the big European countries.
-
Overt or covert transition to a wartime economy/production within the big European countries.
-
If the number of mobilized troops of Russia exceeds more than one and a half million men. I'm talking only about the mobilized. Not about the already standing conscript and professional peacetime army.
-
Calmness of Vladimir Putin is gone for a longer time. In fact, he would be visually very angry and his rhetoric would reach levels, never seen before. See his behaviour from November 2021 until February 2022, for a small version of what we would see.
-
Active and official participation of NATO troops in hostilities against Russia.
-
Officially breaking off relations between Russia and major NATO countries. Withdrawing of diplomatic missions and personnel, etc.
-
Total severing of all economic relations.
-
Russia withdrawing from many not-crucial markets without visible reasons.
-
Russia withdrawing from Syria.
-
Overt or covert full mobilisation in Russia.
-
Withdrawal of the Americans from important and major regions without a clear reason. Say, a sudden withdrawal of the Americans from the Middle East, including its navy. The Americans would try to bring as much equipment and as many troops as possible out of harm's way before the Russian barrages start to hit American bases worldwide.
Important factors
As I said. I want to be honest, I think, and this is only my assumption\ߪ It is too late for triggering WW3:
-
The Ukrainian human potential is almost gone. And soon it WILL BE GONE.
-
The Europeans have been demilitarized. And they will be demilitarized further until this is over. There is not much which could be used to actually fight the Russians.
-
The Americans would withdraw its equipment to America or Asia. This is an important region. Europe lost its significance, and with it, the obligation to NATO.
-
Article 5 says that the allies should consult on whether and how to support the member under attack. The decision of the single member states could be to send medical equipment or simply to do nothing. This applies to America as well. America wouldn't do much for Eastern European states. And it certainly would NOT fight Russia over them. I'm not yet sure, about central and west Europe, since America will need them, for reindustrializing over their resources and industries.
-
Until this war is over, NATO will only be four letters on a piece of paper. To be honest, I didn't expect it that way. I will point out my assumption, how NATO could be dismembered, in the “strategic outlook” chapter. But as it turns out, the NATO military branch will soon be done and gone. Left will be a club of people, that are meeting regularly to issue some threats out of a parallel universe in the direction of Russia. As I said, I'll go deeper into this later.
I want you all to keep in mind, what the ultimate goal of Russia is. Russia's ultimate goal is to secure its strategic security in the western direction, by forcing the West to accept the new draft treaty for European security. Either voluntarily or by force. Force can be military, economic or revolutionary. Don't forget that part. In case of failure, we all are simply going to die. \&#D83D;\&#DE0A; I pointed out the process and the reasons in detail in my analysis of Phase 3.
As I pointed out in the quoted article, who is cheering for Russia to lose, is cheering for his own death.
The lynchpin \ߝ Odessa
The strategic lynchpin, whether there will be a Ukraine, going forward, or not, is Odessa. With Odessa, Ukraine could sustain some kind of economy, by accessing the Black Sea. Probably it would be enough, to continue an existence as a classic American failed state, like Libya and some others that I won't name so as to not insult the people living there.
If Russia takes Odessa, or defeats the Ukrainian army somewhere else, so that Odessa could no longer be defended, then the war is over. Odessa is more important to Ukraine than Kiev itself.
Odessa is also one of the strategic goals, named by President Vladimir Putin, before he started the SMO. One of these goals is to bring justice to what happened in Odessa in 2014, when some fifty Russians were burned to death by Ukrainian nationalists. It is a personal goal of Vladimir Putin to take the city and seek justice for these deaths. Here are more reasons:
-
It is a strategic city. Without it, there could never be something like “Ukraine” again. It wouldn't be economically sustainable.
-
It would give Russia the control of a big part of the Black Sea. In fact, Russia's dominance in the Black Sea couldn't be contested anymore. Not only not from the Sea, but also not from the land or air.
-
Russia would have a deep outpost within the east flank of NATO, which is crucial. Think of radars, air bases, air defences, missile bases, fleet bases, marshalling grounds, etc.
-
Odessa is a Russian city. Not just any Russian city. It is a highly important Russian city. It was built by a very popular Russian emperor, Katherine the Great. Moreover, it is a hero city. (See WW2 hero cities).
-
Ukraine and the West will never accept peace with Russia as long as Russia holds territory that the West claims as well, such as Kherson, Crimea, etc. If the Russians would leave Odessa to Ukraine, under some kind of treaty, there would always be the danger that Ukraine rearms and uses Odessa and its access to the Black Sea to harm Russia. As we all know, and Russia knows even more, the West breaks ALL treaties that it signs.
-
Odessa is the last step before Russia can reunify with Transnistria. This is a problem which certainly needs to be solved. And it needs to be solved now. And it will be solved now.
In fact, you can take these arguments and flipside them, then you have the reasons, why NATO (America) has a strategic interest to take Odessa. The arguments are essentially similar to these, why the West desperately wants to have Crimea. To be straightforward. Crimea and Odessa are by far more important to the West than Kiev or any other region of Ukraine. That's why we always hear the talk about an offensive against Crimea. The question is, will the West have a strategic advantage against Russia or will Russia have a strategic advantage against NATO. The answer is obvious.
Considering all this, there is no chance in the world that Russia won't take Odessa. No matter what agreements would be proposed, or what treaties, or whatever. Maybe there was a moment where it would have been possible. In Phase 1. MAYBE still in Phase 2. But since August 2022, all this is gone. There has been too much sacrifice to not go all the way through. In fact, it would be a huge insult in the face of all people, that died on the Russian side, both civilian and military.
Nevertheless, there will be an Odessa moment. The moment, when it is clear to everyone, that Odessa can't be defended. I'll give you here an incomplete list of cases, that could be considered as an “Odessa moment”:
-
Siege of Odessa.
-
Collapse of Ukrainian armed forces.
-
Collapse of the Ukrainian state.
-
Complete destruction of the Ukrainian army.
-
Complete surrender of the Ukrainian army.
-
Cutting Odessa off, further north. E.g., Transnistria.
-
An approach to Odessa by the Russian army with no troops left to defend it from the South.
This will be the most dangerous moment in the war. It is the moment where the West will need to decide whether it will surrender Ukraine or double down and intervene with Western troops. This is essentially the question over whether WW3 will happen or not.
Whatever decision the West might take, it is insignificant for Russia, for the aforementioned reasons. Russia would take it, no matter what the escalation threat of the West would be. Even if it would mean the end of the human race. There is no scenario where Russia would not take Odessa and the world would not go up in flames. None whatsoever.
Chickens in Odessa
And here we come to the problem. I described this scenario already in one of my operational updates. See here.
The Americans have the habit to go into a place and claim it forever, only through their presence. The rationale is, that if they are there, no-one would ever dare to contest that. For example, to avoid WW3.
This is essentially true, and it works well, all over the world. See Serbia (our province, Kosovo) and East-Syria. Of course, there are many more examples. I call it the “Chicken game”.
Now, why has the 101st airborne division of the US Army been deployed to Eastern Europe? To Romania? My personal assumption is that they stay idle for the Odessa moment. If the Odessa moment happens, the US government (better, the US oligarchy) will have the opportunity, to move the 101st into Odessa.
Why would they do that? The 101st is unable to fend off a Russian attack. It potentially could buy time until the US is able to mobilize a large force in Romania to relieve them. The truth is that such a force doesn't exist and couldn't relieve anything. Nowadays, Russia has conventional deep strike abilities with hypersonic missiles that are unstoppable. The whole European rear is not defendable. The Americans are not idiots, and their military planners know this.
So why the 101st? Well, they can be quickly deployed with helicopters and create facts on the ground. In fact, create a big “chicken game” right in Odessa. This would create two problems for the Russians:
-
If now the Russians attack Odessa and the American troops, then they would have triggered WW3 from the Western perspective. This is mainly for the civilian audience worldwide to measure how a world war has started and how it could have been avoided. No one will ask why the Americans have moved in after the first missiles start flying. They might ask who shot first, but it doesn't matter. All would die anyway in nuclear fire.
-
As I pointed out already above, Odessa is a crucial and wonderful historical city for Russia. In fact, Russia doesn't want to fight in such cities, to preserve them. If the Americans would move in, Russia would be forced to destroy Odessa, to get them out of there. Again, it doesn't matter anymore at such a point.
Will this “Chicken Plan” be activated by the Americans? I really don't know. If they assume that Russia would back down if they move in, then it could happen. But such information would be wrong and the escalation would start. I personally don't believe yet, judging by the political climate, that it would be triggered. But this assessment could change anytime. For now, I don't want to issue any warnings.
Provided that such a “Chicken Plan” would be triggered by the Americans, there is still the question, which strategy the Russians would choose to get them out of there. Here are some possibilities:
-
There could be a very short timeframe for a diplomatic solution, but none that would leave Odessa in Western hands. More likely, some kind of geopolitical trade somewhere else to preserve humanity. By short, I mean no longer than 48 hours. The Russian army can't wait for American armoured brigades/divisions to marshal in Romania to feed them into Ukraine to relieve the paratroopers (101st) in Odessa.
-
A direct attack on Odessa by simply levelling it to the ground with everything inside, to not give the Americans time to catch up to their paratroopers. A painful solution.
-
Increasing the pain dial for America all over the world to force them to voluntarily withdraw. Hence, sinking the US Navy (which could be triggered anytime by Russia with her long-range hypersonic missiles), bombing all the poorly protected US bases worldwide, with a focus on manpower and equipment and the destruction of the whole NATO infrastructure in Europe with standoff weapons.
There is nothing that could be done against it, since there is currently no technology that can shoot down hypersonic missiles. This strategy is only limited by the number of available missiles. I'm not sure how many of these have been produced to date.
You see, it would be much preferable if the West simply accepts the return of a Russian city to Russia. I want to be straightforward. I don't want to see either an Odessa moment or a Russian attempt to expel the chickens.
One more remark. Scott Ritter also is referring frequently to the “Odessa moment”. I only want to highlight that we have here a similar concept, but it is not the same. As you surely have figured out on your own.
Strategic outlook
Basics
In this chapter I want to present a few strategic considerations.
Poland and its options
I think first there were considerations to intervene directly in Western Ukraine through Poland. Not to fight the Russians, but to secure territory. And I also think that President Putin made it crystal clear in one of his early speeches during the war, that such actions would trigger lightning responses. Most likely he was talking about a hypersonic rain over Poland. These intentions died down afterwards. Nevertheless, it seems that Poland is still eager to seize some parts of Ukraine that Poland considers former Polish territories.
This, of course, is an interesting fact.
Why?
Well, Russia wants to force the West to implement the new draft treaty for European security. Hence, to push back NATO influence and military infrastructure in Eastern Europe. In former articles, I presented the economic axes which could trigger a European political collapse. Here, I'm going to present some strategies on a geopolitical scale.
Poland is openly talking about taking former Polish territories. Russia is highlighting this fact in the media. Even Dimitry Medvedev often highlights it on his Telegram channel. But apart from highlighting it, there don't seem to be many objections. In fact, I believe, that it would have some advantages for Russia, if Poland would indeed take the Lvov oblast. First, see the map.
Russia could indeed allow Poland to take the Lviv oblast marked above. It is an oblast that is highly committed to and associated with Stepan Bandera ideology. They are deeply anti-Russian and one would struggle to call them Russians or former Russians. In fact, taking, appeasing, and governing it would be a burden to Russia. It will be a burden for Poland as well, but they want it. \&#D83D;\&#DE0A;
The big advantage is not about governing or appeasing it. No, the big advantage is that it would trigger major tensions within the EU and NATO, especially between Poland and the other major EU countries, Germany, France, and Italy. I remember a comment from the German chancellor Olaf Scholz in 2022. Reportedly, he privately said to the Poles that if they insist on reparation payments from Germany, that Germany could remember about former German territories that are currently part of Poland. If Poland takes Lviv, then this dispute would escalate.
Tensions in the EU and NATO absolutely contribute to the implementation of the new draft treaty for European security. Not voluntarily, but by diplomatic force. \&#D83D;\&#DE0A; So, I truly could imagine that such a move could take place if the Polish really want it, but in agreement with Russia, not against Russia's will.
Here we come to two major constraints:
-
The oblasts north of Lvov mustn't be touched by Poland. These are buffer and security zones for Belarus.
-
The oblasts to the south of Lvov also mustn't be touched by Poland. These are the geopolitical gates to the Eastern European states. So, to say, land bridges through states, that are not controlled by the West. West Ukraine (to be done), Hungary (will break free as soon as the land bridge is established) and Serbia (the same).
If Poland were to claim these territories, there would be a lightning response by President Putin. I think the message was clear to Poland.
I explained it already in my analysis of Phase 3. It is possible that West Ukraine (minus Lvov) won't join Russia. Who knows? But it certainly will be taken, demilitarized and denazified. Afterwards, it could be released in some kind of pseudo-independence, with Russian military bases on its territory, to secure this state. But this “pseudo-independent country” would be crucial because it would be Russia's gate to Eastern Europe. Its landbridge.
Black Mountain Analysis is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Hungary, Serbia and the end of NATO
And here we come straight to these landbridges and trade routes.
Before I begin, I just want to remind you about my articles “Economics and Empires 1” and “Economics and Empires 2”. Essentially, Serbia and Hungary currently are being held hostage by the West. Since they are landlocked countries that are also hostages to America, but more submissive hostages than other European nations, Serbia and Hungary can't develop independent foreign politics or foreign trade. If they don't do what they are told, many things can happen to them apart from military action:
-
Blackmailing
-
Intimidation
-
Blockade of trade routes
-
Denial of critical supplies
-
Closure of air space
And all this without openly admitting it, but by inventing reasons. The West loves to use Croatia for trade restrictions against Serbia into the European direction. Croatia then invents some reasons why Serbian lorries aren't allowed to drive through Croatia. And similar stuff.
That's the reason why Serbia has been forced these many years to say that it wants to join the EU, even though the people don't. Such fealty is required by the West, to not press Serbia down again.
And here comes the war in Ukraine and “West-Ukraine” into play. If Russia manages to secure the landbridge to Hungary in Western Ukraine, then the whole house of cards built on blackmailing Eastern Ukraine falls apart. Russia would have through Hungary, which faces problems like Serbia's even though Hungary is part of the EU and NATO, direct access to Serbia.
It would allow Serbia and Hungary to freely choose with whom they want to trade and have relations. Hence, the whole heartland would be open to these countries. And with it the SCO and BRICS states. The West couldn't threaten these countries any longer with blocking them from trade and supplies, and if military threats are employed, Russia could deploy troops or provide unlimited military assistance through the corridor.
However, I could imagine troops only in Serbia because it is a brother state. This would be a huge part of the solution for the Kosovo problem, which is a Western-occupied province of Serbia. Today, NATO can threaten Serbia with bombing in the case that Serbia is protecting its citizens in Kosovo. If Serbia would have direct land and air access to Russia, things would be completely different. Apart from that, Russia left the imperial path with the Soviet Union, which is good! Russia won't spend blood and money to maintain a remote empire anymore.
Exactly this would be the death of both the EU and NATO. Why? Look at my second map.
-
The black lines are the new main trade routes with the initial “breakaway” countries, Serbia and Hungary. They in fact are waiting for these routes to be opened. As long as they aren't open, both countries need to endure massive intimidation by the West.
-
The red lines represent potential new trade routes between Russia (BRICS/SCO) and single Eastern European countries. When these nations see how Serbia and Hungary can develop independent policy and trade, ever more European countries would join this model and break free from the Western influence/blackmailing/colonialism. As soon this begins to unravel, it would be the end of NATO and the EU. Combine this with the economic pressure, due to the self-sanctions and to Poland's possible seizure of Lvov, and NATO and the EU is finished. Of course, no one should imagine that such a centrifugal process would be finished overnight. We are talking about a few years.
You see no lines to Romania? Well, Romania is by far the most submissive colony without a single bit of an own will. I don't know how much it could free itself, even with land access to Russia.
You might want to argue that some of these countries (Croatia, Greece etc.) already have access to the sea. Yes, but they have no land access to Russia. In theory, they could do independent trade. But in case of military escalation, they would be on their own without the landbridge to Russia.
Russia's steamroller
There is something we mustn't forget. Russia is not yet mobilized in any reasonable sense. I'm not talking about full mobilization. Russia isn't even partially mobilized yet. But remember one thing: if the West would force Russia to switch its economy to a full war economy, her society also goes into full war mood and if her losses mount over a reasonable number, then the West will get what it got after Napoleon and Hitler. A Russian society, army and war machine that can't be simply “switched off” after it reconquers Ukraine. If you have a million or even two-million-man army standing on the Polish border, then this army will do what their ancestors did. They will march to Berlin or even beyond and put an end to the new threat to Russian statehood.
We haven't reached this point yet. And if there won't be an escalation which would include western troops IN Ukraine, we won't ever reach this point. Nevertheless, if the West would escalate with Western troops in Ukraine, this point could be reached easily.
As NATO is currently demilitarising itself on a large scale and soon will only exist as four letters on a piece of paper, you can imagine what will stop the Russian army on its way to Berlin. Nothing.
Is Russia powerful enough to do that? This question is totally insignificant. Remember what happens if Russia loses militarily. Given the state of NATO, there is not much they could do against such an event if Russia fights doctrinally. In Ukraine, there is a civil war between Russians. President Putin said repeatedly that he still considerers the Ukrainians as brothers and Russians. That's the reason he takes care that the civilians suffer as least as possible within such a war environment. You should not even try to think about it what weapons and strategies would be applied against a hostile nation like Poland or (fill in the blank). Certainly not a slow grinding to only destroy the enemy army.
Nor does it matter how loudly people would scream “ARTICLE 5”. This is not a magic spell, that would make the Russian army vanish. You think there would be a nuclear retaliation by the United States? Nope! Europe is a used condom for the Americans. The new cool guys are in Asia. America will never ever put itself at risk for a used condom. Pardon, for Europe.
Again, I don't see such a scenario happening. But nothing is certain.
Now we are coming closer to my conclusion.
China
Initially I said that there will be a WW3. And yes, I think there will be a WW3. But I doubt, at least for now, that it will be triggered in Europe. And I also doubt that its main battlefield will be in Europe. Although there will be a battle in Europe.
The big battle of our time will be in Asia and in the pacific. And not today but in 2030. The battle will be about throwing the United States out of a region where it doesn't belong. China is preparing two strategies.
-
The best-case scenario for the world would be if BRICS and the SCO bring the American imperial economy down, in such a way, that it couldn't sustain its empire and network of military bases any longer. Thereby it would withdraw under an economic and social collapse from its bases abroad. Don't get me wrong. I do not wish the American people their downfall. Absolutely not! I like Americans (the people, not the imperial parasite) as much as I do anyone else. I wish for the American people, that your country comes out stronger through the hard times that are ahead. That you manage to become a normal nation among others and that every single American becomes prosperous. This with normal trade relations with other nations, without the need to bomb them to get good trade conditions.
-
Option two is war. Therefore, China is currently building the biggest military the world has ever seen. But it is not ready yet in terms of quantity or professionalism/experience. But it certainly will be, within the next few years, 2030 at the latest. Russia, currently pinning down the empire in Europe and depleting it, is the biggest gift China can get. That's why China will do what it can to sustain this status. Therefore, China is helping Russia to circumvent most of the sanctions.
And Russia is more than returning the favour. She is buying time for China with her blood as a side effect of her existential struggle against NATO.
Well, I will stop here, since I'm planning to write a separate article about the struggle in the Pacific region. But please keep the following in mind. I can make more or less accurate predictions for the timeframe of one year (operational). I can explain the shape, probabilities and boundaries of a strategy, which covers up to three years. The actual implementation could look completely different. And everything one writes, including myself, that would make predictions for a time after three years (vision), simply writes fairy tales.
Nevertheless, I'll try to write such a fairy tale about the Pacific region in another article. But I'll mark it as an assumption and also as one possible scenario between infinite possible scenarios. Hence, you'll need to consider it to learn backgrounds but apart from that you should take it with a grain of salt.
Conclusion
Okay, we reached the end of the article. I'll try to sum it up and make a conclusion.
The question that this article seeks to answer is about the prospect of a World War developing from the Ukraine crisis. I see a probability of 90% that the Ukraine war will not evolve into a World War. Unfortunately, 90% is still far from certain! There is still a possibility that the West will try to push proxy forces (Poland, Romania, Germany?) into Ukraine to create a bigger “local”/continental conflict, while the Americans focus on Asia. Here we are at 5%. And above that, there is a probability of 5% that the United States will directly intervene (See Odessa moment, etc.), which certainly would evolve into an instant World War.
-
Peace after Ukrainian army is defeated (90%)
-
Developing war between Russia and European proxies within Ukraine/Europe (5%)
-
American intervention &emdassh; World War 3 (5%).
That is, of course, still too high. We are talking about the human race.
Indeed, there are two major determining factors which will decide whether there will be an escalation or not:
The “Odessa moment” and the “Western Ukraine” moment.
-
Odessa moment:
The West will try to do what it can to avoid giving Odessa to the Russians. This is for strategic military considerations. If the Russians have it, they will have a strategic advantage and leverage over NATO. If NATO has it, the same applies to NATO against Russia.
-
“Western Ukraine” moment:
Here we are talking about Russia's land access to Hungary and thereby to Serbia. Essentially, if Russia gets it, NATO and the EU is done. History. Not instantly, but within a reasonable number of years.
I can only leave you here and say that when one of these moments are imminent, start praying to whomever you are praying to.
Nevertheless, I want to end this article on a positive note. Since I AM positive. Everything depends on the decisions of the oligarchs in the United States. Are they willing to let Ukraine go or not when they are threatened with global annihilation? These guys are not idiots. Sure, they want to possess power over others, but in the event of a nuclear war, they and their children will possess nothing. Exactly as everyone else.
Even though they seem to have no reverse gear and always doubling down, in this particular case I assume that they would do the right thing and vacate Ukraine. Why is there still a possibility of 10% of escalation? Well, Russia (BRICS) is engaged in escalation management, to provide a safe way for the Americans to transition into a normal state.
And here we come to the fact that not even the Americans and their oligarchs can control everything. It is possible that a crazy group of people, either within America or within Europe, could suddenly do something extremely stupid when they feel that the end is near. Think of Poles or the Baltic statelets or some extremely crazy American neoconservatives. The good thing is that I don't give more than a 10% chance to such an idiotic chain of events.