Monthly Shaarli
December, 2021

What follows is a long essay I wrote almost a year ago, in October 2020, on another platform. I had almost no audience at the time, but many people told me they enjoyed it, and I am happy to provide this edited, shortened and slightly updated version for many new readers.
In reading it now, I find that it is more heavily focused on lockdowns and mass containment than it would be if I wrote it today, but I think even these passages are still important. Lockdowns will be kept around, initially as selective “lock-outs” to repress and punish the unvaccinated; from there it will be trivial to impose closures on whole populations once again, as case statistics deteriorate in the winter.
Beyond all of the politics and hysteria and right-thinking, there is a real virus beneath it all. Its name is Sars-Cov-2. This virus is not to be confused with Covid-19, which is the illness that the virus causes. The distinction, like that between HIV and AIDS, is medically useful, and it invites us to make other, analogous distinctions, in service of cleaning up our thought.
Illness is as much a social matter as a biological one, and for most of us, the vastly more significant distinction is not that between virus and disease, but between the biological reality of the virus-disease, and the political and social perceptions of this virus-disease. Words help us think, and so here I propose to call the former biological virus-disease Sars2; and the latter, socio-political virus-disease, Covid.
Sars2 is only one of the players responsible for the social construction of Covid, and not even the most important one. It is best to think of Covid as a committee project, with a lot of creative talent. Politicians, epidemiologists, virologists, public health experts, computer models, public health institutes, journalists, Chinese bureaucrats, and yes, among them all, Sars2—they all get some say in constructing Covid. Sometimes Sars2 disagrees with their construct, and sometimes his fellow committee members listen to him. But sometimes he disagrees and gets overruled. He’s only one voice at the table, after all. When a Twitter blue-check or a scientist or your professor lectures you about the substance of scientific consensus, they are just delivering articles of faith about the social construct of Covid, as the committee has defined it.
When we say that something is a social construct, we don’t mean that it isn’t real. We just mean that it could be conceived of in a much different way; and that a big part of what we take for granted about the constructed thing is malleable. Clearly political and scientific authorities could have constructed a massively different version of Covid if they wanted to. If you doubt this, look at China. They have basically eradicated Covid by constructing it out of existence.
In the West, Covid has acquired a variety of features that demand constant and heavy-handed technocratic intervention. This is not the case everywhere, but in the West, where technocratic bureaucracies dominate, this is what Covid has become. The technocrats have had a huge hand in building Covid, and they have constructed the perfect nail for their hammer.
Above all, they have constructed Covid to be an intractable problem, because our bureaucracies derive much of their authority and legitimacy from permanent, intractable problems. This was not the only path. We very nearly embarked upon a quite different one. Before the permanent bureaucracy recognised that Sars2 provided fodder for another eternal project, they had taken substantial steps towards building a very different disease out of Sars2—a disease that nobody needed to worry about very much, that was not very different from other respiratory illnesses, and that would probably go away in the end, or that we could at least overlook if we didn’t think about it too carefully or test for it all that widely.
That changed very quickly. By March, western Covid committees had begun building a very different disease. One of its most important features, is its omnipresence and invisibility.
Covid Is A Hidden, Lurking Menace
Central to our image of Covid is its appearance out of nowhere. A wet market deep in China, or some bio-lab—official discourse is agnostic. The earliest images to reach the West depicted apparently healthy Chinese people suddenly collapsing in convulsions, as if struck by God. Efforts to quarantine the earliest Covid patients in Europe totally failed, as the disease turned out to be circulating broadly among the population first in Lombardy, then in northern Europe, and finally in the United States. This early impression of Covid as omnipresent and invisible remains with us to this day. It is not enough to stay home if you are sick. Healthy people, who never develop symptoms of Covid, nevertheless spread the disease. Aerosolised transmission is the subject of much discussion; Covid menaces through the air. Interestingly, the aerosol aspect only took off after establishment scientists decided that transmission via surfaces was at best infrequent. Yet the menace of contaminated surfaces has persisted in our consciousness, alongside the contaminated air, and the contaminated healthy people, and the visibly contaminated sick.
In the ancient world, it was held that certain life-forms, such as fish, were generated spontaneously by the environment. If you kept a barrel of water around long enough, theory held you’d soon find little minnows swimming around in it. This is, functionally, how we behave with Covid. Two healthy people conversing in an unventilated room will probably yield Covid in one of them. In fact Covid can arise from any instance of social proximity. People fear objects that many others have touched. People fear friends or relatives who are perceived to socialise or travel too much.
Now, Covid does not lurk absolutely everywhere. It favours above all those spaces subject to the direct control of government bureaucracies. Schools, therefore, are especially feared. Public transit is considered another terrifying locus of infection. Covid is especially pervasive in hospitals; a lot of people avoid them now at all costs. In the first wave, it was common to close parks and playgrounds, even though we know the risk of transmission outdoors is minimal. Bureaucrats control public parks.
As you move away from bureaucratic oversight, the threat of Covid recedes. Bars and clubs, in most countries subject to substantial regulation but essentially private enterprises, are a kind of middle ground: Dangerous certainly, and the subject of much moral expostulation, but not quite the unmitigated danger of schools. Things like restaurants and chamber music concerts at private venues take a further step away from bureaucratic oversight, and Covid recedes accordingly. Private offices are managed by bureaucrats hardly at all, so we don't read that much about infection at work. The exception is government bureaucrats themselves, who hear a lot about how dangerous it is for them to go to the office. That space furthest removed from bureaucratic supervision, the home, is a safe haven from Covid, although it is the one place you’re most likely to contract Sars2.
The presence of Covid, which is invisible and potentially everywhere, can only be ascertained via special tests. While you can give yourself an antigen test at home, the results are far less authoritative than antigen tests administered by authorised agents of the bureaucracy, and these in turn are still less significant than PCR tests, administered by medical professions and processed in a lab.
Mere symptoms do not mean you are infected; you could have something else. On the other hand, perfect health does not mean you are Covid-free. I don’t think enough people have recognised how bizarre this situation is. Consider all those people these past months who have recovered from a respiratory illness, with fever and cough, without ever being tested. When they suggest that perhaps they had Covid, it is routine to doubt them. Certainly nobody would exempt them from vaccines on that basis. Compare them to all the people who have no symptoms at all, but test positive, and are widely considered to have a disease. The voluminous and eager literature on the asymptomatics is extremely telling. They are 20% of all cases, or 80%; they are responsible for 2% of infections, or 40%. They are tallied in the statistics, undifferentiated from the truly ill.
Central to the definition of Covid, is that mass testing programs be the only means of defining the extent of the disease, assessing the success of the technocratic response, and the virtue of the compliant population. Covid is not like other communicable diseases, which are diagnosed mostly in private, according to likely symptoms.
Covid as a hidden, lurking menace has had by far the worst consequences for children. Sars2, everybody knows, is not a danger to them. The virus himself has been very clear about this and it has not been possible for the disease bureaucrats to overrule him. It is easy to imagine a parallel universe, one where we are relieved at the near-total safety of our children in the face of this disease, one where we spare them the effects of public health interventions, because they are not at risk.
That is not our world. Government bureaucracies are heavily involved in the lives of children, particularly through schools. Thus public health authorities and, most unnaturally, many women, have come to fear children as a vector of infection. Some people even believe children are the main drivers of the pandemic. Covid lurks, a deadly silent threat, inside them, wherever they gather to play, wherever they gather in school. Classrooms and childcare centres have become places of intense microbial hysteria, silly simulacra of hospitals, with odd Plexiglas barriers, hand sanitiser around every corner, and constant, constant testing. In this world Covid creates its own reality vortex. You find infections where you swab the most. Every time schools are opened, intense surveillance uncovers a new flood of cases, which cements the image of children as dangerous and contaminated, a mortal threat to their grandparents.
If you say to a person of orthodox political alignments that this is a bizarre approach to any disease, to surround precisely those people at least risk with so many precautions, harmful in themselves; and at the same time to leave those most at-risk to their own devices with vague advice to self-isolate, they will say a great many things to you. One of the first things they say will be this: Covid is a totally new virus. It poses an unknown and wholly unprecedented threat to our society. There are no low-risk populations, and there is no way way to protect the vulnerable from this pervasive invisible pathogen. All we can do is disrupt hidden transmission among the invulnerable carriers.
Covid Is A Novel, Extra-Natural Disease
As with the hidden menace, the foundations for this aspect of Covid were laid early on. In the beginning Covid was held to be a zoonotic virus, brought upon humans by exotic Chinese dietary practices. Now many admit that it is likely a laboratory invention, unleashed with some sinister purpose or by accident. However that may be, Covid is totally new to humans; it is unlike any disease we have ever faced before. It is beyond nature and we have no natural defences against it. In the discourse surrounding Covid there has always been the tendency to push this extra-natural facet to the extremes, nearly to the supernatural. The early paranoia about surfaces comes to mind yet again, with those old stories of mail-room employees picking up Covid from packages sent from far-off, plague-ridden lands. Covid can perfuse the air for hours after a fateful cough. There is no general unified Covid with a limited set of properties. Attempts to fix its characteristics dissolve in a pool of contradictory evidence. Note the widely differing characteristics of Covid in neighbouring, broadly similar countries. The better part of this variation arises from different national medical bureaucracies, which have lent Covid different properties according to their capacities and proclivities. But of course the variation is not understood in that way; it is rather put down to some magical aspect of the virus itself. Extranatural virions do one thing in Sweden, and another thing in Germany, and another thing in Italy.
Because Covid is an extra-natural disease, our natural immune systems are not up to fighting it. This is why the prospect of Covid reinfection has been a matter of obsession from the very beginning. The first rumours of reinfection arose in China, where reinfected were said to suffer devastating symptoms, such as heart attacks. Similar cases were never observed in the West and so everyone stopped talking about that. Later on, South Korean health officials began reporting various cases of reinfection, but then it emerged that this was an artefact of the manic Korean testing regime. Recovering Covid patients issued multiple tests may come up negative one day and positive the next, as their body sheds the virus. Though they had been proven wrong twice, reinfection theories persisted. Minor victory came when some serological studies failed to find antibodies in some confirmed Covid patients. Later they had the holy grail, namely several confirmed genuine reinfections.
You could say, perhaps, that the reinfectionists on the Covid committee forced a compromise with Sars2 on this point. Reinfection aligns neatly with established doctrine about the inadequacy of our natural defences. Only broad-scale social and political countermeasures have any chance of success against Covid. Think of it as a substitute, artificial, social immune system: Lockdowns, curfews, quarantines, travel bans, mass testing, masks, school closures, personal distance, interior ventilation, hand sanitiser, contact tracing apps, home office, and more. This is what a society of immune-compromised people looks like. Just as our bodily immune response is responsible for many of the symptoms we associate with illness, so too is the social immune response responsible for the majority of negative effects from Covid. We have made our whole society sick, in a vain effort to keep some people healthy.
The body’s immune system can overreact to the point that it poses a greater danger than the infection itself. In a related way, our social response to Sars2 has entered an inflammatory phase, a spiral of disease hysteria demanding mass testing and contact tracing leading to the discovery of more cases causing more stringent anti-Covid social measures that just make our nations and our societies vastly sicker and more dysfunctional than we were before. Remember that this all started with "two weeks to crush the curve," and consider how far we have come, and how far we might go still. It goes without saying that all these negative effects are taken as further proof of the unusual threat that Covid poses.
Beyond the extra-natural social defences, we have placed all of our hopes in an extra-natural vaccine. Here the discourse devolves into awkward contradiction. To begin with, vaccines, while indeed extra-natural, merely stimulate natural immunity. If we may hope for a vaccine, it is unclear why we cannot let some of our natural immune systems join the fight. What is more, despite unprecedented mass testing programs and enormous scientific interest and the bias of our perspective, Covid reinfection is not yet a pervasive phenomenon. Those with natural immunity are well protected indeed. From the very beginning, the developers of extra-natural vaccines have been warning for a long time that their products will provide only partial protection against Sars2. Yet their products were marketed, until recently, as more protective than infection, and to this moment, even as the vaccines fail, politicians everywhere insist that mass vaccination is the only answer.
Fundamental to this paradox, is the axiom that extra-natural Covid poses an unknowable yet grave risk to everyone. Reinfection is only the beginning of it. All those people who have recovered without lingering effects may well develop brain lesions next year. The health of their internal organs has yet to be confirmed and there are dark suppositions that no few harbour hidden heart or liver or kidney damage. A lot of people might never smell again. Many recover only to relapse several weeks later, and perhaps again several weeks after that. There is now an enormous body of literature about Long Covid, a chronic syndrome marked by every symptom you could imagine: Ongoing fatigue, shortness of breath, brain fog, joint pain, cartilage degeneration, insomnia, depression—on and on.
Before you get into the weeds of the journal literature on Long Covid or permanent organ damage from Sars2, consider this: Officially, the virus has infected over 220 million people across the world. That is a great river, wide and deep, for our Covid committee to trawl for stories of unusual complications, debilitating symptoms and incomplete convalescences, from now until forever. The question is not, what odd horrible things lurk in that river; but how many of them there are, relative to the ordinary pedestrian things. What are you most likely to find? Long Covid and relapsed Covid and heart attack Covid? Or low-grade grade fever Covid, mild-cough Covid, over-in-five-days-without-a-second-thought Covid? I think we can all answer that question for ourselves. That we let the rare and the unusual dominate our construction of Covid, rather than the mild and the pedestrian, is partly down to publication bias. The banal almost never makes it into print; the strange and unusual invariably find an audience.
But that is not the only reason we must constantly hear about the grave unknown risks of this extra-natural disease. There are others too, and the biggest is simply this: The bureaucracies responsible for constructing Covid have decided that infections must be minimised above all else. That is the Sisyphean task they have set themselves. As the costs of their containment measures increase and society gets sicker, they must tell ever grimmer stories about why it is unacceptable for anyone, ever, to contract Sars2.
Covid Is Universal
Covid is the great sin of globalism, and globalism has brought it everywhere. Not even Antarctica remains Covid-free. Covid can infect animals as well as humans, and the prospect of reinfection has been leveraged to dispel the idea that anyone might become immune from Covid. In this way, the disease applies always and everywhere to everyone. (The opposite and far better-documented phenomenon, that a lot of people who have never had Sars2 have some partial immunity—presumably from prior non-Sars2 coronavirus infections—is contrary to Universal Covid and so it is excluded from official Covid doctrine.)
Because Covid is everywhere, and everybody is subject to it, containment policies must also be general, and vaccination policies must be too. For the disease bureaucrats, Universal Covid is a central doctrine, eagerly defended. The myth of Universal Covid is reinforced by the infection statistics we hear about every day. The only thing that ever makes headlines is how many positive tests there were today, as opposed to yesterday or last week; and which regions have the most infections right now. Since the Lombardy outbreak, everybody grasps that Sars2 infections have a regional particularism about them, but this is never presented as a challenge to Covid’s universality. Regional “hot-spots” are universally applicable examples of what will happen to your region, too, if Covid is not suppressed there and everywhere. Positive swabs might also be broken down into age cohorts, and these function much the same way. If your region has many new cases, but nobody really seems to be sick or dying, this is because the pandemic is currently concentrated among young people. Old people are next, if everybody does not comply with suppression measures. The effect is to make grim statistics a problem, even in the total absence of anybody actually suffering or dying.
Beyond these crude numbers, you don’t know anything about all those positive tests or the processes that generated them at all. It is very hard to figure out, for example, how many of them represent people who tested positive last week, and now have submitted a second test to see if they’ve cleared the virus and can leave their apartment again. Crucial for the interpretation of any such statistics, is to know how many of them emerge from contact-tracing operations, from the kinds of routine tests administered to people like doctors, teachers, and school children; and how many of them reflect actual patients seeking medical treatment. Equally central, if you want to make sense of these numbers, is how many of these people are actually sick, which is another question that many testing regimes leave wholly or mostly unanswered.
Western nations instituted mass testing programs, a universal solution to Universal Covid, after the example of South Korea. In the early days, it was thought that the Koreans had avoided a serious outbreak, without locking down, by testing and tracing everybody. So now we’re doing that too. The theory was that the technocrats would find the positives, shut them away, and allow the rest of us to go about our lives. In practice, it has been pretty much the opposite. Mass testing and tracing, far from replacing mass containment, merely provide the data to justify its enforcement. It is the same with vaccines, now that many regimes are struggling to vaccinate their way out of lockdowns. All that testing and tracing ought to make vaccines less important. Are they not identifying and quarantining the sick? Alas, you can never test and trace your way out of the Universal Covid we have constructed. That would only work for a Local Covid or an Endemic Covid, which we have not built—a Covid that afflicts certain people and not others. So the contact tracers do their thing, but the statistics that their activities generate are used to assess the state of the Covid outbreak for absolutely everybody and general, universal solutions are deployed in response to them. More lockdowns, more vaccines.
The German government is highly federalised, even more so than the United States. Much of the governing actually happens at the level of individual federal states, or Bundesländer. Each of the states could, in theory, manage its own response, according to local circumstances and sensibilities. You’d think this would be an advantage, because the instance of Sars2 infections varies vastly across Germany, and people in different states have different opinions about how to deal with it. If different states had gone their different ways, we would now have very direct insight into the effectiveness of competing containment policies. Of course, nobody in government sees it that way. Instead, Angela Merkel has spent every minute fighting against a federal approach and demanding a unified response. Newspapers have deplored our traditional federalism.
A final expression of Universal Covid lies in the universal mathematical formulae that were once widely held to predict its future progress. In March 2020, the population of the entire world received instruction in the basics of exponential functions. It was thought, as the first wave advanced, that Covid could be plotted on a graph, with time as the x axis and new cases as the y axis. Wherever Covid was spreading, this exercise yielded a curve sloping upwards to the right. Predicting the future course of Covid became a simple matter of plotting that same exponential function into future x-axis time. A lot of commentators, including many scientists, portrayed the resulting projections as mathematical certainties. This was important because raw infection numbers differed everywhere: Lombardy had the worst statistics, and so it was in the lead. Behind it were France and Spain, where Lombardy had been the previous week. Further back was Germany, which needed still three or four more weeks to reach a catastrophe of Lombardic scale. But the math assured all of us that the same thing would happen everywhere, eventually. I will confess that I found all of this powerfully convincing at the time. The flat edifice of Universal Covid seemed to brook no contradictions. But typing it all out now, it is easy to see how foolish it was. Covid did not work the same everywhere, and the curves themselves were never forever and always exponential. Germany never caught up to Lombardy. It never even came close.
Those graphs have receded from our conceptions of Covid. That is not only because they were wrong, but because they ended up drawing attention to how much all of the national outbreaks differed from each other. They were a direct shot across the bow of Universal Covid, and in April and May you could read very long essays by deeply mystified people, pondering how this was possible and what was going on. Many of the authors behind these think pieces were presumably familiar with things like seasonal flu epidemics, which in Europe often differ drastically across regions, even though a similar mixture of flu viruses are typically implicated every season. Influenza, however, isn’t constructed to be a universal affliction, so its various impacts have never bothered anybody.
Covid is a Vice of the Young and the Healthy Against the Old and the Sick
We come to the fourth obtrusive feature of our socially-constructed Covid. By nautical miles, it is the most egregious and appalling one of all, and so I regret that I have the least to say about it. Stupid cruelty does not admit of much analysis.
Sars2 is no threat to the young, we said that already. What is more, disease bureaucracies have not been able to convince the young that they, personally, should worry about Sars2. The only way to enforce the one-size-fits-all measures that Universal Covid demands, is via an ugly moral blackmail.
What began as an appeal in early days to the conscience of the youth, to consider the health of their grandparents, has become an all-out war on everything that young, healthy and fit people do. Here is insight into the withered souls of many scientists and bureaucrats, who see in the casual joy, effortless strength and unthinking beauty of our youth a great indictment of themselves. Many of them have long disliked young people and what they get up to, and now they have been given the power to vent their spleens about it.
The social life of young people irks them most of all. Parties are scorned. Contact tracers routinely identify private celebrations as outbreak epicentres, and from the press reports, you’d think whole districts are rising up in rage against the kids who dared to gather in somebody’s friend’s garage. German police spent a lot of time the past few springs citing teenagers who, after weeks of isolation, dared to get a few beers with friends in the park. It was truly strange to behold: Patrol cars sporting loudspeakers driving slowly along footpaths, between the trees, past benches, reciting the corona distancing rules.
It’s safe to complain about parties, because some people stupidly assume they aren’t essential, or that they’re irresponsible or excessive. But behind the scenes, these ageing meddlers were busy attacking everything else. They have closed gyms for months. When they allowed them to reopen, the conditions were so onerous and counterproductive that it was hard to doubt malicious intent. A whole cloud of official opprobrium descended upon every sort of recreational travel, and remains there. Early disease clusters were traced to skiers, and a batch of young people who’d had the misfortune to visit Ischgl at the wrong time were handed responsibility for several national outbreaks. (Chinese travellers, responsible for the entire European pandemic, remained beyond criticism, even as Italy and Germany had a brief spat over who introduced the virus to whom.) In Bavaria, open-air playgrounds were closed for weeks and weeks, longer than hair salons, in case you thought any of this was about the risk of infection.
When anonymous bureaucrats of this sort are given their way, secure in the knowledge that nobody will hold them accountable for their egregious decisions, and that every mild critique of their policies will be suppressed, they spiral into extremism. In the midst of the lockdown, they began to complain that people were shopping for groceries too frequently and spending too much time in supermarkets. After mask requirements were issued for public transit and indoor spaces, newspapers ran very strange articles lecturing their readers about proper mask procedures. Readers were told never to put on a mask until they’d thoroughly washed and sanitised their hands. Then they were told never to touch the mask again at all. Should they touch it the mask would become hopelessly contaminated, and their hands too, so they'd need to sterilise them all over again and start over with a new mask. Runners and walkers were still allowed outside, for purposes of exercise, and this made the disease bureaucrats very nervous indeed. Pundits complained that parks were too full. Schoolmarms posing as experts began telling runners that their heavy breathing was a danger to everyone within three or four metres of them.
Covid the socially constructed virus-disease exploits the health and beauty of youth to reach the old, but this is not how Sars2 actually works. Sars2 prefers to do most of its killing in institutional settings. It is at base a disease of healthcare institutions, like MERS and SARS; it thrives in nursing homes and in hospital wings. This in Spring 2020 it was ironically the most alarmist regions, those that had imposed the strictest lockdowns nominally for the safety of the elderly, which ended up killing more elderly than anybody else, due to over-hospitalisation, criminal mistreatment of many Sars2 patients and poor, paranoid management of elderly cases.
Undeniably, Sars2—like many other viruses—exploits the social activity of humans. Until now, the Covid bureaucrats have responded with rolling seasonal embargoes on all human social activity that is not mediated by electronics. People who violate these restrictions are behaving irresponsibly and endangering all of society. Consider how much this stance differs from their approach to other viruses. Were gay men, at any point, ever exhorted to abstain from anal sex in the interests of defeating HIV? Was the gay community ever blamed for the AIDS epidemic and scolded by public health bureaucrats for worsening statistics? Were gay bars and bath houses ever targeted for closure or curfews or—imagine!—contact tracing, to flatten the curve? No, they weren’t; and if any of that had happened, we’d be reading to this day what a grave injustice all of it was. HIV is undeniably much harder on those it infects than Sars2, and I submit that, in the hierarchy of human needs, quotidian social interaction ranks well above anal sex.
Some Deconstruction
The question of how we ended up with this miserable social construction of Covid, and not with some other more manageable social construction of Covid, is well worth pondering. The most obvious answer is simply this: Our disease bureaucrats, a bunch of socially promoted charlatans and degree connoisseurs who play scientists on television, got spooked by Sars2. They had a lot of credentials but no real ideas, and so they borrowed their public health response from China.
Before January 2020, lockdowns were totally foreign to the public health establishment. None of our governments or epidemiologists or disease-control agencies had ever before contemplated containing a pandemic by placing everybody under house arrest and freezing the better part of economic and social life. Lockdowns as a measure against Covid are, top to bottom, an invention not of a fabled “scientific consensus,” but of anonymous authoritarian Chinese bureaucrats whose motives and intent are largely opaque to us. Italian disease bureaucrats copied this measure from the Chinese bureaucrats, the rest of our disease bureaucrats copied from the Italians, and since then they have all continued the senseless copying of containment policies among themselves down to this very moment. If you are an incompetent pseudo-intellectual devoid of ideas, following others is your only option; and if you can get everyone else to follow in the same way, you might even escape blame.
Covid, the socially constructed virus-disease, was fashioned in the midst of the lockdowns, to justify them. This scary construct also works well as a justification for coercive, universal vaccination programs, and so it continues to be propagated. It is a monument to the cognitive dissonance of our intelligentsia, who lobbied hard for a catastrophic policy on the strength of dire predictions that, save in a few much publicised cases, were never realised. Almost everything that has become “scientific consensus” about Covid is a retroactive justification of our failed and plainly foolish containment measures: Covid lurks everywhere, and it is invisible, so we must hide from it in our homes. Covid is a totally novel disease, full of indeterminate properties and unknowable risks, so nobody can be exposed. Covid endangers everyone, and so everyone must stay inside. Even if young people are all but invulnerable to Covid, they too must lock down, to save the old. And of course, for all of these reasons, absolutely everyone must be vaccinated—however dangerous the vaccines, however low-risk the person.
That is the simplest, most straightforward answer to the question of how we got this Covid, and not some other Covid. It is equivalent to the wet-market theory of the origins of Sars2. We got Covid from the stupidity and incompetence of our elites, desperate to justify the economic destruction they wrought via their plagiarised containment measures. Relatedly, in the wet-market theory of Sars2, the virus found its way to humans via the unhygienic dietary practices of the Chinese, and was spread everywhere by the unrelenting globalism of our short-sighted elites.
But just as the vastly more plausible theory of Sars2 is that it represents the product of gain of function research at the Wuhan Institute of Virology, so too there is another, much more compelling way of thinking about the deepest origins of our Covid construct. Cast your mind back to January, as the Chinese implemented their own lockdown of Hubei. Consider those bizarre videos that appeared on social media, showing Covid patients convulsing in streets, collapsing on stairs—succumbing, or so it seemed, to instant viral death. Some of this footage recalled scenes from Hollywood films, particularly Contagion. At the time, the framing was this: The Chinese were keeping a tight lid on the Wuhan outbreak, but here and there the magic of social media could defeat the evil communist censors and provide some glimpse of what was really going on. Clips of Chinese news coverage circulated, where the screen briefly flashed mortality figures orders of magnitude higher than the official numbers. This was the journalists trying to alert the rest of the world, or it was grim reality crying out from the ground, or something. All kinds of strange news items, about mass mobile account cancellations in China and industrial-scale cremation in Wuhan, were put about to show that the Chinese were dying in the millions. Everyone in the world watched blurry video of some Chinese guys welding a door shut. Online news outfits declared that the Chinese were literally sealing people in their apartments. That’s how bad Covid was. In the weeks before conditions deteriorated in Lombardy, a whole host of social media accounts began advocating lockdowns as a western containment measure. It has now emerged that many of these were operated by people in China.
Sophisticated propaganda and disinformation campaigns involve more than Russians buying Facebook ads. One tactic, is to take the idea you want to plant, cut it up into a bunch of different pieces, and release these to the world via various proxies and intermediaries. These little bits and piece might take the form of accidental leaks or hacked data or surreptitious photos or whatever. People gather these pieces and put them together, find that they all contribute to the same, ominous picture, and believe that they have discovered a hidden truth. This gives the lie an organic, authentic feel. It becomes a personal thesis and nobody realises that they have been led down the garden path. All of that early nonsense from China has entirely this feel about it. None of it was true, nobody really knows where it came from, but it all supported the same false hysteria.
So a deeper, more conspiratorial but also more plausible answer to the origins of our socially constructed disease, might be this: Covid is the ideological construct our disease bureaucrats used to justify their failed lockdowns; but at root, this construct was probably not of their making. They merely recycled the selfsame propaganda by which shadowy actors had sold them on lockdowns in the first place. It looks like some people very much wanted western governments to implement lockdowns. This led to a remarkable realignment of opinion, whereby the elite leftist establishment, which had sought to minimise the virus as much as possible, totally reversed their position by early March 2020 and began advocating a maximal approach. The Covid that we have now is all downstream from that, and there is no changing it.
*
How things started, of course, is no indication of how they will end. The optimistic scenario was that the vaccine roll-out in Spring 2021 would defeat Sars2 and that all of this would go away. That was never very plausible, and as it now becomes clear to everyone that the vaccines do not work very well, optimism is no longer on the menu. Perhaps it never was. Covid has given a lot of terrible, petty, mediocre people a great deal of power, and they won’t be willing to give that up, ever, however often they fail.
The most likely scenario, the one which is already playing out, is that Covid devolves into an eternal nuisance after the pattern of climate change, but more intrusive. The vaccines have come, but mass testing and various containment policies remain in place. There will be some attempt to maintain regular boosters, first for the elderly, then for everyone. But this path is one of diminishing returns. Each new round of injections will inspire less compliance, and will also prove less effective.
Over the next several years, most countries will probably fight their disease bureaucrats towards some minimally acceptable long-term compromise. Home office will be normalised. The media hysteria will never totally fade. Full lockdowns, contrary to the interests of many industries, will probably be phased out in the coming years, but in the meantime we will see increasingly inhumane restrictions on the unvaccinated. Other obnoxious interventions will likely return every year in time for Christmas, a holiday that will be increasingly celebrated with a few close relatives, in private. The campaigns against shaking hands, standing too close, or having too many people over for dinner will probably not end for a long time. Contact tracers will come to be loathed as much as city parking enforcers. In the longer run, Covid policy will probably be redirected towards pharmaceutical boondoggles and hygiene legislation that creates markets for a new world of garbage consumer products. The vaccines are probably an early preview of all of the false hope, graft and absurdity the coming world of market solutions will bring. Should Sars2 become especially rare, then other seasonal respiratory illnesses, like the flu, will likely be pressed into service. In many countries, it is likely that a whole generation of kids will grow up wearing crayola-branded dinosaur masks in school.
Still more pessimistic scenarios are possible, but they would probably resolve themselves sooner or later. It is hard to see how any western democracy could endure the economic destruction of biannual lockdowns, or other similarly drastic interventions, for many more years, without destabilising itself politically.
Campaigns to impose regular boosters on entire populations will stir up more and more opposition to mandatory vaccination regimes and, if the gods are merciful, make repression of the unvaccinated increasingly unworkable. We must also remember that the disease bureaucrats are not omnipotent. They have seized power, at first on temporary terms, from other political players, who will sooner or later try to get it back. Intemperate Covid policies have also inspired a wide array of opposition throughout academia and government, even if you don’t always see it. Now that the vaccines have failed and there is no obvious end, it is likely these people will begin to form opposition movements from within bureaucratic ranks. In some countries they might even win, and in the breakdown of international consensus there will be some small hope.

The release a couple of days ago on the RF Ministry of Foreign Affairs website of its draft treaties to totally revise the European security architecture¹ has been picked up by our leading mainstream media. The New York Times lost no time posting an article by its most experienced journalists covering Russia, Andrew Kramer and Steven Erlanger: “Russia Lays Out Demands for a Sweeping New Security Deal With NATO.” For its part, The Financial Times brought together its key experts Max Seddon in Moscow, Henry Foy in Brussels and Aime Williams in Washington to concoct “Russia publishes ‘red line’ security demands for Nato and US.”
Both flagships of the English language print media correctly identified the main new feature of the Russian initiative, encapsulated by the word ‘demands.” However, they did not explore the “what if” question, how and why these ‘demands’ are being presented de facto if not by name as an ‘ultimatum,’ as I consider them to be.
The newspaper articles themselves are weak tea. They summarize the points set out in the Russian draft treaties. But they are incapable of providing an interpretation of what the Russian initiative means for the immediate future of us all.
Normally they would be hand fed such analysis by the U.S. State Department and Pentagon. However, this time Washington has declined to comment, saying it is now studying the Russian treaties and will have its answer in a week or so. In the meantime, America’s reliable lap dog Jens Stoltenberg, NATO Secretary General, saw no need for reflection and flatly rejected the Russian demands as unacceptable. The ‘front line’ NATO member states in the Baltics also reflexively vetoed any talks with the Russians on these matters.
However, even the FT and NYT understand what Mr. Stoltenberg’s opinion or Estonia’s opinion is worth and held back on giving their own thumbs up or down. They both analyze the draft treaties primarily in connection with the current massing of Russian troops at the border of Ukraine. They assume that if the Russians receive no satisfaction on their demands they will use this to justify an invasion. We are told that in such an eventuality a new Cold War will set in on the Old Continent, as if that will be the end of all the fuss.
In part, the problem with these media is that their journalist and editorial teams are tone deaf as regards things Russian. They are insensitive to nuance and incapable of seeing what is new here in content and still more in the presentation of the Russian texts. In part, the weakness is attributable to the common problem of journalists: their time horizon goes back to what happened last week. They lack perspective.
In what I present below, I will attempt to address these shortcomings. I will not invoke historical time, which would possibly take us back seventy years to the start of the first Cold War or even thirty years to the end of that Cold War, but will restrict my commentary to the time surrounding the last such Russian call for treaties to regulate the security environment on the European continent, 2008 – 2009 under then President Dmitry Medvedev. That is within the time horizon of political science.
I will pay particular attention to the tone of this Russian démarche and will try to explain why the Russians have drawn their ‘red lines’ in the sand precisely now. All of this will lead to a conclusion that it is not only President Volodymyr Zelensky in Kiev who should be concerned about the condition of local bomb shelters, but also all of us in Brussels, Warsaw, Bucharest, etc on this side of the Atlantic, and in Washington, D.C., New York and other major centers on the American continent. We are staring down what might be called Cuban Missile Crisis Redux.
Another week, another Vaccine Surveillance report (now published by the U.K. Health Security Agency (UKHSA), the successor to Public Health England), and with it more worrying news on the vaccine front.
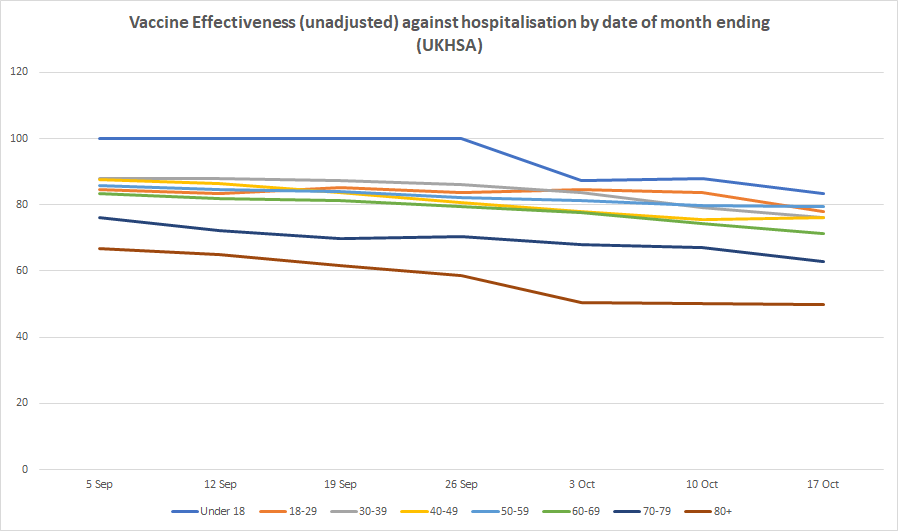
Infection rates in the double-vaccinated compared to the unvaccinated continue to rise, meaning unadjusted vaccine effectiveness continues to decline. Infection rates are now higher in the double-vaccinated compared to the unvaccinated by 124% in those in their 40s, 103% in those in their 50s and 60s and 101% in those in their 70s, corresponding to unadjusted vaccine effectiveness estimates of minus-124%, minus-103% and minus-101% respectively. For those over 80 the unadjusted vaccine effectiveness is minus-34% while for those in their 30s it is minus-27%. For 18-29 year-olds it is 25%, so still positive but low, while for under-18s it is 90%, the only age group showing high efficacy. Vaccine effectiveness against emergency hospital admission and death continues to hold up, though with some indication of gradual slide, particularly in older age groups (see below). (For definitions and limitations, see here.)


The UKHSA has continued to receive criticism for publishing this data, with claims that the figures used for the unvaccinated population are unreliable and likely too high, artificially suppressing the infection rate and vaccine effectiveness. Cambridge statistician Professor David Spiegelhalter put out a scathing tweet on these lines on Friday, but he didn’t elaborate on his claim or link to an article explaining it further.
Completely unacceptable that UKHSA put out absurd statistics showing case-rates higher in vaxxed than non-vaxxed (Fig 2), when just an artefact of using hopelessly biased NIMS popn estimates. Feeding conspiracy theorists worldwide. https://t.co/DjyhxnSm2z
— David Spiegelhalter (@d_spiegel) October 22, 2021
Professors Norman Fenton and Martin Neil have argued that in fact the PHE/UKHSA data may underestimate the number of unvaccinated rather than overestimate them, which would have the reverse effect.
Either way though, what wouldn’t change is the fact of the large and fast decline in effectiveness against infection. This is now generally acknowledged among many scientists (likely caused by waning over time or new variants or both), though has not had the logical impact on Government policy one might have expected and hoped for of eliminating the rationale for vaccine passports and mandates.
A further point revealed for the first time in this week’s surveillance report is that the vaccines may actually hobble the body’s ability to develop the strongest immunity once infected. As noted by Alex Berenson, the report mentions (in passing) that “recent observations from U.K. Health Security Agency (UKHSA) surveillance data” show that “N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination”.
The report does not elaborate on this, but on the face of it it is a startling admission. It is basically saying that a certain kind of antibody which is not produced by the vaccines but is usually produced by infection (and hence is used by PHE/UKHSA to identify those with antibodies-from-infection) is not produced so well by those who are infected post-vaccination. Insofar as this is true it means the vaccines may actually prevent the immune system from developing the strongest form of protection against reinfection. This phenomenon of the immune system being in some way hobbled by the way it first encounters a pathogen is well-known and is referred to as original antigenic sin.
There would be a number of implications of this. It would mean that since the vaccine rollout got going the prevalence of N antibodies in the population has ceased to be a reliable measure of how many people are previously infected (which might explain why it has been rising so slowly during the Delta surge). It would also mean the vaccines may make reinfections and serious illness upon reinfection more likely. Plus likely other things as well.
This is something that should be investigated fully and the results published so that its impact can be properly assessed and understood.

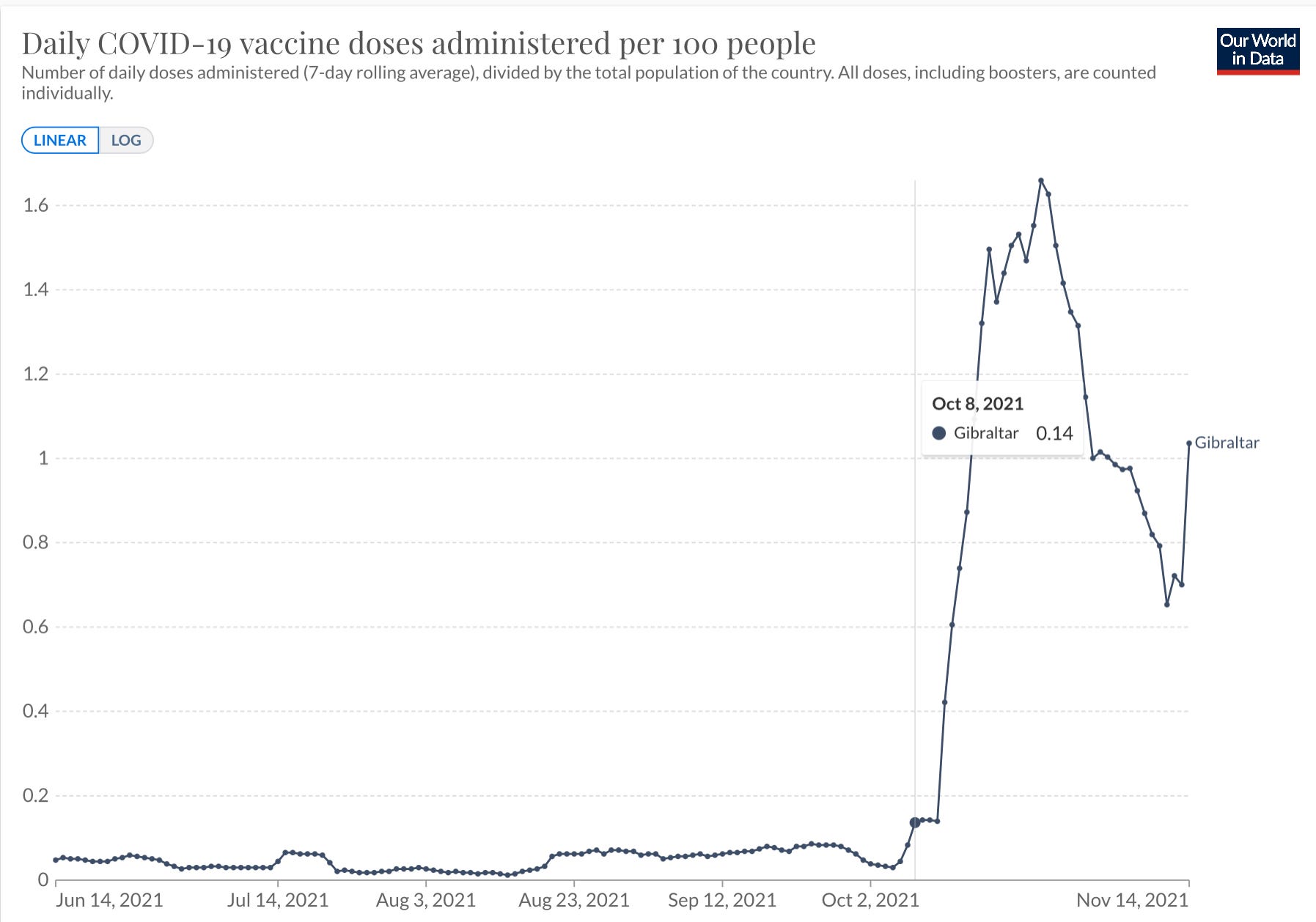
Everybody is vaccinated in Gibraltar; since October, increasingly large numbers of people are triple vaccinated there.
Here’s what their booster campaign looks like:
 a.image2.image-link.image2-1020-728 { display: inline; padding-bottom: 140.1098901098901%; padding-bottom: min(140.1098901098901%, 1020px); width: 100%; height: 0; } a.image2.image-link.image2-1020-728 img { max-width: 728px; max-height: 1020px; }
a.image2.image-link.image2-1020-728 { display: inline; padding-bottom: 140.1098901098901%; padding-bottom: min(140.1098901098901%, 1020px); width: 100%; height: 0; } a.image2.image-link.image2-1020-728 img { max-width: 728px; max-height: 1020px; }As if on cue, infections in Gibraltar skyrocketed directly afterwards:
 a.image2.image-link.image2-1068-728 { display: inline; padding-bottom: 146.7032967032967%; padding-bottom: min(146.7032967032967%, 1068px); width: 100%; height: 0; } a.image2.image-link.image2-1068-728 img { max-width: 728px; max-height: 1068px; }
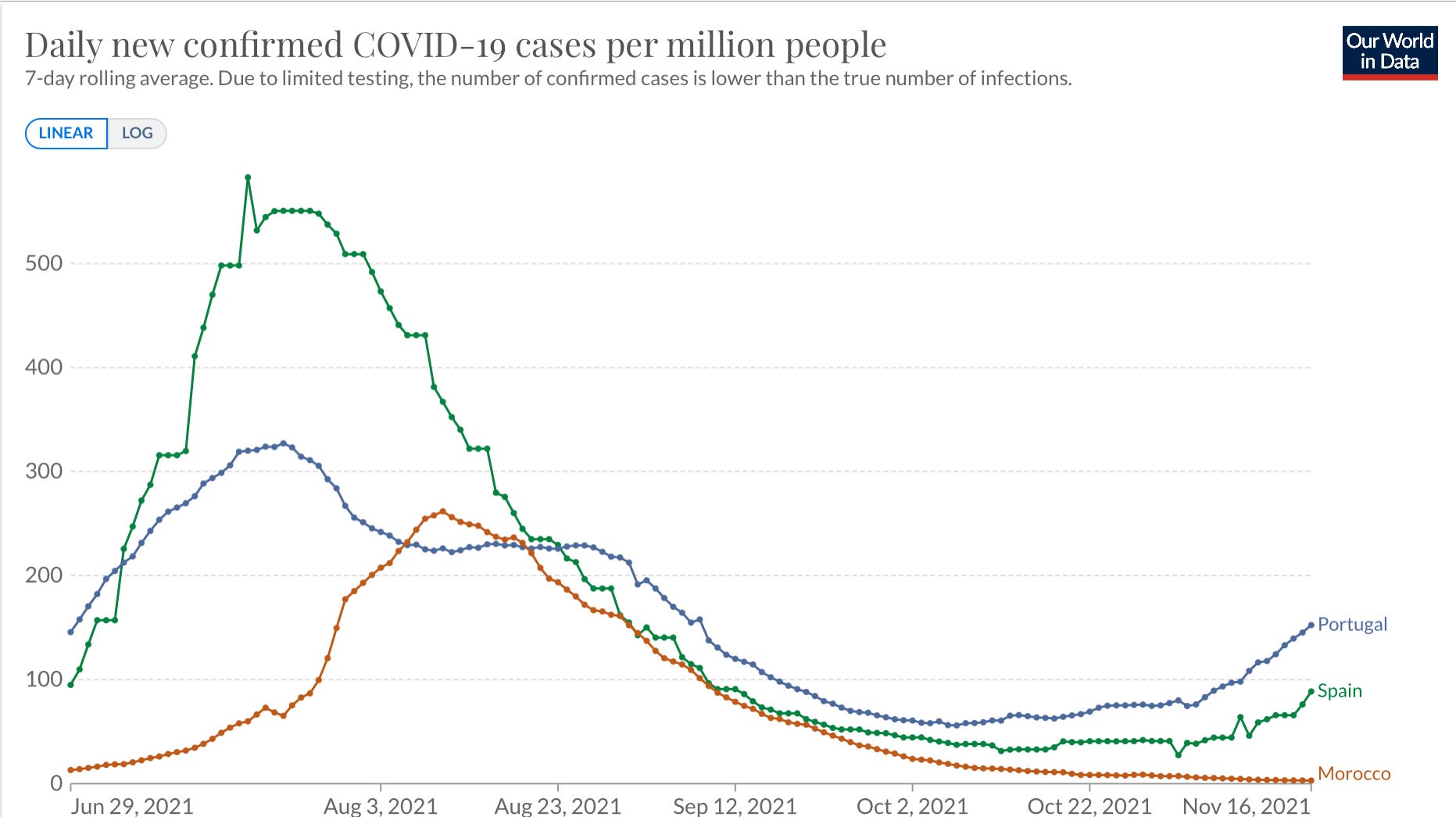
a.image2.image-link.image2-1068-728 { display: inline; padding-bottom: 146.7032967032967%; padding-bottom: min(146.7032967032967%, 1068px); width: 100%; height: 0; } a.image2.image-link.image2-1068-728 img { max-width: 728px; max-height: 1068px; }This isn’t a seasonal or a regional effect. Neighbouring countries, where the booster campaign has yet to begin (Morocco) or kick into high gear (Portugal, Spain), see a slight upward, seasonal trend—nothing like the Gibraltar spike.
 a.image2.image-link.image2-817-728 { display: inline; padding-bottom: 112.22527472527473%; padding-bottom: min(112.22527472527473%, 817px); width: 100%; height: 0; } a.image2.image-link.image2-817-728 img { max-width: 728px; max-height: 817px; }
a.image2.image-link.image2-817-728 { display: inline; padding-bottom: 112.22527472527473%; padding-bottom: min(112.22527472527473%, 817px); width: 100%; height: 0; } a.image2.image-link.image2-817-728 img { max-width: 728px; max-height: 817px; }When Israel rolled out boosters in August, they also saw spikes in infections and deaths. It is the same phenomenon we observed after dose 1. Only the second dose does not enhance infections, presumably because it is administered in the protective shadow of the first one. As with everything involving this virus and our vaccines, there are probably multiple causes at work here. For about ten days following vaccination, the vaccinated are more susceptible to infection, and a subset of them probably become minimally symptomatic super-spreaders.
Millions of people across Europe and North America will become eligible for Dose 3 at the very height of coronavirus season, in December and January. Uptake will be highest among medical professionals and nursing home personnel. There is the potential for real catastrophe here. While the vaccines don’t work as advertised, they are powerful pharmaceutical products and they have strange, unexpected effects — not only on the bodies of people who take them, but also on the dynamics of transmission and infection. Deranged medical bureaucrats, who refuse to abandon their dreams of controlling a highly contagious seasonal respiratory virus, have whole populations popping these things like aspirin. They could very well succeed in making Corona into the unprecedented public health disaster that the virus itself never quite was.
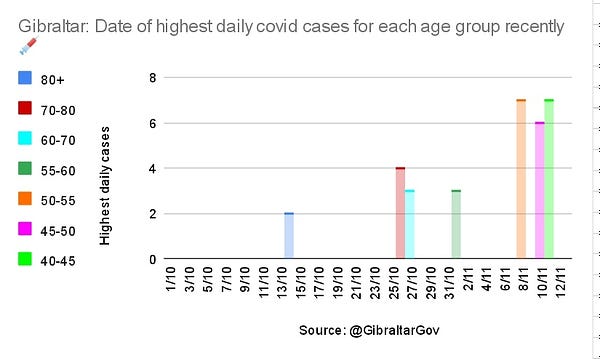
UPDATE: Always-sharp commenter someothercat points to this further proof: Infection peaks in Gibraltar are cascading from the oldest age groups to the youngest, following the order in which they were boosted.
[
 Simon @stevin2021
Simon @stevin2021
@orwell2022 @MConceptions What are the chances that the dates of the day with highest daily cases for each boosted age group in Gibraltar follow a perfect chronological order? Those vaccinated first peaked first and so on. Isn't that proof that the booster are causing the current 🌊?
](https://twitter.com/stevin2021/status/1459987142231404552?s=20)[
November 14th 2021
11 Retweets18 Likes
](https://twitter.com/stevin2021/status/1459987142231404552?s=20)
Similarly close correlations plagued Dose 1. As @kingotnik discovered in May, infections in Germany were always around 2–7% of vaccine doses administered 17 days prior. The effect disappeared only with improving spring weather.
 a.image2.image-link.image2-498-728 { display: inline; padding-bottom: 68.4065934065934%; padding-bottom: min(68.4065934065934%, 498px); width: 100%; height: 0; } a.image2.image-link.image2-498-728 img { max-width: 728px; max-height: 498px; }
a.image2.image-link.image2-498-728 { display: inline; padding-bottom: 68.4065934065934%; padding-bottom: min(68.4065934065934%, 498px); width: 100%; height: 0; } a.image2.image-link.image2-498-728 img { max-width: 728px; max-height: 498px; }This key post in the Politics of Care series stems from an invite from Norman Fenton to give a lecture on December 6 to a group interested in the evidence swirling around vaccines. It is accompanied by The Handmaid’s Vaccine on RxISK, which gives a video of the talk, whose text and slides are below. The sound effects in the video are slightly mixed at one or two point and you might need the text to clarify the points made.
This talk is for all who are interested in evidence and how we generate it as well as for a group of people who are pro-vaccine, to the point of being volunteers in clinical trials, but who have ended up being harmed by them. They are the ones doing the science and demonstrating what science means – as I’ll explain – but their work is written off as misinformation.
The company handling of SSRI harms shows we came to classify real Evidence as misinformation. Many of the company tricks involved in this effort to persuade us the world is flat will be known to you but the brazenness with which they were deployed and the failure of physicians to spot what was going on may be new.
Slide 2
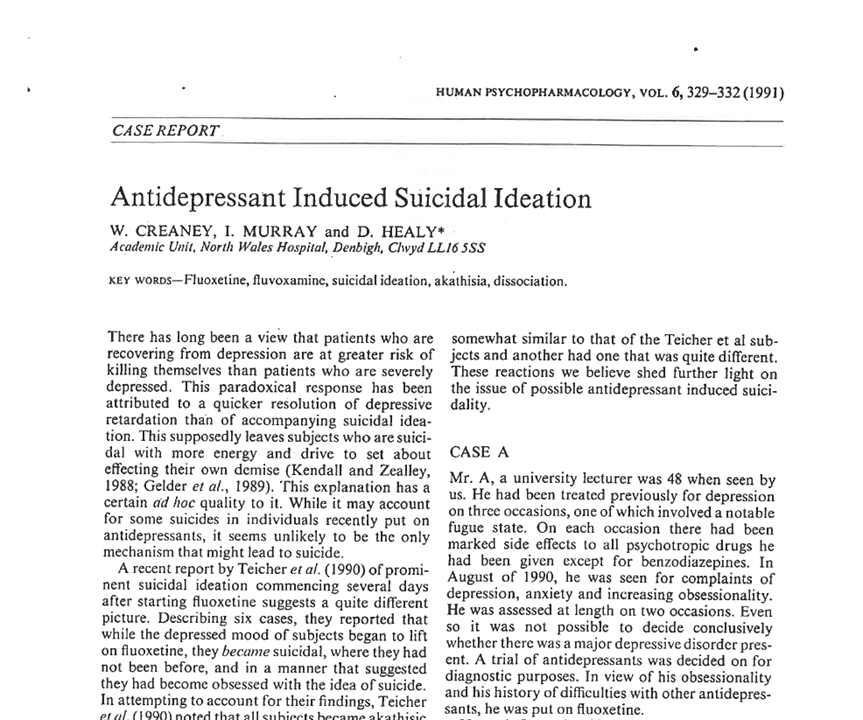
I have a doctorate in Serotonin Reuptake and was keen to try the SSRIs early on. Two men I put on Prozac became suicidal. Their problems cleared after stopping and re-emerged on starting another serotonin reuptake inhibitor and stopped again after stopping. See Creaney et al.
This is as clear a causal connection as you can get anywhere in science. I sent the cases to Lilly for comment and presented them in forums. No-one offered alternate explanations. Others reported similar cases during the year to publication of this article.
Slide 3
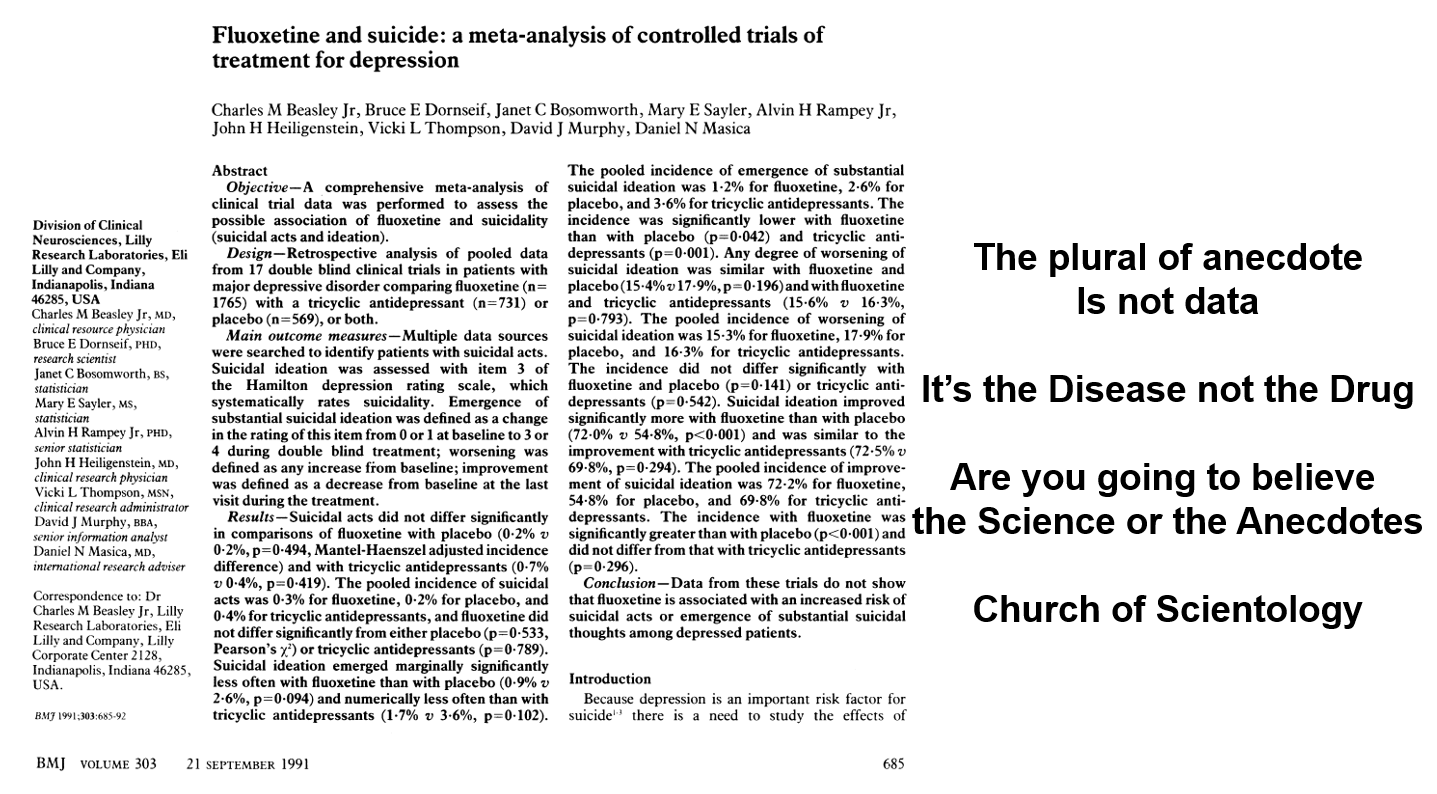
This rash of cases forced FDA to require Lilly to defend their drug. As my article came out, Lilly published this Beasley et al article in the BMJ. It came out on the same day the company presented their case at an FDA hearing – September 20, 1991 – stating:
- The plural of anecdote is not data
- It’s the disease not the drug
- Are you going to believe the misinformation or the science?
- It’s all the fault of the Church of Scientology (1991’s Anti-vaxxers).
The BMJ article shows more suicidal events on Prozac but the paper said these were not statistically significant and so there was no problem. FDA talked about heart-breaking cases reported to them but concluded the science didn’t link Prozac to the problem.
Slide 4
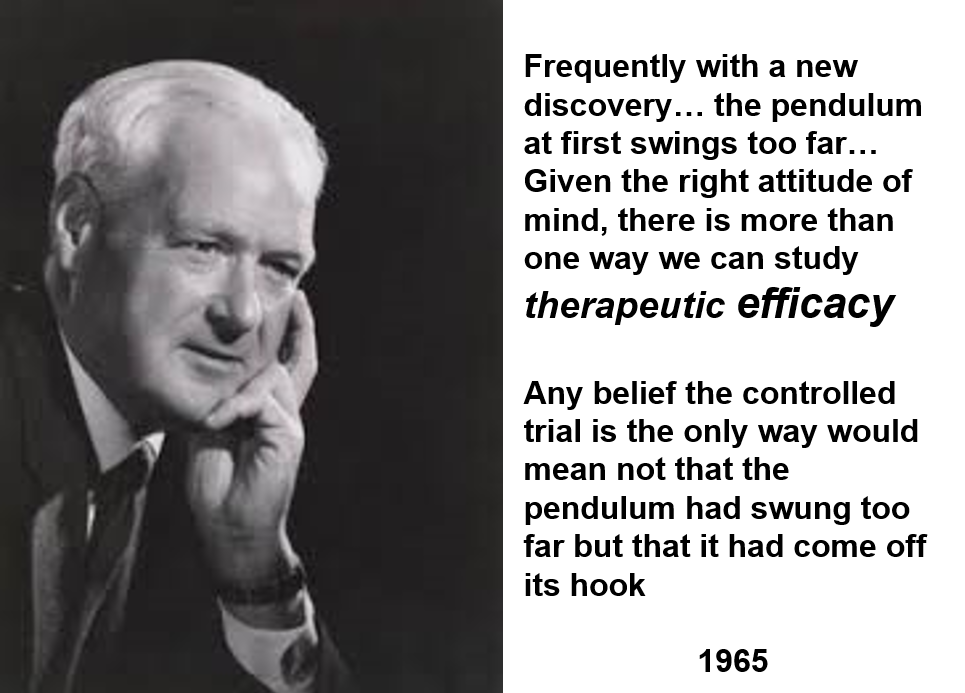
Here is Tony Hill, who created RCTs, saying 20 years later RCTs can help assess one of the 100 things a drug does – something we might be able to use for treatment purposes. This, by definition, means RCTs are not a good way to evaluate a drug. See Clinical Trials are not Safe.
Saying RCTs are not the way the truth and the light, these days, is like saying the Bible, the Koran or the US Constitution aren’t reliable.
Slide 5 Watch this.
Slide 6
In a depression trial, investigators focus intensely on one thing – does Prozac have an effect on mood. Pretty well everything else is ignored. The statistics we use don’t work unless there is an intense effort to collect everything we can about this one outcome.
And so, depression trials miss something that happens to almost everyone who takes an SSRI within 30 minutes of the first pill – your genitals go numb. You can search the RCTs on these drugs and all you will find is that perhaps 5% of people have sexual issues on these drugs.
Emotional numbing is another extremely common effect almost completely missed. This is how these drugs help. This is how these drugs might help someone diagnosed as depressed but the key point is that it is much more common than depression recovery.
Similarly in the vaccine trials, the common thing is a multiplicity of Spike protein effects – doing this we hope might help but if we are hypnotized by what is hoped for we will miss and have missed what these Spike proteins are actually doing.
If we just depend on RCTs, we end up knowing almost nothing about a drug.
The idea that an RCT shows there is a favourable Risk-Benefit ratio for a drug or vaccine can only hold true if the thing we are looking at is the commonest thing this vaccine does – like a parachute for instance. The commonest thing is a life saved and the Risk Benefit is favourable but we don’t need an RCT for parachutes.
If what we are hoping for is pretty rare – as in vaccine or SSRI trials – and in particular if we don’t know what we are missing, such as an obliteration of our ability to make love, perhaps for all time, then claiming a favourable Risk Benefit ratio is psychotic.
Slide 7
The first rating scale for behaviour was the Hamilton Rating Scale for Depression. An aid to make sure physicians checked on most of the things that might be abnormal in depression while they were interviewing a patient. An aid to help a doctor do an interview that would help the patient to live the life they wanted to live.
If you cleave to the checklist you will do very standardized but possibly disastrous interviews. For instance, on the Hamilton Scale, there is an item on suicide which could stem from the illness or from the drug – it needs a judgement call as to which of these is responsible. Ditto for sex, for sleep. Just checking yes for suicidality risks going badly wrong.
Checklists like these however became viewed as scientific instruments. They look better to hospital managers than DH asking about your daughter or partner. Without judgements, in medicine we call these diagnoses, rating scales are meaningless – other than to help a doctor to help you to live the life Pfizer want you to live.
Slide 8
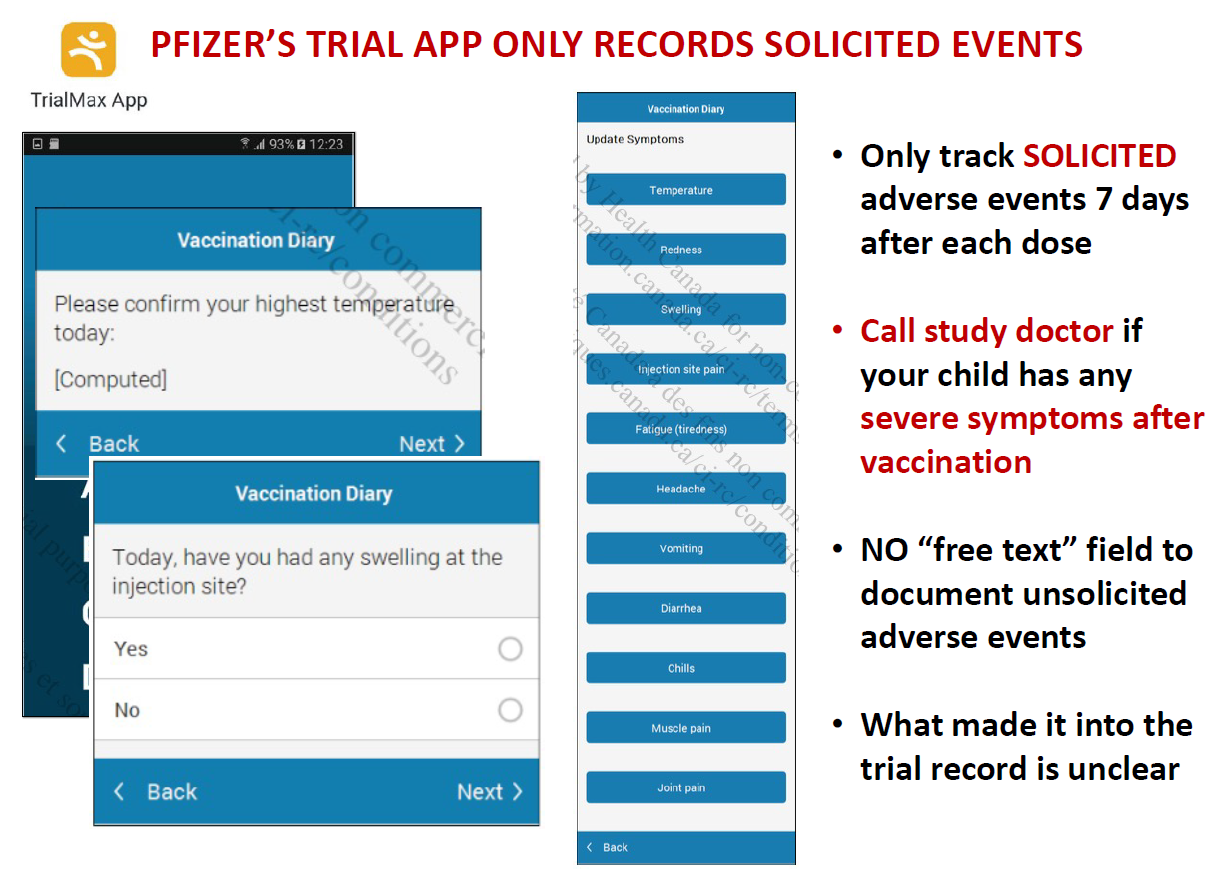
The latest twist on this story are the rating scales for adverse events companies now run electronically which let people rate up to 12 things that happen after the vaccine – such as sore arm, headache, nausea etc. This ensures certain events become statistically significant – and are put forward as a result as the only things we know for sure happen on the vaccine. See Johanna Ryan’s work on Virtual Trials.
There is no area for people to contribute anything else – so reports of other adverse events end up coming from outside the trial and are viewed anecdotes – misinformation. Companies like Pfizer tally anecdotes. What else would you do with misinformation?
Slide 9

Here is Fluvoxamine, an SSRI supposedly good for Covid. There have been lots of dropouts in the trials done on this, enough to invalidate the trial.
Side effects though could be endorsed on pre-populated lists that included cough, fever, nausea etc but not suicidality, homicidality, sexual dysfunction or the other things this drug causes that were likely responsible for the huge dropout rate.
Many look to drugs like this as an alternate to vaccines. Some doctors advocate them as our Hi Tech versus Albert Bourla’s Hi Tech. There are lots of low tech things that might be more helpful like getting you off some of the Tech you’re on rather than throwing more Hi Tech at you.
As we throw Hi Tech at you, we miss the fact that RCTs convert poisons, from whose use we hope to bring some good, into sacraments – something that can only do good. Most believers figure having as many sacraments as you can daily is a good thing where its seems equally obvious to most of us that taking more than one poison at the same time is unlikely to be all that safe.
One more quirk is companies always want their Ugly Ducklings to have an I’m a Swan moment – thalidomide was the fourth most profitable drug in the US last year but will be pushed down to fifth by Albertine this year. Thalidomide is a drug that causes suicidality, sexual dysfunction and birth defects – just like the SSRIs including fluvoxamine.
Slide 10
For drug companies, rating scales ensure you do an interview that produces figures which are the most seductive way to get the patient on their drug. The interview helps you to help them to live the life Pfizer want them to live.
This is not just true for rating scales, it is true for any measure – peak flow rates, bone densities, blood pressure or lipids, or sugar. It may be important to do something about some figures, but the goal is to help people to live the life they want to live – not the life Pfizer want them to live.
A stopwatch can be a wonderful motivator to achieve a dream – it provides data from one fraction of our lives. If we remain on top of that fine – but what about weighing scales? Just after they were introduced we got the first descriptions of anorexia nervosa. In the 1920s, they had norms for ideal weight attached to them and eating disorders mushroomed. They migrated into our homes in the 1960s and eating disorders became epidemic.
It’s very difficult to ignore figures for weight. Without data from every other aspect of our lives at the same time, we risk being trapped by this one data source. We become neurotic.
Can we let bone densities remain thin, or lipid levels remain high? Yes, we can. You think of post-mortems as something that reveal what we died from – they more often reveal what we can live with.
Slide 11

Figures create risks and pharma makes money from treating risks rather than diseases. We are seduced into taking drugs when we are healthy.
The Covid dashboards are a great mechanism to generate perceptions of risk and fear. The vaccines of course treat risks – not disease.
The Meatloaf title Paradise by the Dashboard Light is what Pfizer sees but its Hell by the Dashboard Light for us – this now extends to the evaluation of lectures and ensures we pander to people rather than challenge them.
It’s extraordinary how little we have put into treating SARS-Cov, the disease in this case and its associated pneumonia. Curing diseases is not a good business model.
Slide 12 As Peter Drucker, the Guru of Marketing Science put it 50 years ago:
The goal of marketing is to make selling superfluous. The aim is to know and understand the customer so well that the product or service fits and sells itself.
Slide 13
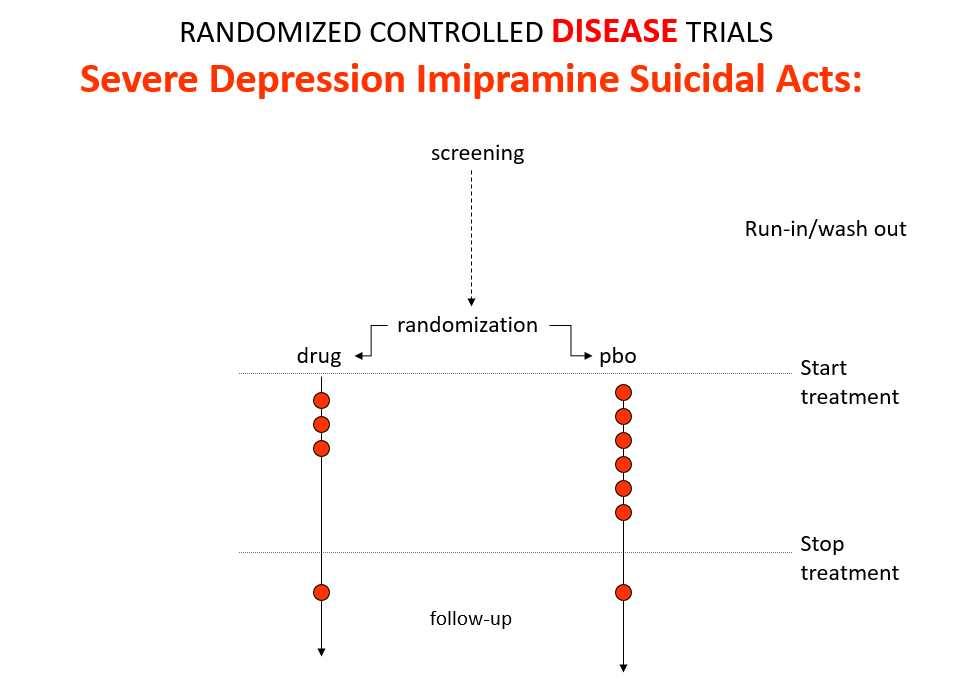
Imipramine was the first antidepressant. It beats the later SSRIs in RCTs. It treats melancholia – they can’t. They are useless for severe depression. Melancholia comes with a high risk of suicide.
Imipramine was launched in 1958. A year later at a meeting in England, Danish psychiatrists made it clear that while it was a wonderful treatment it made some people suicidal.
Let’s do a thought RCT of imipramine versus placebo in melancholia. Even though it can cause suicide, we would expect it to reduce the number of suicides because it treats the condition. This RCT would be great evidence antidepressants do not cause suicide.
Slide 14
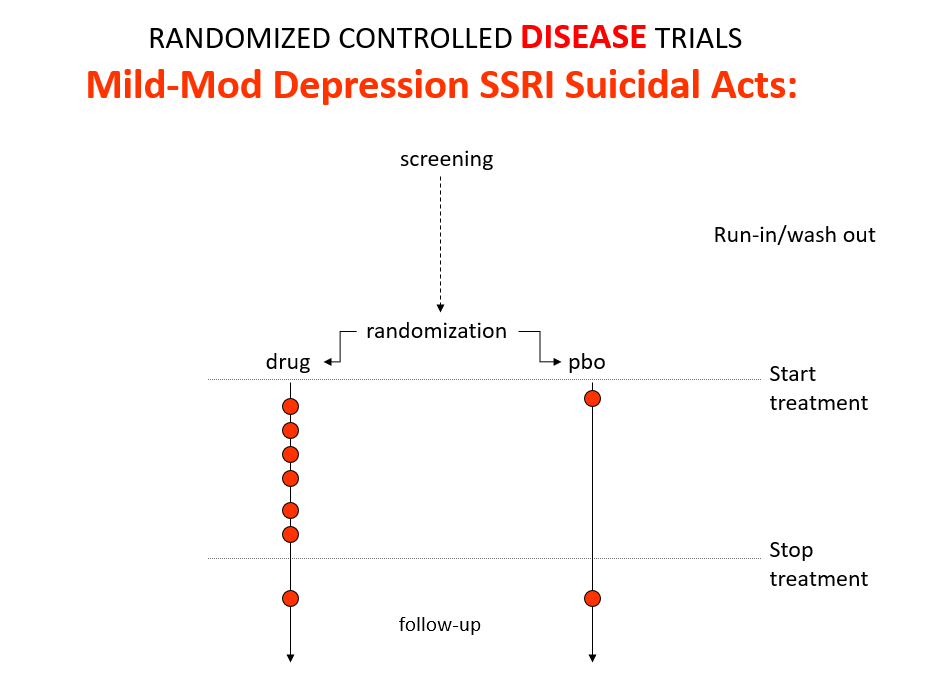
Here is the data on the trials in mild depression that brought the SSRIs to market – a doubling of suicidal events compared to placebo.
Slide 15
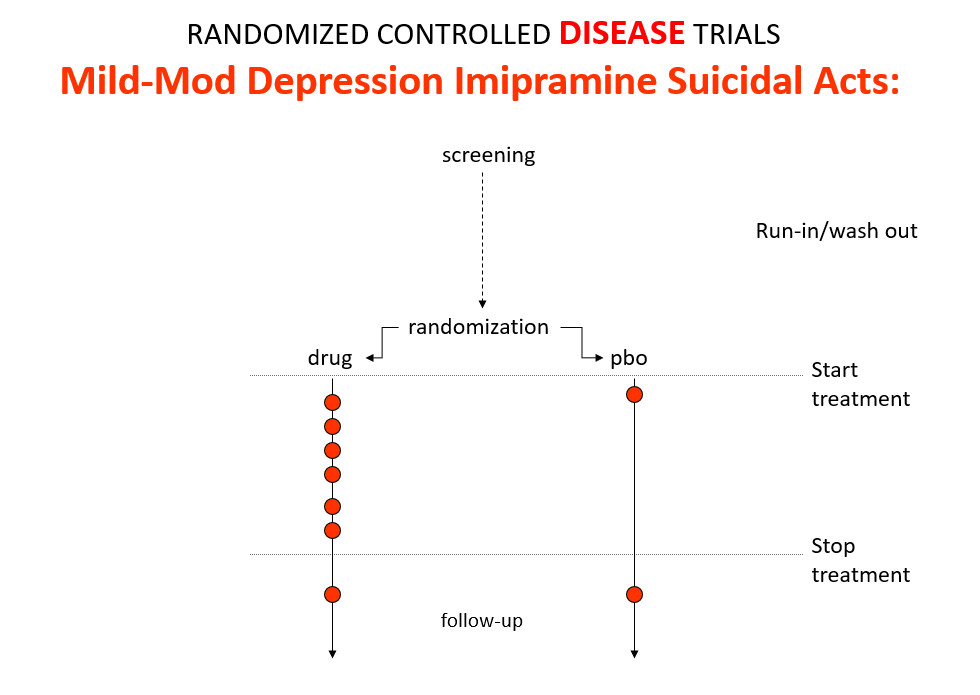
Imipramine looks the same in mild depressions. Now it too causes suicides. So RCTs tell us nothing about cause and effect – they can give us diametrically opposite answers. This is because these aren’t drug trials. They are Treatment Trials and in any clinical Trial, the condition confounds the effects of the drugs.
People evaluating drugs pre-RCTs knew this. When a patient becomes suicidal in a trial you have to use your judgement to work out what has happened but you are told not to.
Slide 16
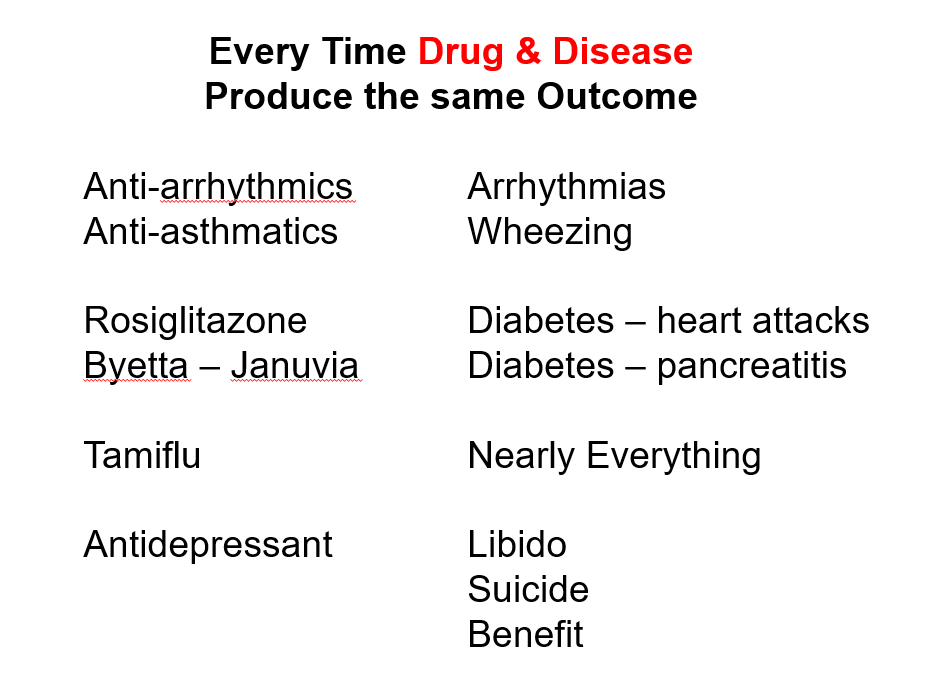
This is true in every clinical situation where drugs and conditions cause superficially similar effects – diabetes and glitazones both cause heart failure, osteoporosis and bisphosphonates both cause fractures – and this makes it impossible for an algorithmic exercise as most RCTs are to establish what is happening.
Slide 17
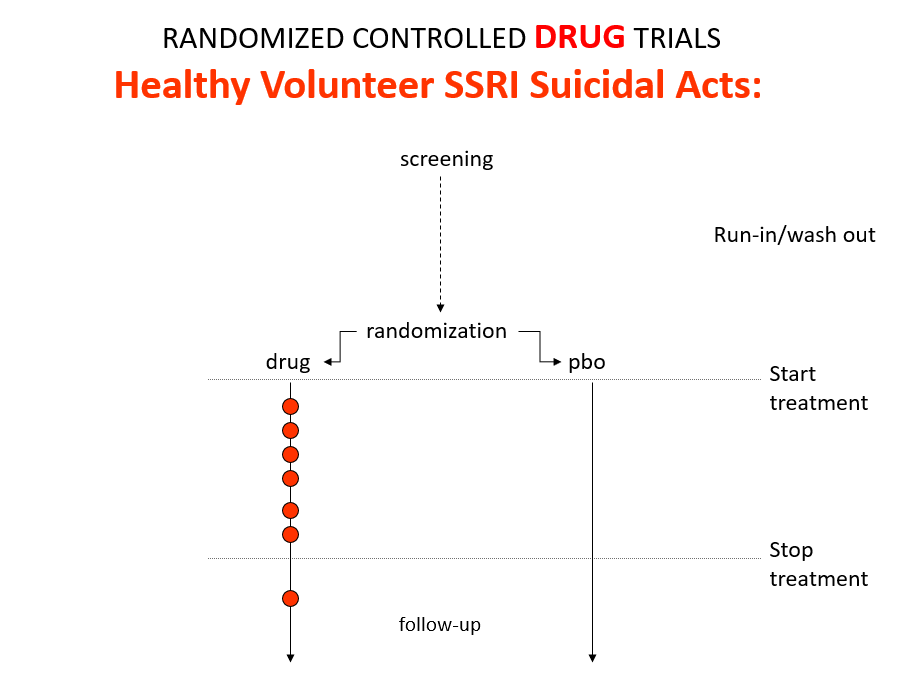
Here is what a real drug trial looks like. Companies ran these studies in the 1980s and found that SSRIs make healthy volunteers suicidal, cause dependence and sexual dysfunction but we heard nothing about this when the drugs launched. These Trials enabled companies to game their Treatment Trials to hide these problems.
Vaccine trials are healthy volunteer trials.
Slide 18
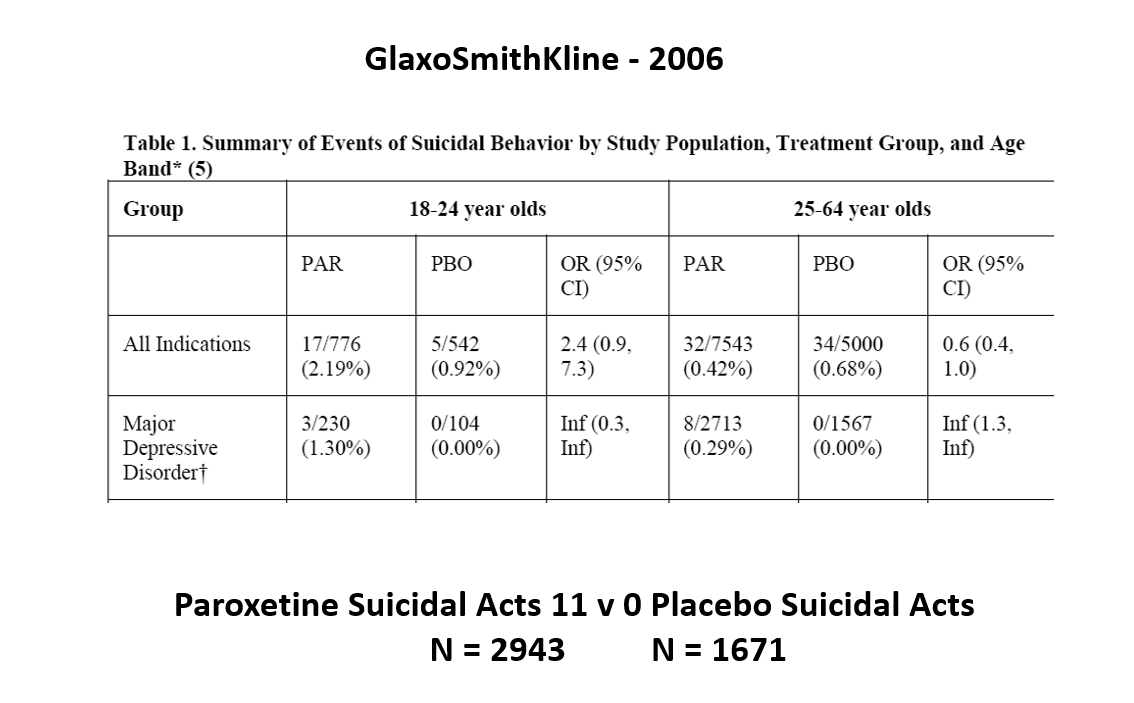
This slide shows data straight from a 2006 GlaxoSmithKline paper. GSK’s SSRI paroxetine was in trouble – the RCTs data for Major Depressive Disorder seem to show paroxetine causes suicidal events. The real data are likely worse that GSK admit to here.
Slide 19

But never fear RCTs come to the rescue. GSK also did trials in people with Intermittent Brief Depressive Disorders – IBDD. These are borderline personality disorder to most people – patients who have suicidal events much more often than anyone else. But these patients can meet criteria for depression and could be entered into Depression RCTs.
Slide 20
Prozac in these patients didn’t work. Paroxetine didn’t either and had a 3-fold higher suicidal act rate than placebo. GSK then did another trial in a similar group of patients. Why?
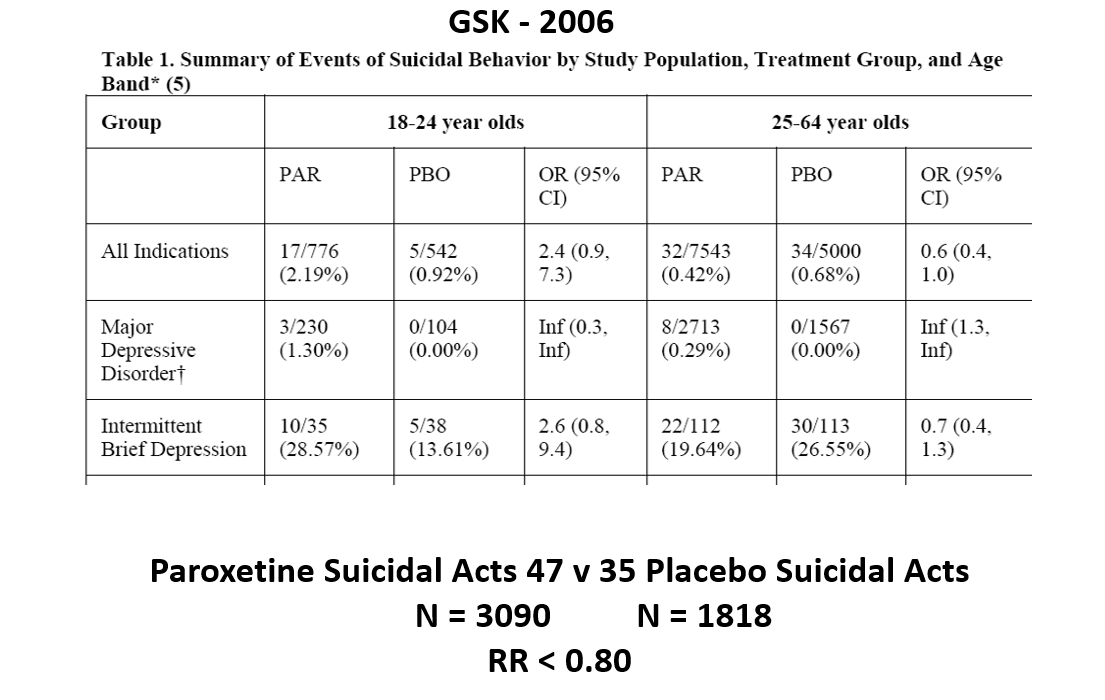
The answer is here. Here are IBDD data from the two GSK trials. I have seen other data for these two trials which make paroxetine look worse but let’s stick with GSK’s story. We could even add 16 more events to the paroxetine arm and still get the same magical outcome
When you add the IBDD data to the MDD data – all of a sudden paroxetine doesn’t cause suicidal events it protects against them.
Something like this must happen in every treatment trial with heterogenous patients – back pain, breast cancer, diabetes, hypertension, osteoporosis, parkinson’s disease. We can use an effect a drug causes to hide an effect a drug causes.
RCTs are not a way to work out what is going on. Back pain trials will insist you use analgesics rather than antibiotics – which is wrong for the 10% of backpains caused by infections.
Slide 21

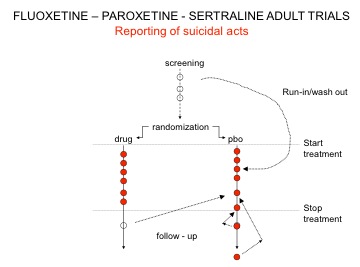
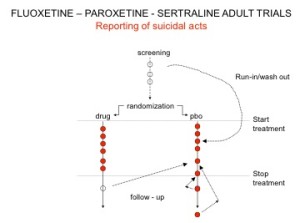
You’ve seen the son of this slide before. Here are the parents. In all AD RCTs there was a 2-week washout period during which patients were whipped off prior medicines. We now know this was a tricky thing to do – it gives lots of suicides – a bit like the two-week post vaccine period.
But companies argued as the patients were on nothing, all these events should be counted as placebo events – as the diagram here illustrates.
Slide 22
The Prozac 1991 paper had an increased number of suicidal events – but hey not statistically significant. Undo this maneuver –– and they are statistically significant.
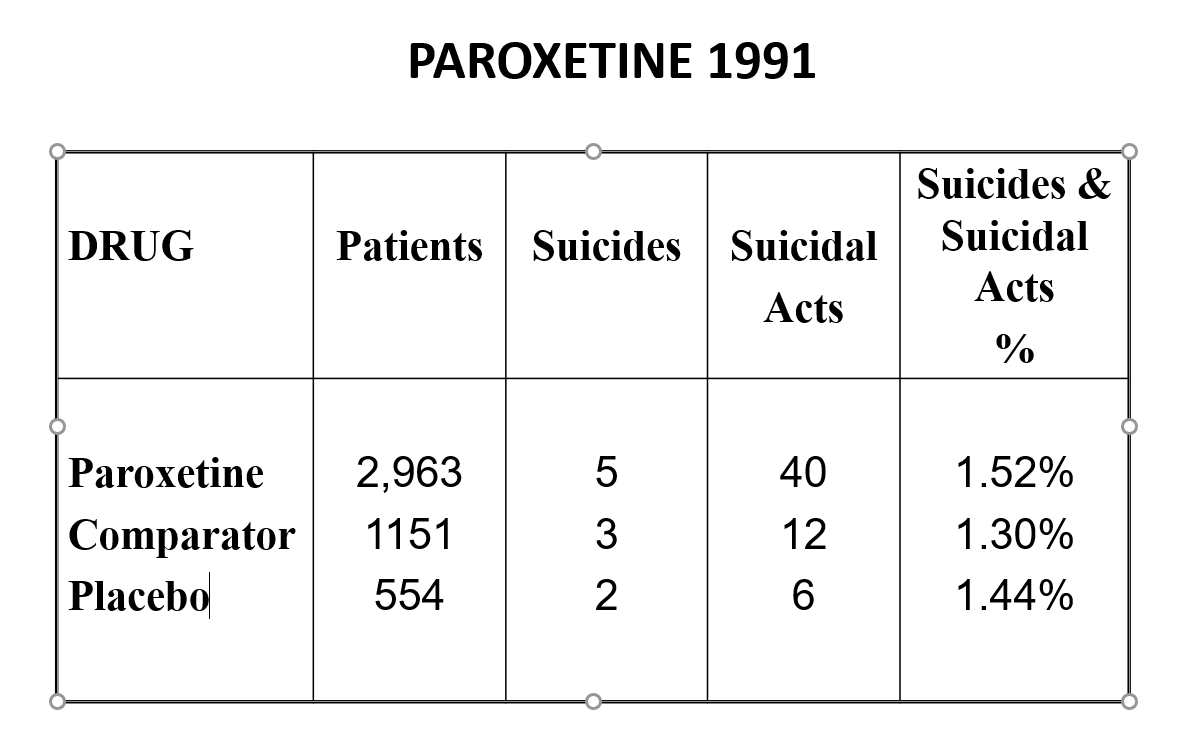
Here are the paroxetine data presented to FDA. We’d prefer the figures for paroxetine to be better than placebo but what’s a fraction between friends.
Slide 23

Undo the washout maneuver and this is what the data looked like. FDA knew what was going on and that it breached regulations and did nothing. And these figures don’t look like a drug that should be approved without warnings.
Slide 24
When that was rumbled, companies changed the game. Patients terminated from their SSRI who went into withdrawal and became suicidal were viewed as placebo, while those who stopped placebo and were put on an SSRI and committed suicide were classified as a placebo suicide – on an intention to treat basis. Regulators didn’t ask questions.
Slide 25
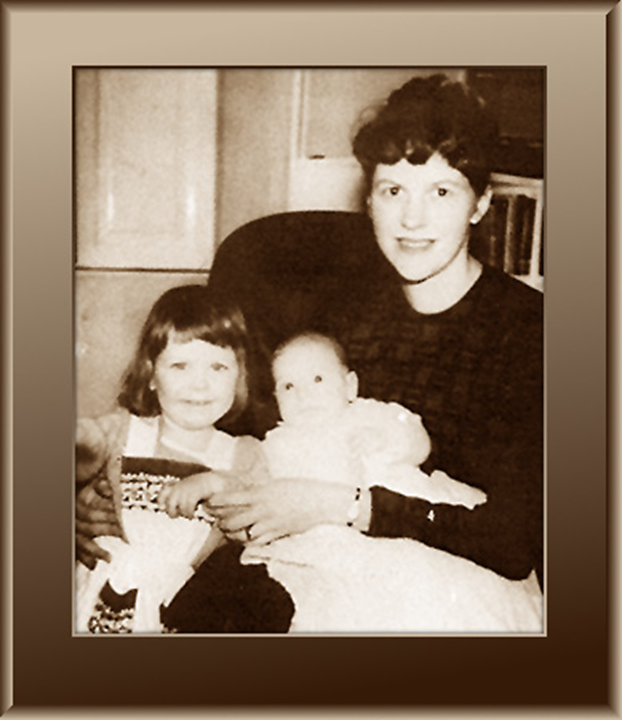
Sylvia Plath committed suicide a week into an antidepressant – a common timeframe.
Slide 26
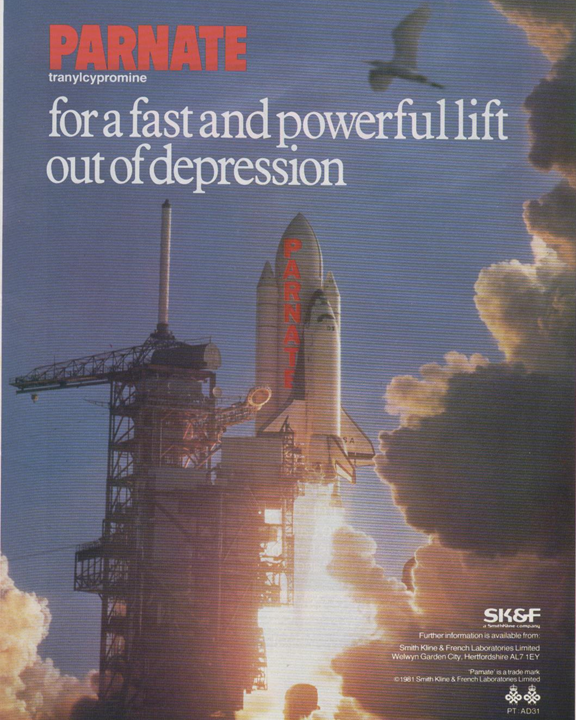
This advert is for the type of antidepressant she was given, an MAOI, featuring a space shuttle, aimed to giving doctors the impression this drug will get their patients into orbit faster.
Slide 27
Here is a space shuttle – the safest transport ever per million miles travelled – but not so safe if expressed in terms of exits from and entries back into earth’s atmosphere.
Rather than express suicidal events per patient exposed companies stuck to events per thousand patient years – having taken care to ensure some patients doing well remained in extended follow-up for months or years.
Slide 28
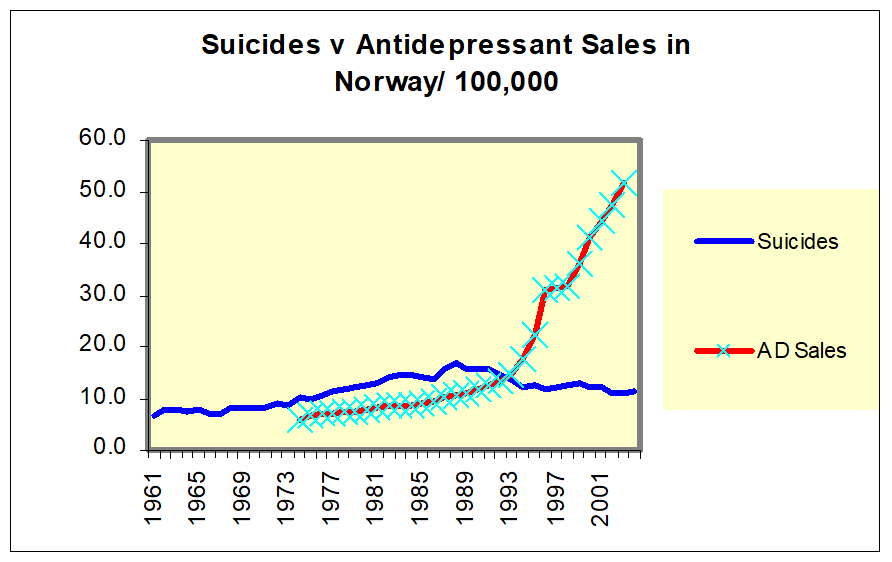
When the RCT data turned tricky and we got Black Box Warnings – companies turned to Real World Evidence – like national suicide rates. Here you see the claims for Norway which were typical of all Nordic countries – as SSRI use increased suicide rates fell – which is not compatible with the SSRI data.
If you look though suicide rates are going up with pre SSRI AD use until about 1988 – 3-4 years pre SSRI when they begin to fall.
Slide 29
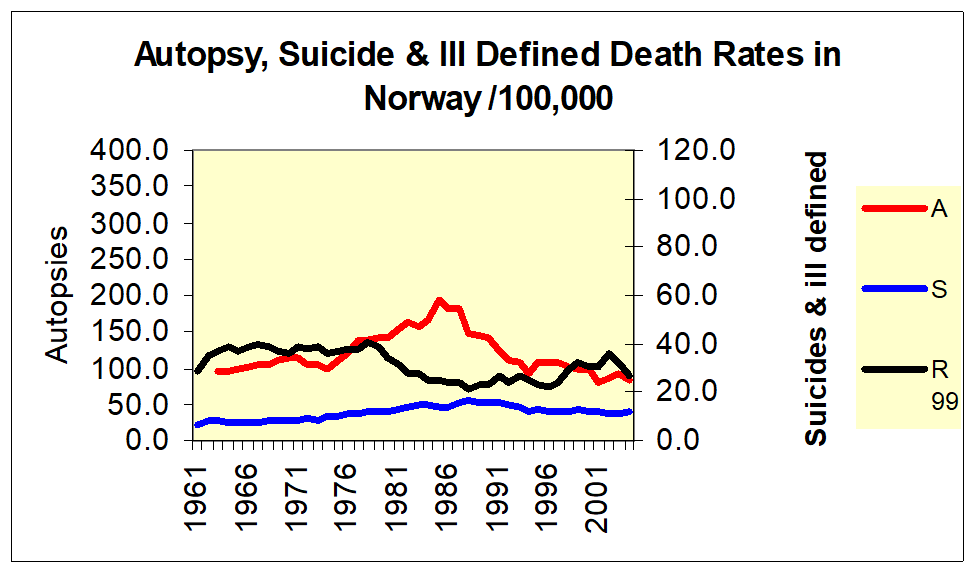
Here is Norway again where you see suicide rates falling from 88 or so and what you see if them rising as autopsy rates rise and then falling in step – as ill-defined deaths fall and rise.
Slide 30 This is true for all the Nordic countries – See Reseland et al.

Slide 31
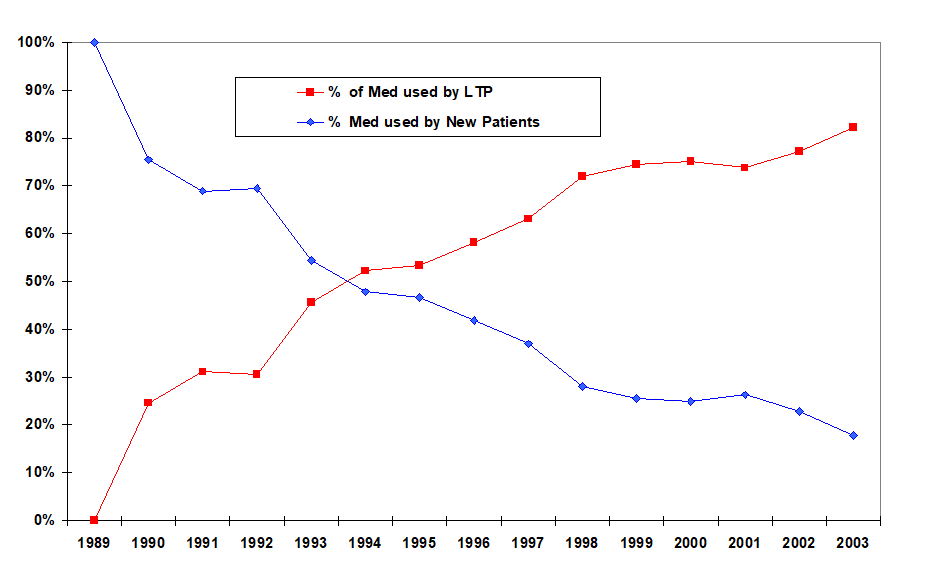
We routinely hear that SSRI use is escalating. It’s not – the same number of people go on them each year. The increase speaks to the growing numbers who are dependent on them.
Slide 32
This has implications for suicide rates – you are only likely to see an effect on an index like this during the first few years. In the case of vaccines, this years rate of myocarditis and thromboses will become the new normal – See Healy and Aldred 2005.
Slide 33
In 1999 I was asked to participate as a speaking at a company symposium in London – speakers would need to produce articles for a supplement. I said yes and soon after had an email with my article. It was a great Healy article saying the things Healy say in the way he says them with Healy references. No one who knew my stuff would pick it out as not mine.
I emailed back saying I figured on writing my own. There was surprise at the other end but they said okay. I sent it on to them and they said this is rather good but there are some important commercial messages in the other one – we’ll get Siegfried Kasper to put his name on it.
Here it is – only one word changed from the original paper – the name of author Kasper. Everybody in Vienna knows this but its done no harm to SK’s career. You can find materials saying you can trust doctors like Kasper because they have written a 1000 articles or more. Its still a great Healy article etc.
Slide 34
A year later I was in Pfizer’s archive where even the loo-paper was stamped confidential. I came across this working document – which was the articles on Pfizer’s SSRI Zoloft being managed by Current Medical Directions – a medical writing company.
Slide 35

Inside there are pages listing the articles published or in train on Zoloft for the anxious, the depressed, the young, the old etc – here you see the PTSD page.
You will see on the right – the articles were written for these essentially negative studies saying the drug worked wonderfully well. One would go to NEJM – the other to JAMA. And on the left – you see TBD – authors names are To Be Determined. Pfizer’s marketing department will work out who would be the best sales people for the drug.
This is not just a mental health issue. It holds for all treatments across medicine.
Slide 36
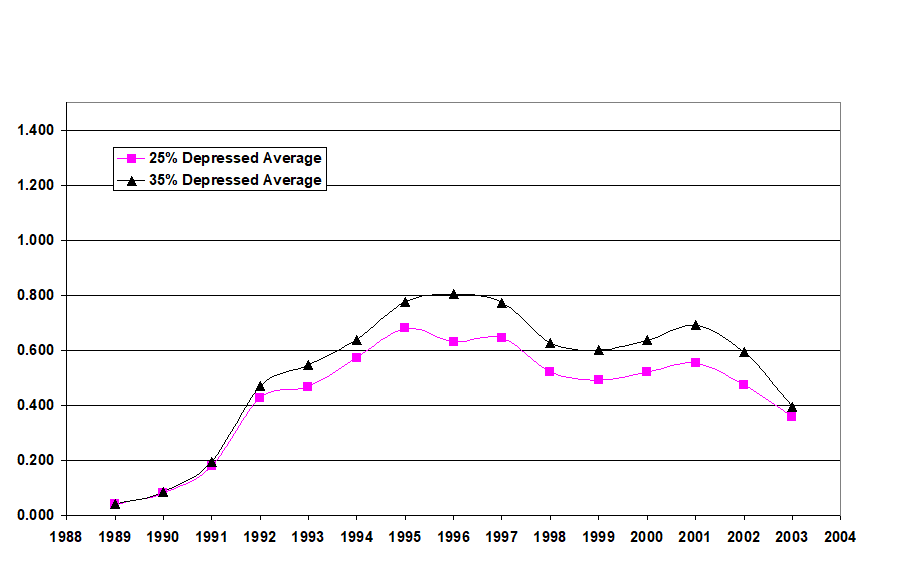
Here is the most famous RCT of all time. It has a distinguished authorship line and is in the journal with the highest impact factor in child psychiatry and says paroxetine works wonderfully well and is entirely safe for children who are depressed.
Slide 37
This internal GSK document from 1998 shows the company knew the trial had shown the drug didn’t work and proposed taking out the good bits of the data and publishing those which is the article you have seen. New York State took a fraud action against GSK on this basis who were also fined $3 billion which led to access to the trial data and what you are going to see next.
Slide 38 The full story is on Study329.org
Slide 39
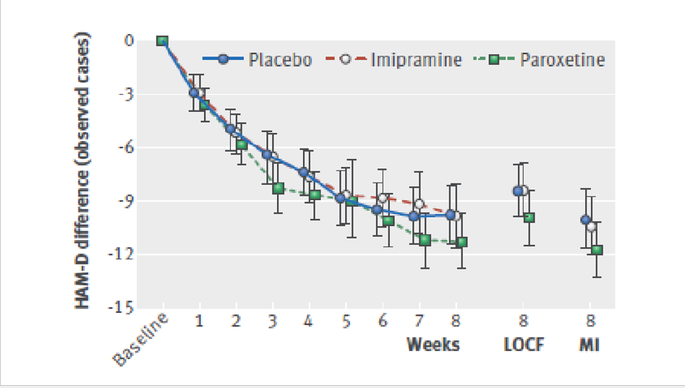
Through this legal action we got access to company data no one ever sees. The efficacy data is pretty irrelevant, but it was still possible to show that no matter which way you cut the data paroxetine was not more efficacious than placebo.
Slide 40

The tricks used to hide the problems were the real interest in these data.
The original article had 10 pages. Regulators see an 800-page Clinical Study Report (CSR) plus nearly 5000 pages of appendices – these are notional they are there but no-one in MHRA or FDA will look at them. We saw these and a further 77,000 Clinical Record Form (CRF) pages.
Point 2 points to data that just didn’t get transcribed from the 77000 pages to the 5000 pages. Point 10 is patients on placebo got SSRIs – I can explain how. But I want to focus on the coding issues.
Slide 41
The psychiatric adverse events all got grouped in CNS or neurological events – into which the groupers also put headaches and dizziness. The dizziness was not neurological – it was cardiovascular because it this case the comparator drug lowers BP especially when used in double or triple the adult dose.
The effect of this was to drown out the signal from psychiatric adverse events. So there is an issue about grouping. We were sensitized to this by Elizabeth Loder, the BMJ editor handling out paper – which took over a year to publish with 7 review rounds and 7 reviewers – who objected to our every mention of headache. As it turned out was a headache-ologist, who was an opinion leader for GSK but above all was the wife of an attorney working in Ropes and Gray who had been the lawyers defending GSK against the $3 billion fine.
Slide 42
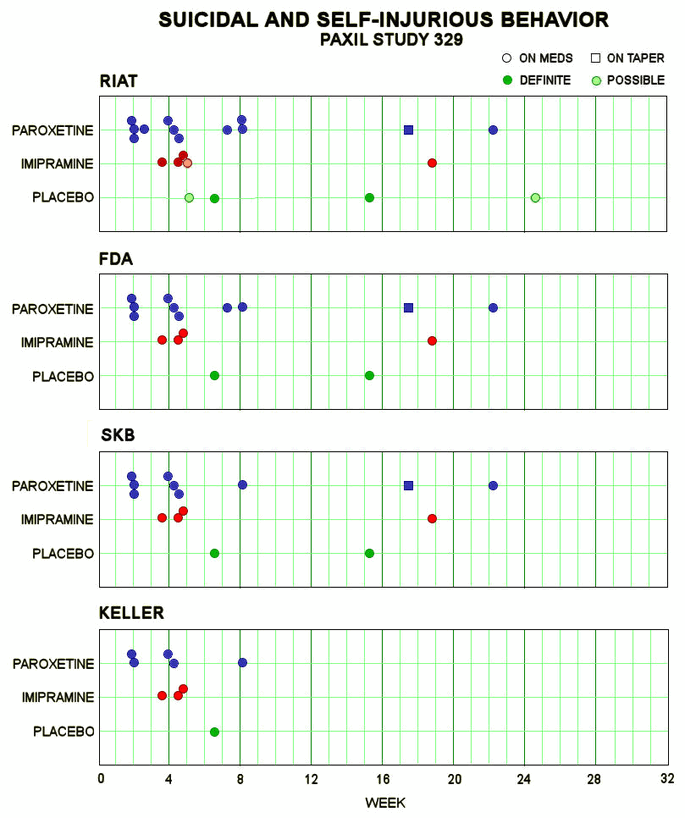
So here, leaving out headache and dizziness, in the lower bar you see the number of suicidal events in the Keller paper – once you decode them from emotional lability. In the middle bar, GSK revised this after being asked to do so by FDA when a fuss blew up. In the upper bar you see that we found more again – and there were more than we missed as I’m about to tell you.
Slide 43
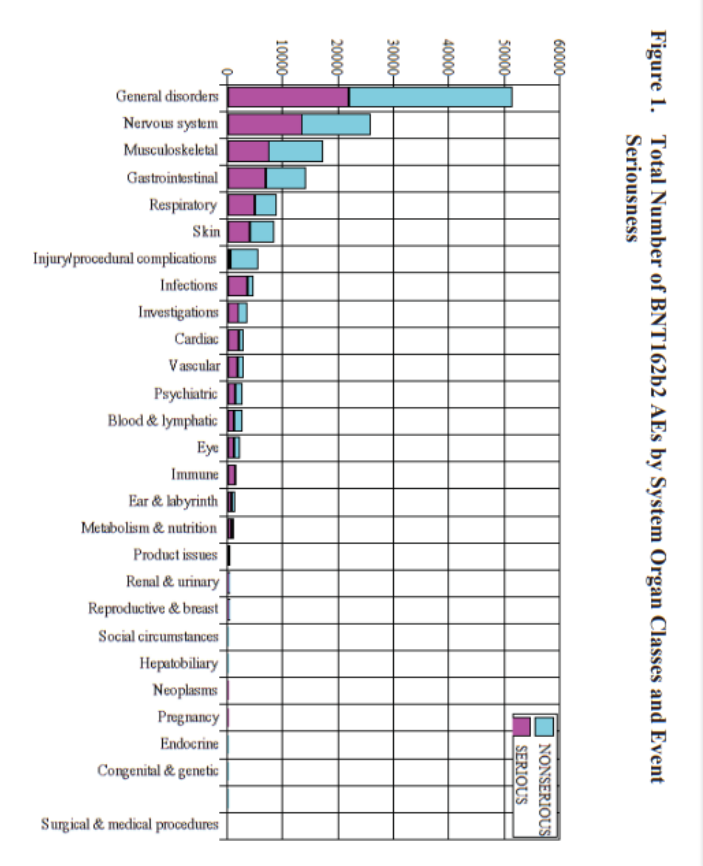
How does this fit Co-Vaccines? Well, here you see Pfizer’s report of their adverse event data – a ton of them have disappeared into a higher order coding group called General Disorders. The crimson half of the bar shows you these are serious, potentially lethal. General Disorders is a meaningless group – it needs unpacking.
Slide 44

In a Pfizer trial, one man poured petrol over himself and set a match to it, intending to kill himself. He died 5 days later from his burns. His death was coded as burns. But the company had to write a Serious Adverse Events narrative and if you got to see that you could work out that he should have been coded as suicide.
Slide 45

Companies have found a way to get around this, as found out after Study 329 finished. Here is a young man on a street waving a gun. Its Kyle Rittenhouse. In Study 329 a boy of 15 was picked up out on the street waving a gun around and threatening to kill people. He was hospitalized and should therefore have had an SAE narrative but the company coded him as intercurrent illness.
Four children dropped out of Study 329 coded as intercurrent illness – all were taking paroxetine. Add them into the picture you have just seen and things look a lot worse.
What is intercurrent illness? This was almost certainly an adverse event on paroxetine but invoking an intercurrent illness that means you really should not have been entered into this study means there is no need to write a narrative. This loophole has been there for 25 years and FDA have not moved to close it.
Slide 46
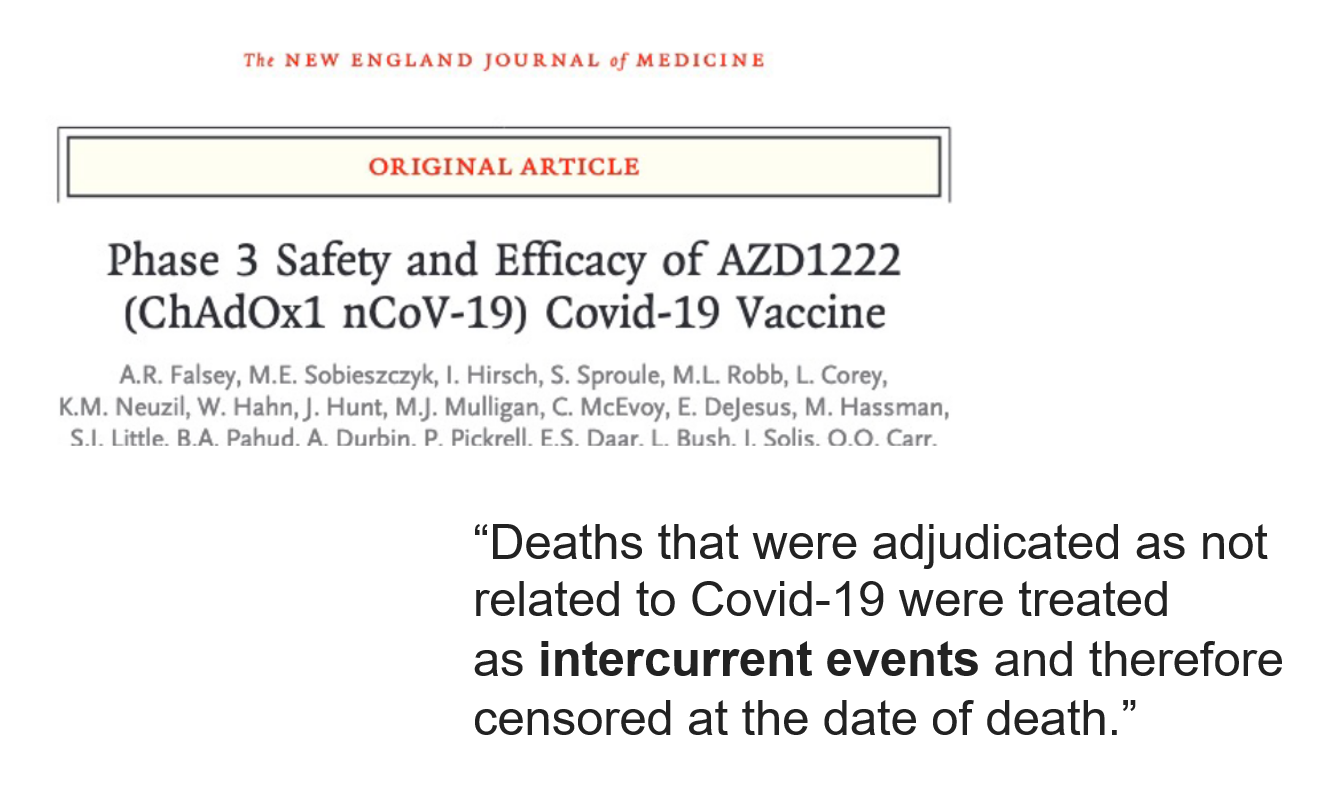
We know Astra-Zeneca broke the blind and got rid of serious adverse events like the ones that happened to Bri Dressen – see New England J of Misinformation. Here you see intercurrent illnesses turning up in this same Astra-Zeneca trial.
Slide 47
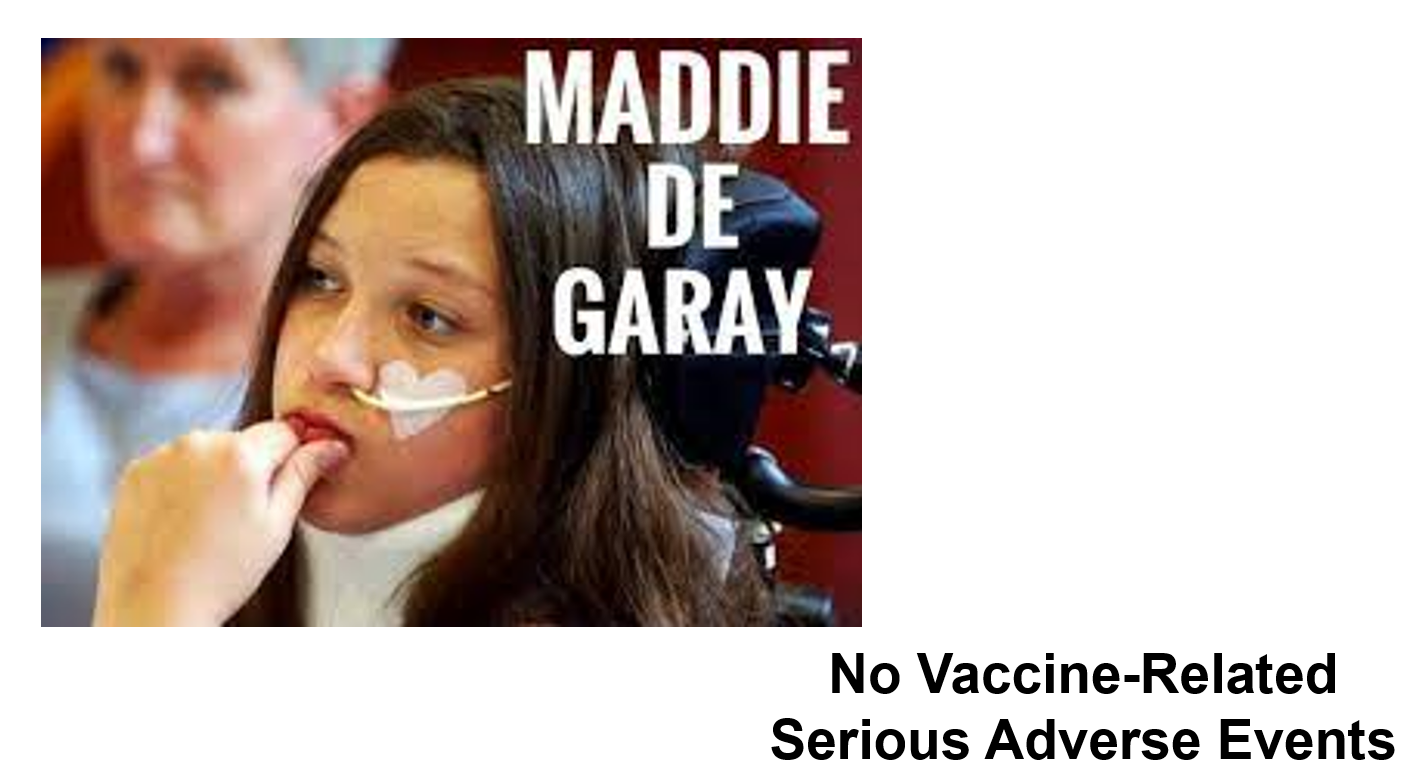
Here you have Maddie de Garay who has been tube fed and needs a wheelchair since a few days after the second dose of Pfizer’s vaccine in their trial for 12-15 year olds. But the company says no serious vaccine-related adverse events happened in this trial. They claim she has hysteria and of course that antedates the trial and so the vaccine can’t have caused it.
Slide 48
Few people know that FDA approved paroxetine for children – here is part of FDA’s 2002 letter of approval to GSK. The key bit is typed up so you can read it. The date is important – the Keller paper was 2001.
You can see here GSK told FDA that Study 329 was negative and you see that FDA agreed to approve the drug on the back of three negative studies and also agreed that there was no need to mention this in the labelling. Why would FDA do this?
Slide 49
Here are the published results of adult trials of antidepressants nearly a decade earlier. The picture looks pretty good.
Slide 50
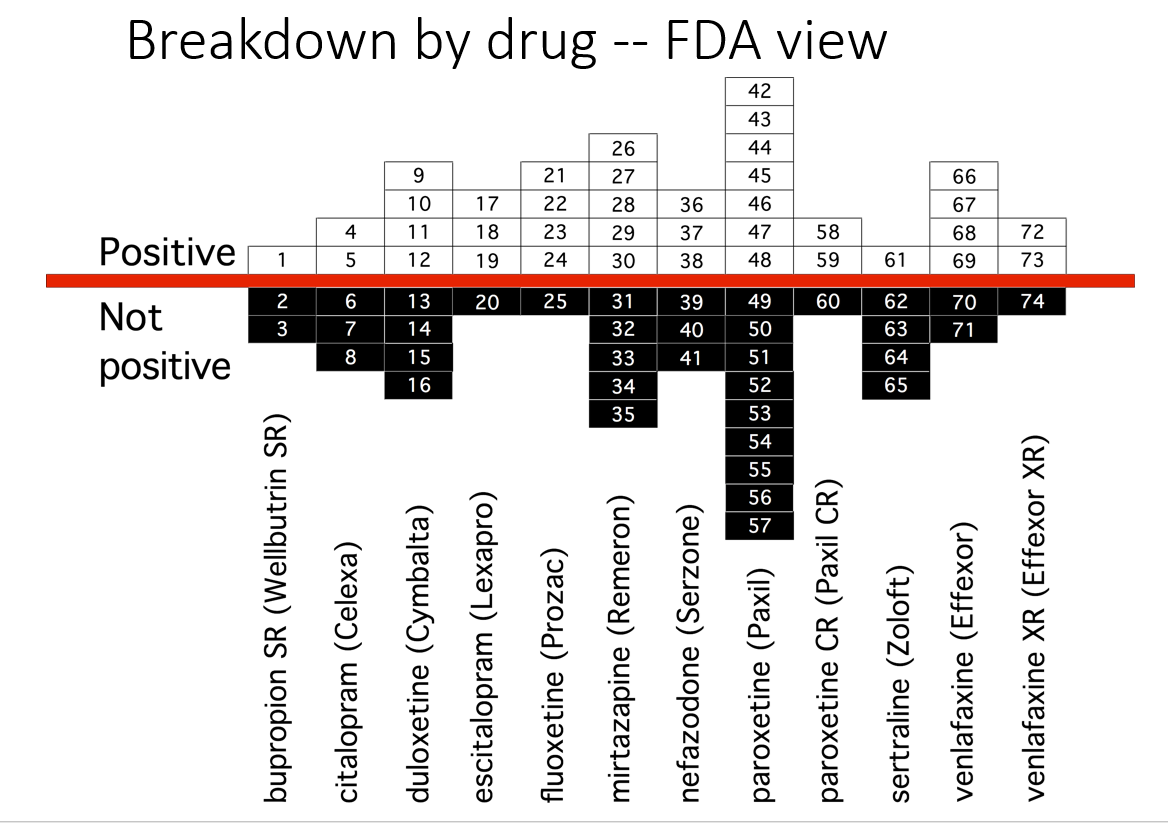
But as Erick Turner has shown, this is how these studies looked to FDA. A different picture. Companies don’t leave negative studies unpublished, they know FDA are happy to let them publish negative studies as positive.
Why? Did GSK tell FDA – if you tell the world Study 329 was negative, we might get sued for fraud – which they did and fined for $3 billion. FDA don’t feel inclined to blow this whistle and MHRA and EMA have even less incentive.
Slide 51
So here is Study 329 again. The author is not listed. In the case of trials done in children, pretty well the entire literature was company written. The mismatch between what articles claim and the data when we see is the greatest known divide in medicine but likely not atypical. Study 329 was a good and ethical trial compared to some of the current vaccine trials.
There are now 45 negative trials for antidepressants in minors – out of 45 trials done. Yet antidepressants appear now to be the second most commonly taken drugs by teenage girls.
Slide 52
In this New England J of Misinformation article, the first thing to note is the author is not listed here. Twenty of the 29 apparent authors are company people. Few are clinicians and none are likely to have seen anyone harmed.
Second the trial was run by I Con rather than Pfizer who subcontracted to Palladium Research, who subcontracted to Ventavia and we know Ventavia ran a shit-show.
Anyone with experience of company trials knows that it is worth looking at the centres involved because for instance in a trial of aripiprazole where there might be 33 centres with 30 producing results for the drug that would not get approval, but perhaps 3 in places FDA won’t visit that found every patient put on the drug did fabulously and every on placebo was seriously injured or died a horrible death and adding both together produces a result that can squeak by FDA.
There is scope to wonder if something similar happened in this trial.
What we do know is that more people died on vaccine than placebo and lots more people disappeared on vaccine and FDA’s current leadership for whatever reason would prefer to be dead before anyone gets access to the data and their correspondence with Pfizer.
Slide 53
Is there a House in the Doctor? The medical drama House was watched and loved by many. Dr House was good at solving puzzling clinical cases by pulling on the thread of some minor detail which led to the answer.
Doctors today have close to lost the ability to say an evident X causes an evident Y – largely down to the mantra that only RCT evidence tells us what a treatment does and we can’t believe the evident anymore. Wife shoots husband point blank in chest – did she kill him? Who knows. In perhaps 1 case in 100 he had a heart attack just beforehand – we need to pass the 100 cases on to those experts in CDC, FDA, EMA etc and let them work it out.
As a result docs report maybe 1 in 10 or 1 in 100 serious side effects to regulators who file these away and do nothing with them.
This is unlike airline pilots who also report near misses and refuse to fly if these reports are not taken into account – after all if the customer dies the pilot does too. This is not true of doctors.
Slide 54
There is a profound misapprehension of the role of a regulator. They are not part of the health apparatus. Their job , perhaps easier to see in the case of food, is to decide if this yellow stuff is butter or lard colored to look like butter. If butter – it is not their job to decide if this is good butter or not or if butter is good for us or not. Ditto with drugs – the role is just to tick a box if certain criteria are met.
They have no abilities to or training in establishing if a drug or vaccine causes a problem.
Slide 55

Here is Walter Raleigh getting his head chopped off. After the fact legal systems recognized the injustice of convicting someone based on hearsay and said cases could only be decided on the basis of evidence in the room that can examined and cross-examined.
The first thing MHRA do with any reports is to remove the names of doctors and patients. This converts them into hearsay, anedcotes, misinformation. It means no-one can decide if there is a link.
MHRA will say till the crack of doom they are looking to find causal needles in the haystack of reports but faced with a needle-stack they can’t seem to spot a needle.
The key to determining cause and effect is an encounter between a doctor and patient. All the data is there. After a first run through there is a chance to follow up when oddities about the data come to mind. Remove the possibility for an ongoing two-way encounter like this and you remove the ability to establish cause and effect.
Slide 56
The one tool regulators have with anonymized drug reports is proportional reporting rates but as Matthew Crawford pointed out you can’t even use this for VAERS because you need lots of drugs in the mix for this to work properly. Besides proportional reporting rates are a cop-out. They might look more scientific than interviewing someone but they aren’t.
Slide 57

If someone commits suicide on an SSRI, their doctor will be advised by their insurer not to say the drug caused it or say anything that might lead to a further legal case. Insurance is supposed to be a business that supports us to take risks but is not doing this here.
If the doctor breaks ranks and blames the drug, a coroner, who can say a street drug caused a death, has no box to tick to implicate a prescription drug in a death.
Media guidance equally ensures journalists cannot say the obvious – the drug caused the suicide if the coroner hasn’t done so – and all this will apply to vaccines also.
If the coroner goes rogue and writes to the regulator and intimates that the evident cause of death was the drug or vaccine, the regulator will check on what the doctor has said and if the doctor didn’t finger the drug or vaccine – they won’t.
If the case is so Evident that both doctor and coroner go rogue, as in the Alana Cutland case, the regulator will respond, as MHRA did, that we only have a handful of reports like this – not enough to let us work out what might have gone on.
Slide 58
In the TV series House, the hero pays heed to tiny things that don’t fit the pattern and after twists and turns finds how it all hangs together.
When a wife shoots her husband in front of Dr House these days he seems unable to work out what’s gone on. Ok the guy may have had a heart attack at the same time and she shot him afterwards out of spite at being cheated out of a pleasant moment but 99 times out a 100 it’s pretty simple, she killed him. House though has lost this plot.
Some great doctors encourage their colleagues to report adverse events to regulators – which makes the problem worse. Regulators will file these reports away until the crack of doom. Unless doctors have the courage to say – look I know what I have seen and the vaccine or the drug killed my patient, they make things worse.
Dr House can’t get his head around the fact that with drugs and vaccines we hope to bring good out of the use of a poison, and sometimes people get poisoned. We and he prefer the idea he is giving sacraments – things that can only do good.
F Scott Fitzgerald once said that a sophisticated mind can hold two contradictory things in mind at the same time and still function – doctors could do this once but can’t now.
Science challenges Muslims and Jews, Xtians and Atheists to leave their biases at the door and come to a consensus about the data. But as in a jury trial, sticking with the data we still have to come to a verdict. A judgement. A diagnosis. It is not the role of a regulator to make diagnoses or deliver verdicts.
A verdict has effects in the real world just as much as shooting someone. There are evident effects from shooting on a husband who dies, and equally evident effects on the wife being tried.
This is important but more important for all of us just now are the effects on the doctor or failing to make any verdict, and just as much failing to make the diagnosis they know or suspect is the right one.
This failure transforms them into Model Doctors – a shrunken replica of the real thing.
When treating a patient, following the evidence can’t mean doing what ghostwritten fraudulent articles say. It has to mean following the person in front of me and coming to a consensus view just as a jury would.
If there is a mismatch between that and the so-called evidence – well all the books say that’s what moves science forward.
Slide 60
See The Handmaid’s Vaccine on RxISK – and its message about Albert and Ursula, the happy couple you see here.

Vaccines currently are the primary mitigation strategy to combat COVID-19 around the world. For instance, the narrative related to the ongoing surge of new cases in the United States (US) is argued to be driven by areas with low vaccination rates [1]. A similar narrative also has been observed in countries, such as Germany and the United Kingdom [2]. At the same time, Israel that was hailed for its swift and high rates of vaccination has also seen a substantial resurgence in COVID-19 cases [3]. We investigate the relationship between the percentage of population fully vaccinated and new COVID-19 cases across 68 countries and across 2947 counties in the US.
Methods
We used COVID-19 data provided by the Our World in Data for cross-country analysis, available as of September 3, 2021 (Supplementary Table 1) [4]. We included 68 countries that met the following criteria: had second dose vaccine data available; had COVID-19 case data available; had population data available; and the last update of data was within 3 days prior to or on September 3, 2021. For the 7 days preceding September 3, 2021 we computed the COVID-19 cases per 1 million people for each country as well as the percentage of population that is fully vaccinated.
For the county-level analysis in the US, we utilized the White House COVID-19 Team data [5], available as of September 2, 2021 (Supplementary Table 2). We excluded counties that did not report fully vaccinated population percentage data yielding 2947 counties for the analysis. We computed the number and percentages of counties that experienced an increase in COVID-19 cases by levels of the percentage of people fully vaccinated in each county. The percentage increase in COVID-19 cases was calculated based on the difference in cases from the last 7 days and the 7 days preceding them. For example, Los Angeles county in California had 18,171 cases in the last 7 days (August 26 to September 1) and 31,616 cases in the previous 7 days (August 19–25), so this county did not experience an increase of cases in our dataset. We provide a dashboard of the metrics used in this analysis that is updated automatically as new data is made available by the White House COVID-19 Team (https://tiny.cc/USDashboard).
Findings
At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days (Fig. 1). In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people. Notably, Israel with over 60% of their population fully vaccinated had the highest COVID-19 cases per 1 million people in the last 7 days. The lack of a meaningful association between percentage population fully vaccinated and new COVID-19 cases is further exemplified, for instance, by comparison of Iceland and Portugal. Both countries have over 75% of their population fully vaccinated and have more COVID-19 cases per 1 million people than countries such as Vietnam and South Africa that have around 10% of their population fully vaccinated.
Fig. 1

Relationship between cases per 1 million people (last 7 days) and percentage of population fully vaccinated across 68 countries as of September 3, 2021 (See Table S1 for the underlying data)
Across the US counties too, the median new COVID-19 cases per 100,000 people in the last 7 days is largely similar across the categories of percent population fully vaccinated (Fig. 2). Notably there is also substantial county variation in new COVID-19 cases within categories of percentage population fully vaccinated. There also appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated (Fig. 3).
Fig. 2

Median, interquartile range and variation in cases per 100,000 people in the last 7 days across percentage of population fully vaccinated as of September 2, 2021
Fig. 3

Percentage of counties that experienced an increase of cases between two consecutive 7-day time periods by percentage of population fully vaccinated across 2947 counties as of September 2, 2021
Of the top 5 counties that have the highest percentage of population fully vaccinated (99.9–84.3%), the US Centers for Disease Control and Prevention (CDC) identifies 4 of them as “High” Transmission counties. Chattahoochee (Georgia), McKinley (New Mexico), and Arecibo (Puerto Rico) counties have above 90% of their population fully vaccinated with all three being classified as “High” transmission. Conversely, of the 57 counties that have been classified as “low” transmission counties by the CDC, 26.3% (15) have percentage of population fully vaccinated below 20%.
Since full immunity from the vaccine is believed to take about 2 weeks after the second dose, we conducted sensitivity analyses by using a 1-month lag on the percentage population fully vaccinated for countries and US counties. The above findings of no discernable association between COVID-19 cases and levels of fully vaccinated was also observed when we considered a 1-month lag on the levels of fully vaccinated (Supplementary Figure 1, Supplementary Figure 2).
We should note that the COVID-19 case data is of confirmed cases, which is a function of both supply (e.g., variation in testing capacities or reporting practices) and demand-side (e.g., variation in people’s decision on when to get tested) factors.
Interpretation
The sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences needs to be re-examined, especially considering the Delta (B.1.617.2) variant and the likelihood of future variants. Other pharmacological and non-pharmacological interventions may need to be put in place alongside increasing vaccination rates. Such course correction, especially with regards to the policy narrative, becomes paramount with emerging scientific evidence on real world effectiveness of the vaccines.
For instance, in a report released from the Ministry of Health in Israel, the effectiveness of 2 doses of the BNT162b2 (Pfizer-BioNTech) vaccine against preventing COVID-19 infection was reported to be 39% [6], substantially lower than the trial efficacy of 96% [7]. It is also emerging that immunity derived from the Pfizer-BioNTech vaccine may not be as strong as immunity acquired through recovery from the COVID-19 virus [8]. A substantial decline in immunity from mRNA vaccines 6-months post immunization has also been reported [9]. Even though vaccinations offers protection to individuals against severe hospitalization and death, the CDC reported an increase from 0.01 to 9% and 0 to 15.1% (between January to May 2021) in the rates of hospitalizations and deaths, respectively, amongst the fully vaccinated [10].
In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect. Stigmatizing populations can do more harm than good. Importantly, other non-pharmacological prevention efforts (e.g., the importance of basic public health hygiene with regards to maintaining safe distance or handwashing, promoting better frequent and cheaper forms of testing) needs to be renewed in order to strike the balance of learning to live with COVID-19 in the same manner we continue to live a 100 years later with various seasonal alterations of the 1918 Influenza virus.

Unlimited Hangout — On Wednesday, an “industry-led and UN-convened” alliance of private banking and financial institutions announced plans at the COP26 conference to overhaul the role of global and regional financial institutions, including the World Bank and IMF, as part of a broader plan to “transform” the global financial system. The officially stated purpose of this proposed overhaul, per alliance members, is to promote the transition to a “net zero” economy. However, the group’s proposed “reimagining” of international financial institutions, according to their recently published “progress report,” would also move to merge these institutions with the private-banking interests that compose the alliance; create a new system of “global financial governance”; and erode national sovereignty among developing countries by forcing them to establish business environments deemed “friendly” to the interests of alliance members. In other words, the powerful banking interests that compose this group are pushing to recreate the entire global financial system for their benefit under the guise of promoting sustainability.
This alliance, called the Glasgow Financial Alliance for Net Zero (GFANZ), was launched in April by John Kerry, US Special Presidential Envoy for Climate Change; Janet Yellen, US Secretary of the Treasury and former chair of the Federal Reserve; and Mark Carney, UN Special Envoy for Climate Action and Finance and former chair of the Bank of England and Bank of Canada. Carney, who is also the UK prime minister’s Finance Advisor for the COP26 conference, currently cochairs the alliance with US billionaire and former mayor of New York City, Michael Bloomberg.
![]()

GFANZ Leadership; Source: GFANZ
On its creation, GFANZ stated that it would “provide a forum for strategic coordination among the leadership of finance institutions from across the finance sector to accelerate the transition to a net zero economy” and “mobilize the trillions of dollars necessary” to accomplish the group’s zero emissions goals. At the time of the alliance’s launch, UK prime minister Boris Johnson described GFANZ as “uniting the world’s banks and financial institutions behind the global transition to net zero,” while John Kerry noted that “the largest financial players in the world recognize energy transition represents a vast commercial opportunity.” In analyzing those two statements together, it seems clear that GFANZ has united the world’s most powerful private banks and financial institutions behind what it sees, first and foremost, as “a vast commercial opportunity,” the exploitation of which it is marketing as a “planetary imperative.”
![]()

John Kerry in conversation with CNN’s Christine Amanpour at COP 26. Source: CNN
GFANZ is composed of several “subsector alliances,” including the Net Zero Asset Managers Initiative (NZAM), the Net Zero Asset Owner Alliance (NZAOA), and the Net Zero Banking Alliance (NZBA). Together, they command a formidable part of global private banking and finance interests, with the NZBA alone currently representing 43 percent of all global banking assets. However, the “largest financial players” who dominate GFANZ include the CEOs of BlackRock, Citi, Bank of America, Banco Santander, and HSBC, as well as David Schwimmer, CEO of the London Stock Exchange Group and Nili Gilbert, chair of the Investment Committee of the David Rockefeller Fund.
Notably, another Rockefeller-connected entity, the Rockefeller Foundation, recently played a pivotal role in the creation of Natural Asset Corporations (NACs) in September. These NACs seek to create a new asset class that would put the natural world, as well as the ecological processes that underpin all life, up for sale under the guise of “protecting” them. Principals of GFANZ, including BlackRock’s Larry Fink, have long been enthusiastic about the prospects of NACs and other related efforts to financialize the natural world and he has also played a key role in marketing such financialization as necessary to combat climate change.
As part of COP26, GFANZ— a key group at that conference—is publishing a plan aimed at scaling “private capital flows to emerging and developing economies.” Per the alliance’s press release, this plan focuses on “the development of country platforms to connect the now enormous private capital committed to net zero with country projects, scaling blended finance through MDBs [multilateral development banks] and developing high integrity, credible global carbon markets.” The press release notes that this “enormous private capital” is money that alliance members seek to invest in emerging and developing countries, estimated at over $130 trillion, and that—in order to deploy these trillions in investment—“the global financial system is being transformed” by this very alliance in coordination with the group that convened them, the United Nations.
Proposing a Takeover
Details of GFANZ’s plan to deploy trillions of member investments into emerging markets and developing countries was published in the alliance’s inaugural “Progress Report,” the release of which was timed to coincide with the COP26 conference. The report details the alliance’s “near-term work plan and ambitions,” which the alliance succinctly summarizes as a “program of work to transform the financial system.”
The report notes that the alliance has moved from the “commitment” stage to the “engagement” stage, with the main focus of the engagement stage being the “mobilization of private capital into emerging markets and developing countries through private-sector leadership and public-private collaboration.” In doing so, per the report, GFANZ seeks to create “an international financial architecture” that will increase levels of private investment from alliance members in those economies. Their main objectives in this regard revolve around the creation of “ambitious country platforms” and increased collaboration between MDBs and the private financial sector.
Per GFANZ, a “country platform” is defined as a mechanism that convenes and aligns “stakeholders,” that is, a mechanism for public-private partnership/stakeholder capitalism, “around a specific issue or geography.” Examples offered include Mike Bloomberg’s Climate Finance Leadership Initiative (CFLI), which is partnered with Goldman Sachs and HSBC among other private-sector institutions. While framed as being driven by “stakeholders,” existing examples of “country platforms” offered by the GFANZ are either private sector-led initiatives, like the CFLI, or public-private partnerships that are dominated by powerful multinational corporations and billionaires. As recently explained by journalist and researcher Iain Davis, these “stakeholder capitalism” mechanism models, despite being presented as offering a “more responsible” form of capitalism, allow corporations and private entities to participate in forming the regulations that govern their own markets and giving them a greatly increased role in political decision making by placing them on an equal footing with national governments. It is essentially a creative way of marketing “corporatism,” the definition of fascism infamously supplied by Italian dictator Benito Mussolini.
In addition to the creation of “corporatist” “country platforms” that focus on specific areas and/or issues in the developing world, GFANZ aims to also further “corporatize” multilateral development banks (MDBs) and development finance institutions (DFIs) in order to better fulfill the investment goals of alliance members. Per the alliance, this is described as increasing “MDB-private sector collaboration.” The GFANZ report notes that “MDBs play a critical role in helping to grow investment flows” in the developing world. MDBs, like the World Bank, have long been criticized for accomplishing this task by trapping developing nations in debt and then using that debt to force those nations to deregulate markets (specifically financial markets), privatize state assets and implement unpopular austerity policies. The GFANZ report makes it clear that the alliance now seeks to use these same, controversial tactics of MDBs by forcing even greater deregulation on developing countries to facilitate “green” investments from alliance members.
The report explicitly states that MDBs should be used to prompt developing nations “to create the right high-level, cross-cutting enabling environments” for alliance members’ investments in those nations. The significantly greater levels of private-capital investment, which are needed to reach net zero per GFANZ, require that MDBs are used to prompt developing nations to “establish investment-friendly business environments; a replicable framework for deploying private capital investments; and pipelines of bankable investment opportunities.” GFANZ then notes that “private capital and investment will flow to these projects if governments and policymakers create the appropriate conditions,” that is, enable environments for private-sector investments.
In other words, through the proposed increase in private-sector involvement in MDBs, such as the World Bank and regional development banks, alliance members seek to use MDBs to globally impose massive and extensive deregulation on developing countries by using the decarbonization push as justification. No longer must MDBs entrap developing nations in debt to force policies that benefit foreign and multinational private-sector entities, as climate change-related justifications can now be used for the same ends.
![]()
BlackRock CEO and GFANZ principal Larry Fink talks to CNBC during COP26. Source: CNBC
This new modality for MDBs, along with their fusion with the private sector, is ultimately what GFANZ proposes in terms of “reimagining” these institutions. GFANZ principal and BlackRock CEO Larry Fink, during a COP26 panel that took place on November 2, explicitly referred to the plan to overhaul these institutions when he said: “If we’re going to be serious about climate change in the emerging world, we’re going to have to really focus on the reimagination of the World Bank and the IMF.”
Fink continued:
They are the senior lender, and not enough private capital’s coming into the emerging world today because of the risks associated with the political risk, investing in brownfield investments — if we are serious about elevating investment capital in the emerging world. . . . I’m urging the owners of those institutions, the equity owners, to focus on how we reimagine these institutions and rethink their charter.
GFANZ’s proposed plans to reimagine MDBs are particularly alarming given how leaked US military documents show that such banks are considered to be essentially “financial weapons” that have been used as “financial instruments and diplomatic instruments of US national power” as well as instruments of what those same documents refer to as the “current global governance system” that are used to force developing countries to adopt policies they otherwise would not.
In addition, given Fink’s statements, it should not be surprising that the GFANZ report notes that their effort to establish “country platforms” and alter the functioning and charters of MDBs is a key component of implementing preplanned recommendations aimed at “seizing the New Bretton Woods moment” and remaking the “global financial governance” system so that it “promote[s] economic stability and sustainable growth.”
As noted in other GFANZ documents and on their website, the goal of the alliance is the transformation of the global financial system, and it is obvious from member statements and alliance documents that the goal of that transformation is to facilitate the investment goals of alliance members beyond what is currently possible by using climate change-related dictates, rather than debt, as the means to that end.
The UN and the “Quiet Revolution”
In light of GFANZ’s membership and members’ ambitions, some may wonder why the United Nations would back such a predatory initiative. Doesn’t the United Nations, after all, chiefly work with national governments as opposed to private-sector interests?
Though that is certainly the prevailing public perception of the UN, the organization has for decades been following a “stakeholder capitalist” model that privileges the private sector and billionaire “philanthropists” over national governments, with the latter merely being tasked with creating “enabling environments” for the policies created by and for the benefit of the former.
Speaking to the World Economic Forum in 1998, Secretary General Kofi Annan made this shift explicit:
The United Nations has been transformed since we last met here in Davos. The Organization has undergone a complete overhaul that I have described as a ‘quiet revolution.” . . . A fundamental shift has occurred. The United Nations once dealt only with governments. By now we know that peace and prosperity cannot be achieved without partnerships involving governments, international organizations, the business community and civil society. . . . The business of the United Nations involves the businesses of the world.
With the UN now essentially a vehicle for the promotion of stakeholder capitalism, it is only fitting that it would “convene” and support the efforts of a group like GFANZ to extend that stakeholder capitalist model to other institutions involved in global governance, specifically global financial governance. Allowing GFANZ members, that is, many of the largest private banks and financial institutions in the world, to fuse with MDBs, remake the “global financial governance system,” and gain increased control over political decisions in the emerging world is a banker’s dream come true. To get this far, all they have needed to do was to convince enough of the world’s population that such shifts are necessary due to the perceived urgency of climate change and the need to rapidly decarbonize the economy. Yet, if put into practice, what will result is hardly a “greener” world but a world dominated by a small financial and technocratic elite who are free to profit and pillage from both “natural capital” and “human capital.”
Today, MDBs are used as “instruments of power” that utilize debt to force developing nations to implement policies that benefit foreign interests rather than their own national interests. If GFANZ gets its way, the MDBs of tomorrow will be used to essentially eliminate national sovereignty, privatize the “natural assets” (e.g., ecosystems, ecological processes) of the developing world, and force increasingly technocratic policies designed by global governance institutions and think tanks on ever more disenfranchised populations.
Though GFANZ has cloaked itself in lofty rhetoric of “saving the planet,” its plans ultimately amount to a corporate-led coup that will make the global financial system even more corrupt and predatory and further reduce the sovereignty of national governments in the developing world.
Feature photo | Former governor of the Bank of England Mark Carney, who is the U.N.’s special envoy for climate change, speaks at a Bank of England Financial Stability Report Press Conference, in London, Dec. 16, 2019. Kirsty Wigglesworth | AP
Whitney Webb has been a professional writer, researcher and journalist since 2016. She has written for several websites and, from 2017 to 2020, was a staff writer and senior investigative reporter for MintPress News. She currently writes for her own outlet Unlimited Hangout and contributes to The Last American Vagabond and MintPress News.

The first principle of non-violent action is that of non-cooperation with everything humiliating.
– Mohandas K. Gandhi
I once read an account of bullying in rural America in the early 20th century. The narrator said, “If a victim did not stand up to them, there was no limit to how far the bullies would go.” He described them tying another child to the train tracks as a train approached (on the parallel track). There was no appeasing the bullies. Each capitulation only whetted their appetite for new and crueler humiliations.
The psychology of bullies is well understood: compensation for a loss of power, reenactment of trauma with roles reversed, and so forth. Beyond all that, though, the Bully archetype draws from another source. On some unconscious level, what the bully wants is for the victim to cease being a victim and to stand up to him. That is why submission does not appease a bully, but only invites further torment.
There is an initiatory possibility in the abuser-victim relationship. In that relationship and perhaps beyond it, the victim seeks to control the world through submissiveness. If I am submissive enough, pitiable enough, the abuser may finally relent. Other people might step in (the Rescuer archetype). There is nothing intrinsically wrong with submission or what improvisational theater pioneer Keith Johnstone called a low-status play. There are indeed some situations when doing that is necessary to survive. However, when the submissive posture becomes a habit and the victim loses touch with her capability and strength, the initiatory potential of the situation emerges. The bully or abuser intensifies the abuse until the victim reaches a point where the situation is so intolerable that she throws habit and caution to the wind. She discovers a capacity within her that she did not know she had. She becomes someone new and greater than she had been. That is a pretty good definition of an initiation.
When that happens, when the victim stands his ground and fights back, quite often the bully leaves him alone. On the soul level, his work is done. The initiation is complete. Of course, one might also say that the bully is a coward who wants only submissive victims. Or one might say that resistance spoils the sought-after psychodrama of dominance and submission. There is no guarantee that the resistance will be successful, but even if it is not, the dynamics of the relationship change when the victim decides she is through being a victim. She may discover that a lot of the power the bully had was in her fear and not in his actual physical control.
Until that shift happens, even if a rescuer intervenes, the situation is unlikely to change. Either the intervention will fail, or the rescuer will become a new abuser. The world will ask again and again whether the victim is ready to take a stand.
Please do not interpret this as a cavalier suggestion to someone in an abusive relationship to simply “take a stand.” That is easier said than done, and especially easy to say in ignorance of just what sort of courage would be required. In some situations, especially when children are involved, there is no way to resist without horrible risk to oneself or innocent others. Yet even in the most hopeless situations, the victim often learns a certain strength that she didn’t know she had. Because submission often leads to further, intensifying violation, eventually she will reach her breaking point where courage is born. In that moment, freedom from the abuser is more important than life itself.
The relationship between our governing authorities and the public today bears many similarities to the abuser-victim dynamic. Facing a bully, it is futile to hope that the bully will relent if you don’t resist. Acquiescence invites further humiliation. Similarly, it is wishful thinking to hope that the authorities will simply hand back the powers they have seized over the course of the pandemic. Indeed, if our rights and freedoms exist only by the whim of those authorities, conditional on their decision to grant them, then they are not rights and freedoms at all, but only privileges. By its nature, freedom is not something one can beg for; the posture of begging already grants the power relations of subjugation. The victim can beg the bully to relent, and maybe he will—temporarily—satisfied that the relation of dominance has been affirmed. The victim is still not free of the bully.
That is why I feel impatient when someone speaks of “When the pandemic is over” or “When we are able to travel again” or “When we are able to have festivals again.” None of these things will happen by themselves. Compared to past pandemics, Covid is more a social-political phenomenon than it is an actual deadly disease. Yes, people are dying, but even assuming that everyone in the official numbers died “of” and not “with” Covid, casualties number one-third to one-ninth those of the 1918 flu; per-capita it is one-twelfth to one-thirty-sixth.1 As a sociopolitical phenomenon, there is no guaranteed end to it. Nature will not end it, at any rate; it will end only through the agreement of human beings that it has ended.2 This has become abundantly clear with the Omicron Variant. Political leaders, public health officials, and the media are whipping up fear and reinstituting policies that would have been unthinkable a few years ago for a disease that, at the present writing, has killed one person globally. So, we cannot speak of the pandemic ever being over unless we the people declare it to be over.
Of course, I could be wrong here. Perhaps Omicron is, as World Medical Association chairman Frank Ulrich Montgomery has warned, as dangerous as Ebola. Regardless, the question remains: will we allow ourselves to be held forever hostage to the possibility of an epidemic disease? That possibility will never disappear.
Another thing I’ve been hearing a lot of recently is that “Covid tyranny is bound to end soon, because people just aren’t going to stand for it much longer.” It would be more accurate to say, “Covid tyranny will continue until people no longer stand for it.” That brings up the question, “Am I standing for it?” Or am I waiting for other people to end it for me, so that I don’t have to? In other words, am I waiting for the rescuer, so that I needn’t take the risk of standing up to the bully?
If you do put up with it, waiting for others to resist instead, then you affirm a general principle of “waiting for others to do it.” Having affirmed that principle, the forlorn hope that others will resist rings hollow. Why should I believe others will do what I’m unwilling to do? That is why pronouncements about the inevitability of a return to normalcy, though they seem hopeful, carry an aura of delusion and despair.
In fact, there is no obvious limit to what people will put up with, just as there is no limit to what an abusive power will do to them.
If the end of Covid bullying is not an inevitability, then what is it? It is a choice. It is precisely the initiatory moment in which the victim—that is, the public—discovers its power. At the very beginning of the pandemic I called it a coronation: an initiation into sovereignty. Covid has shown us a future toward which we have long been hurtling, a future of technologically mediated relationships, ubiquitous surveillance, big tech information control, obsession with safety, shrinking civil liberties, widening wealth inequality, and the medicalization of life. All these trends predate Covid. Now we see in sharp relief where we have been headed. Is this what we want? An automatic inertial trend has become conscious, available for choice. But to choose something else, we must wrest control away from the institutions administering the current system. That requires a restoration of real democracy; i.e., popular sovereignty, in which we no longer passively accept as inevitable the agendas of established authority, and in which we no longer beg for privileges disguised as freedoms.
Despite appearances, Covid has not been the end of democracy. It has merely revealed that we were already not in a democracy. It showed where the power really is and how easily the facade of freedom could be stripped from us. It showed that we were “free” only at the pleasure of elite institutions. By our ready acquiescence, it showed us something about ourselves.
We were already unfree. We were already conditioned to submission.
In Orwell’s 1984, Winston’s interrogator O’Brien states: “The more the Party is powerful, the less it will be tolerant: the weaker the opposition, the tighter the despotism.” The Covid era has seen endless indignities, humiliations, and abuse heaped upon the public, each more outrageous than the last. It is as if someone is performing a psychological experiment to see how much people are willing to take. Let’s tell them that masks don’t work, and then reverse it and require them to mask up. Let’s tell them they can’t shake hands. Let’s tell them they can’t go near each other. Let’s shut down their churches, choirs, businesses, and festivals. Let’s stop them from gathering for the holidays. Let’s make them inject poison into their bodies. Let’s make them do it again. Let’s make them do it to their children. Let’s censor their first-hand stories as “false information.” Let’s feed them obvious absurdities to see what they’ll swallow. Let’s make promises and break them. Let’s make the same promises again and break them again. Let’s require authorization for their every movement. Wow, they’re still going along with it? Let’s see how much more they will take.
I have written the above as if the bullying powers were a bunch of cackling sadists delighting in the humiliation of their victims. That is not accurate. Most people staffing our governing institution are normal, decent human beings. While it is also true that these institutions are hospitable environments for martinets, control freaks, and sadists, more often they turn people into martinets, control freaks, and sadists. These individuals are more symptom than cause of the generalized abuse of the public today. They are functionaries, playing the roles that a systemically abusive drama requires. Causing suffering is not their root motivation, it is to establish control. The quest for power doubtless finds justification in the idea that it is all for the greater good. Yes, they think, it would be bad if evil people were in charge of the surveillance, censorship, and coercive apparatus, but fortunately it is we, the rational, intelligent, far-seeing, science-based good guys who are at the helm.
Through the absolute conviction by those who hold power that they are the good guys, power transforms from a means to an end. As maybe it was to begin with—Orwell dispels the false justifications of power when he has O’Brien say:
The Party seeks power entirely for its own sake. We are not interested in the good of others; we are interested solely in power. Not wealth or luxury or long life or happiness: only power, pure power. What pure power means you will understand presently. We are different from all the oligarchies of the past, in that we know what we are doing. All the others, even those who resembled ourselves, were cowards and hypocrites. The German Nazis and the Russian Communists came very close to us in their methods, but they never had the courage to recognize their own motives. They pretended, perhaps they even believed, that they had seized power unwillingly and for a limited time, and that just round the corner there lay a paradise where human beings would be free and equal. We are not like that. We know that no one ever seizes power with the intention of relinquishing it. Power is not a means, it is an end. One does not establish a dictatorship in order to safeguard a revolution; one makes the revolution in order to establish the dictatorship. The object of persecution is persecution. The object of torture is torture. The object of power is power. Now do you begin to understand me?'
The theme resumes on the next page:
He paused, and for a moment assumed again his air of a schoolmaster questioning a promising pupil: 'How does one man assert his power over another, Winston?'
Winston thought. 'By making him suffer,' he said.
'Exactly. By making him suffer. Obedience is not enough. Unless he is suffering, how can you be sure that he is obeying your will and not his own? Power is in inflicting pain and humiliation. Power is in tearing human minds to pieces and putting them together again in new shapes of your own choosing. Do you begin to see, then, what kind of world we are creating?
Thus it is that the privation, humiliation, and suffering of those they dominate is pleasing to the controllers. It isn’t suffering per se that pleases them. They may even consider it a regrettable necessity. It pleases them as a hallmark of submission.
Covid-era policies cannot be understood merely through the lens of public health. In an earlier series of essays I explored them from the perspective of sacrificial violence, mob morality, dehumanization, and the exploitation of these by fascistic forces. Equally important is the perspective of power. Seeing Covid through the lens of rational public health, of course we should expect the “end of the pandemic” quite soon. Seeing through the lens of power, we cannot be so sanguine, any more than the bullied child can hope the bully will stop because, after all, I’ve done everything he told me to.
The bully doesn’t want the victim to do X, Y, and Z for their own sake. He wants to establish the principle that the victim will do X, Y, Z, or A, B, or C, on demand. That’s why arbitrary, unreasonable, ever-shifting demands are characteristic of an abusive relationship. The more irrational the demand, the better. The controllers find it satisfying to see everyone dutifully wearing their masks. As with O’Brien, it is power, not actual public safety, that inspires them. That is why they roundly ignore science casting doubt on masks, lockdowns, and social distancing. Effectiveness was never the root motivation for those policies to begin with.
I learned about this too in school. In the senseless, degrading busy work and the arbitrary rules, I detected a hidden curriculum: a curriculum of submission.3 The principal issued a series of trivial rules under the pretext of “maintaining a positive learning environment.” Neither the students nor the administration actually believed that wearing hats or chewing gum impeded learning, but that didn’t matter. Punishments were not actually for the infraction itself; the real infraction was disobedience. That is the chief crime in a dominance/submission relationship. Thus, when German police patrol the square with meter sticks to enforce social distancing, no one need believe that the enforcement will actually stop anyone from getting sick. The offense they are patrolling against is disobedience. Disobedience is indeed offensive to the abusive party, and to anyone who fully accepts a submissive role in relation to it. When “Karens” report on their neighbors for having more than the permitted number of guests, is it a civic-minded desire to slow the spread that motivates them? Or are they offended that someone is breaking the rules?
It is uncomfortable for those who have knuckled under to a bully to see someone else stand up to him. It disrupts the idea of powerlessness and the role, which may have become perversely comfortable, of the victim. It invokes the initiatory moment by making an unconscious choice conscious: “I could do that too.” To resist the abuser asks others if they will resist too. It is far from inevitable that they will accept the invitation, yet the example of courage is more powerful than any exhortation.
Today a wave of resistance to Covid policies is surging across the globe. You’ll see little mention of it in mainstream media, but thousands and tens of thousands are protesting all across Europe, Thailand, Japan, Australia, North America… pretty much anywhere that lockdowns and vaccine mandates have been applied. People are risking arrest to defy lockdowns and curfews. They are walking out of jobs, losing licenses, enduring forced closures of their businesses, sometimes even losing custody of their children because they refuse to comply with vaccine mandates. They are getting kicked off social media for speaking out. They are sacrificing concerts, sports, skiing, travel, college, careers, and livelihoods. Under compulsory vaccination laws In Austria, they will soon risk prison.
Some people have much more to lose than others by speaking out, refusing vaccination, or engaging in civil disobedience. As someone who has relatively little to lose, it is not my job to demand other people be brave. It isn’t anyone’s job. We can, though, describe the reality of the situation. That fosters bravery, because it isn’t only external fear, force, and threat that breeds submission. In an abusive relationship the victim often adopts some of the abuser’s narrative: I am weak. I am contemptible. I am powerless. You are right. I am wrong. I need you. I deserve this. I am crazy. This is normal. This is OK.
When the victim internalizes the abuser, I say that the bandits have breached the castle walls. I know well what it is like to be a fugitive in my own castle, dodging the patrolling invaders to protect my secret sanity.
My understanding of the bullying victim comes from direct experience. I was among the youngest in my grade and reached puberty quite late. At age 12 I was a scrawny 4’10”, 90-pound weakling among the hulking adolescents of my former friend group. Their cruel jokes and torments were mostly not intended to cause physical pain, but rather to assert dominance and humiliate. Fighting back was not much of an option—the ringleader was literally twice my weight. When I tried to fight back, the gang looked at each other with amusement. “Uh oh,” they said, “Chucky’s getting mad! Did your daddy tell you to stand up to us, Chucky?” The next thing I knew, I was on the floor in a submission hold, surrounded by a chorus of mocking laughter. That was what happened when I resisted. Yet submission didn’t work either; it appeased them for a day or perhaps a few minutes or not at all. It was an invitation to further violence. In this difficult situation, I internalized the abusers by taking on their opinion of myself as pathetic and contemptible.4
In this case, literally fighting back was futile. My initiatory journey took the form of stepping into the unknown of finding new friends—a frightening prospect in the cacophony and chaos of the junior high cafeteria. Exiting the role of victim doesn’t usually mean physical combat or legal combat, though it might. Invariably, it means refusing to comply with violation or humiliation. In real life it could be blocking a caller, getting a restraining order, or simply running away. It cannot be a mere gesture. It must be determined and sustained until the old role no longer beckons.
It is worth noting that none of my abusers were particularly bad people. Nor were those who joined in the laughter, nor those who stood by in disapproving silence. They went on to become solid contributing members of society, good fathers and husbands. There was something in the confluence of our biographies that called them to the role of abuser, enabler, or bystander at that moment. The abuser-victim drama issues a powerful casting call. An abusive spouse may no longer occupy that role in a subsequent marriage. The roles allow each actor to discover—and possibly integrate and transcend—something in themselves. So it is society-wide as well. What will the functionaries of our abusive, degrading, oppressive system become when the drama ends? Already a lot of them are getting sick of their roles. The victim does the abuser no favor by prolonging the drama.
Earlier I wrote that often, the point of courage comes when the pain of submission grows intolerable. The erstwhile victim reaches a breaking point and throws caution to the wind. The abuser may still wield the outward apparatus of power, but no longer does that power have an ally within the victim, who becomes ungovernable. A lot of people are reaching that breaking point now. Powering the aforementioned wave of resistance is a hurricane of fury brewing just offshore of official reality. If you want to get a sense of it, subscribe to the Telegram channel “They Say Its Rare.” It displays without comment Tweets from vaccine-harmed individuals and their friends and families. Thousands upon thousands of Tweets, raw, outraged, and indignant. Most of these people will never comply with vaccination again no matter what the pressure, nor will many of their friends. Perhaps this partly explains low public uptake of boosters. (That and the fact that the first two shots did not deliver the promised rewards of immunity or freedom.)
The drama continues. The bully does not relent at the first sign of resistance. On the soul level, the bully serves his purpose only when he provokes real, sustained courage. As resistance grows, so grows the coercion. We are very nearly at a tipping point. The scale is evenly balanced—so finely, perhaps, that the weight of one person may tip it. Could that person be you? Whatever reasons you have to comply, to stay silent, to keep your head down—and they may be very good reasons indeed—please do not accept the insidious false hope that someone else will take the risk if you do not.
What can one person do? Will it matter if I resist, if too many others do not? Five percent of the population can be locked up, locked in, or locked out of society. Forty percent cannot. Will you resist and risk being one of the five percent? Safer to wait and see, isn’t it. Safer to wait until after critical mass has been reached, and join the winning side.
Of all the lies of a controlling power, the key lie is the powerlessness of its victim. That lie is a form of sorcery, coming true to the extent it is believed. All modern people live within a pervasive metaphysical version of that lie. In a Newtonian universe of deterministic forces, indeed it matters little what one person does. It is wholly irrational for the discrete and separate self to be brave, to defy the mob, or to stand up to power. Sure, if lots of people do it, things will change, but you aren’t lots of people, you are just one person. So why not let other people do it? Your choice won’t much affect theirs.
To refute that logic with logic would require a metaphysical treatise that reclaims self and causality from their Cartesian prison. So I won’t use logic. Instead I’ll appeal to Logos—the fiery logic of the heart. Something in you knows that your private struggles and the choices of just-one-person are significant. Furthermore, something in you knows when the time has come to make the choice, to be brave. You can feel the approach of the breaking point. It may feel like, “I’ve had enough. Enough!” It may be a calm clarity. It may be a leap in the dark. Probably you recognize the moment I’m describing; most of us have gone through some life initiation of this kind, bursting out of a cocoon of fear. In that moment you know something significant has happened. The world looks different. That is because it is different.
An abuser, whether a person or a system, offers an opportunity to graduate to a new degree of sovereignty. We claim by example what a human being is. When made at risk, such a claim issues forth as a prayer. An intelligence beyond rational understanding responds to that prayer, and reorganizes the world around it. We may experience this as synchronicity, which seems to happen with uncanny frequency just at those moments where one takes a leap in the dark. She leaves the abusive spouse in the dead of night with nowhere to go. Yet she is not reckless, because she knows It is time. She steps out into nothingness and Lo! Something meets her foot. A path invisible from the starting point opens with each step along it.
So it shall be. The world will rearrange itself around the brave choices millions of people are making as they trust the knowledge, It is time. If you join us, you will be witness to a most marvelous paradox. The transition to a more beautiful world is a mass awakening into sovereignty, far beyond the doing of any hero, any leader, any individual. Yet you will know that it was you—your choice!—that was the fulcrum of the turning of the age.
Abstract
Our group has been using the PULS Cardiac Test (GD Biosciences, Inc, Irvine, CA) a clinically validated measurement of multiple protein biomarkers which generates a score predicting the 5 yr risk (percentage chance) of a new Acute Coronary Syndrome (ACS). The score is based on changes from the norm of multiple protein biomarkers including IL-16, a proinflammatory cytokine, soluble Fas, an inducer of apoptosis, and Hepatocyte Growth Factor (HGF)which serves as a marker for chemotaxis of T-cells into epithelium and cardiac tissue, among other markers. Elevation above the norm increases the PULS score, while decreases below the norm lowers the PULS score.The score has been measured every 3-6 months in our patient population for 8 years.
Recently, with the advent of the mRNA COVID 19 vaccines (vac) by Moderna and Pfizer, dramatic changes in the PULS score became apparent in most patients.This report summarizes those results.
A total of 566 pts, aged 28 to 97, M:F ratio 1:1 seen in a preventive cardiology practice had a new PULS test drawn from 2 to 10 weeks following the 2nd COVID shot and was compared to the previous PULS score drawn 3 to 5 months previously pre- shot. Baseline IL-16 increased from 35=/-20 above the norm to 82 =/- 75 above the norm post-vac; sFas increased from 22+/- 15 above the norm to 46=/-24 above the norm post-vac; HGF increased from 42+/-12 above the norm to 86+/-31 above the norm post-vac. These changes resulted in an increase of the PULS score from 11% 5 yr ACS risk to 25% 5 yr ACS risk.
At the time of this report, these changes persist for at least 2.5 months post second dose of vac.We conclude that the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.

Note: Kaiser Permanente study done for CDC. Data is unavailable. Suggests Vaccinated persons have up to 70% lower mortality (excluding Covid-19) than unvaccinated. Speculates on on why. Leaves impression that Covid Vaccines are elixirs of life.
On October 22, 2021, this report was posted online as an MMWR Early Release.
Stanley Xu, PhD1; Runxin Huang, MS1; Lina S. Sy, MPH1; Sungching C. Glenn, MS1; Denison S. Ryan, MPH1; Kerresa Morrissette, MPH1; David K. Shay, MD2; Gabriela Vazquez-Benitez, PhD3; Jason M. Glanz, PhD4; Nicola P. Klein, MD, PhD5; David McClure, PhD6; Elizabeth G. Liles, MD7; Eric S. Weintraub, MPH8; Hung-Fu Tseng, MPH, PhD1; Lei Qian, PhD1 (View author affiliations)
Summary
What is already known about this topic?
Although deaths after COVID-19 vaccination have been reported to the Vaccine Adverse Events Reporting System, few studies have been conducted to evaluate mortality not associated with COVID-19 among vaccinated and unvaccinated groups.
What is added by this report?
During December 2020–July 2021, COVID-19 vaccine recipients had lower rates of non–COVID-19 mortality than did unvaccinated persons after adjusting for age, sex, race and ethnicity, and study site.
What are the implications for public health practice?
There is no increased risk for mortality among COVID-19 vaccine recipients. This finding reinforces the safety profile of currently approved COVID-19 vaccines in the United States. All persons aged ≥12 years should receive a COVID-19 vaccine.
Related Materials

By September 21, 2021, an estimated 182 million persons in the United States were fully vaccinated against COVID-19.* Clinical trials indicate that Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273), and Janssen (Johnson & Johnson; Ad.26.COV2.S) vaccines are effective and generally well tolerated (1–3). However, daily vaccination rates have declined approximately 78% since April 13, 2021†; vaccine safety concerns have contributed to vaccine hesitancy (4). A cohort study of 19,625 nursing home residents found that those who received an mRNA vaccine (Pfizer-BioNTech or Moderna) had lower all-cause mortality than did unvaccinated residents (5), but no studies comparing mortality rates within the general population of vaccinated and unvaccinated persons have been conducted. To assess mortality not associated with COVID-19 (non–COVID-19 mortality) after COVID-19 vaccination in a general population setting, a cohort study was conducted during December 2020–July 2021 among approximately 11 million persons enrolled in seven Vaccine Safety Datalink (VSD) sites.§ After standardizing mortality rates by age and sex, this study found that COVID-19 vaccine recipients had lower non–COVID-19 mortality than did unvaccinated persons. After adjusting for demographic characteristics and VSD site, this study found that adjusted relative risk (aRR) of non–COVID-19 mortality for the Pfizer-BioNTech vaccine was 0.41 (95% confidence interval [CI] = 0.38–0.44) after dose 1 and 0.34 (95% CI = 0.33–0.36) after dose 2. The aRRs of non–COVID-19 mortality for the Moderna vaccine were 0.34 (95% CI = 0.32–0.37) after dose 1 and 0.31 (95% CI = 0.30–0.33) after dose 2. The aRR after receipt of the Janssen vaccine was 0.54 (95% CI = 0.49–0.59). There is no increased risk for mortality among COVID-19 vaccine recipients. This finding reinforces the safety profile of currently approved COVID-19 vaccines in the United States.
VSD, a collaborative project between CDC’s Immunization Safety Office and nine health care organizations, collects electronic health data, including information on vaccines, for specific studies. In this cohort study of VSD members aged ≥12 years, vaccination status through May 31, 2021 was determined. Index dates were assigned to all persons on the basis of the distribution of vaccination dates among vaccinated persons.¶ Person-time for unvaccinated persons included unvaccinated person-time before COVID-19 vaccination among COVID-19 vaccinees, and unvaccinated person-time of persons who did not receive a COVID-19 vaccine by May 31, 2021. To ensure comparable health care–seeking behavior among persons who received a COVID-19 vaccine and those who did not (unvaccinated persons), eligible unvaccinated persons were selected from among those who received ≥1 dose of influenza vaccine in the last 2 years. Separate unvaccinated groups were selected for mRNA and Janssen vaccines.** Deaths were identified through VSD, which captures hospital deaths and deaths reported to health plans. In this study, non–COVID-19 deaths were assessed because a protective effect of COVID-19 vaccination for COVID-19–related deaths was expected. Non–COVID-19 deaths were those that did not occur within 30 days of an incident COVID-19 diagnosis or receipt of a positive test result for SARS-CoV-2 (the virus that causes COVID-19) via reverse transcription–polymerase chain reaction or rapid test.
Standardized mortality rates (SMRs) (deaths per 100 person-years) were calculated and compared with a rate ratio test between vaccinated and unvaccinated groups (6); a population of VSD members who were enrolled in December 2020 was used as the standard population. Overall SMRs were reported separately for Pfizer-BioNTech, Moderna, and Janssen vaccines. Poisson models were used to calculate overall aRRs and 95% CIs adjusted for age, sex, race and ethnicity, and VSD site. SMRs and aRRs by age, sex, and race and ethnicity were also calculated, adjusting for other demographic characteristics. Analytical units were aggregated counts of deaths and person-years by vaccination status, age, sex, race and ethnicity, and VSD site. All analyses were conducted using SAS statistical software (version 9.4; SAS Institute).†† This work was reviewed by CDC and VSD sites§§ and was conducted consistent with applicable federal law and CDC policy.¶¶
The cohort consisted of 6.4 million COVID-19 vaccinees and 4.6 million unvaccinated persons with similar characteristics as the comparison groups. Among 3.5 million Pfizer-BioNTech vaccine recipients, 9.2% were aged 12–17 years, 69.4% were aged 18–64 years, 54.0% were female, 42.7% were White persons, 21.4% were Hispanic persons, 16.6% were Asian persons, and 5.1% were Black persons (Table 1). Among 2.6 million Moderna vaccine recipients, 71.7% were aged 18–64 years, 54.5% were female, 44.2% were White persons, 23.1% were Hispanic persons, 14.2% were Asian persons, and 5.6% were Black persons. Among 342,169 Janssen vaccine recipients, 87.5% were aged 18–64 years, 4.1% were aged ≥75 years, 48.0% were female, 45.1% were White persons, 20.3% were Hispanic persons, 13.4% were Asian persons, and 6.1% were Black persons.
After excluding COVID-19–associated deaths, overall SMRs after dose 1 were 0.42 and 0.37 per 100 person-years for Pfizer-BioNTech and Moderna, respectively, and were 0.35 and 0.34, respectively, after dose 2 (Table 2). These rates were lower than the rate of 1.11 per 100 person-years among the unvaccinated mRNA vaccine comparison group (p <0.001). Among Janssen vaccine recipients, the overall SMR was 0.84 per 100 person-years, lower than the rate of 1.47 per 100 person-years among the unvaccinated comparison group (p <0.001). Among persons aged 12–17 years, SMRs were similar among the Pfizer-BioNTech vaccine recipients and unvaccinated comparison groups (p = 0.68 after dose 1 and 0.89 after dose 2). SMRs were also similar between Janssen vaccine recipients and unvaccinated comparison groups among Asian persons (p = 0.11). Among other subgroups defined by vaccine received, age, sex, and race and ethnicity, COVID-19 vaccine recipients had lower SMRs than did their unvaccinated counterparts (p <0.05).
The overall aRR among Pfizer-BioNTech vaccine recipients compared with the unvaccinated comparison group was 0.41 (95% CI = 0.38–0.44) after dose 1 and 0.34 (95% CI = 0.33–0.36) after dose 2 (Table 3). Among Pfizer-BioNTech vaccine recipients aged 12–17 years, mortality risk among vaccinated and unvaccinated persons was similar after dose 1 (aRR = 0.85; 95% CI = 0.38–1.90) and after dose 2 (aRR = 0.73; 95% CI = 0.33–1.64). Among other age groups, aRRs ranged from 0.35 (95% CI = 0.29–0.42) among persons aged 45–64 years to 0.46 (95% CI = 0.39–0.54) among persons aged ≥85 years after dose 1, and from 0.28 (95% CI = 0.25–0.31) among persons aged 45–64 years to 0.39 (95% CI = 0.36–0.43) among those aged ≥85 years after dose 2. Similar aRRs among vaccinated persons compared with the unvaccinated comparison group were observed for recipients of the Moderna vaccine, ranging from 0.31 (95% CI = 0.26–0.37) among persons aged 45–64 years to 0.46 (95% CI = 0.31–0.69) among persons aged 18–44 years after dose 1, and 0.28 (95% CI = 0.26–0.32) among persons aged 65–74 years to 0.38 (95% CI = 0.29–0.50) among those aged 18–44 years after dose 2. The overall aRR for Janssen was 0.54 (95% CI = 0.49–0.59), and age-stratified aRRs ranged from 0.40 (95% CI = 0.34–0.49) among persons aged 45–64 years to 0.68 (95% CI = 0.56–0.82) among persons aged ≥85 years. Across vaccine type and dose, males and females had comparable aRRs. All vaccinated racial and ethnic groups had lower mortality risks than did unvaccinated comparison groups.
Discussion
In a cohort of 6.4 million COVID-19 vaccinees and 4.6 million demographically similar unvaccinated persons, recipients of the Pfizer-BioNTech, Moderna, or Janssen vaccines had lower non–COVID-19 mortality risk than did the unvaccinated comparison groups. There is no increased risk for mortality among COVID-19 vaccine recipients. This finding reinforces the safety profile of currently approved COVID-19 vaccines in the United States. The lower mortality risk after COVID-19 vaccination suggests substantial healthy vaccinee effects (i.e., vaccinated persons tend to be healthier than unvaccinated persons) (7,8), which will be explored in future analyses. Mortality rates among Janssen vaccine recipients were not as low as those among mRNA vaccine recipients. This finding might be because of differences in risk factors, such as underlying health status and risk behaviors among recipients of mRNA and Janssen vaccines that might also be associated with mortality risk.
Among persons aged 12–17 years, mortality risk did not differ between Pfizer-BioNTech vaccinees and unvaccinated persons; only 12 deaths occurred in this age group during the study period. The unvaccinated group might be more similar to the vaccinated group in risk factors than are vaccinated and unvaccinated adults. Stratified analyses by age, sex, and race and ethnicity showed that vaccinated adults had lower mortality than did unvaccinated adults across subgroups.
The findings in this report are subject to at least four limitations. First, the study was observational, and individual-level confounders that were not adjusted for might affect mortality risk, including baseline health status, underlying conditions, health care utilization, and socioeconomic status. Second, healthy vaccinee effects were found in all but the youngest age group. Such effects were also found in a cohort study conducted in a nursing home population, which reported substantially lower aRRs for 7-day mortality among vaccinated residents after dose 1 (0.34) and dose 2 (0.49) as compared with unvaccinated residents (5). Lower rates of non–COVID-19 mortality in vaccinated groups suggest that COVID-19 vaccinees are inherently healthier or engage in fewer risk behaviors (7,8); future analyses will address these issues. Third, although deaths associated with COVID-19 were excluded, causes of death were not assessed. It is possible that the algorithm used might have misclassified some deaths associated with COVID-19 because of lack of testing or because individual mortality reviews were not conducted. Finally, the findings might not be applicable to the general population. The VSD includes approximately 3% of the U.S. population, and is representative of the general population with regard to several demographic and socioeconomic characteristics (9). Other studies have already demonstrated the safety of COVID-19 vaccines authorized in the United States.
Despite these limitations, this study had several strengths. First, this was a cohort study with a large, sociodemographically diverse population, and it encompassed a study period of >7 months. Second, VSD sites were able to capture COVID-19 vaccines administered not just within but also outside their health care systems, including COVID-19 vaccine doses recorded in state immunization registries, allowing for more complete ascertainment of vaccination status. Third, the assignment of index dates allowed COVID-19 vaccinees to contribute unvaccinated person-time before vaccination, thus avoiding immortal time bias (10), which can confer a spurious survival advantage to the treatment group in cohort studies. Index date assignments made the follow-up period comparable between COVID-19 vaccinees and their comparators and helped control for seasonality and general trends in mortality.
CDC recommends that everyone aged ≥12 years should receive a COVID-19 vaccine to help protect against COVID-19.*** This cohort study found lower rates of non–COVID-19 mortality among vaccinated persons compared with unvaccinated persons in a large, sociodemographically diverse population during December 2020–July 2021. There is no increased risk for mortality among COVID-19 vaccine recipients. This finding reinforces the safety profile of currently approved COVID-19 vaccines in the United States.
Corresponding author: Stanley Xu, Stan.Xu@kp.org.
1) Research and Evaluation, Kaiser Permanente Southern California, Pasadena, California; 2) CDC COVID-19 Response Team;
3) Health Partners Institute, Minneapolis, Minnesota;
4) Institute for Health Research, Kaiser Permanente Colorado, Denver, Colorado;
5) Kaiser Permanente Vaccine Study Center, Kaiser Permanente Northern California, Oakland, California;
6) Marshfield Clinic Research Institute, Marshfield, Wisconsin;
7) Center for Health Research, Kaiser Permanente Northwest, Portland, Oregon;
8) Immunization Safety Office, CDC.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Runxin Huang reports support for attending meetings or travel from Dynavax Technologies. Nicola P. Klein reports institutional support from Pfizer, Sanofi Pasteur, Merck, GlaxoSmithKline, and Protein Science (now Sanofi Pasteur to support vaccine studies). Elizabeth G. Liles reports research contracts from the National Human Genome Research Institute and Pfizer. Kerresa Morrissette reports research contracts from the National Institutes of Health, GlaxoSmithKline, and Merck Sharp & Dohme Corporation, outside the submitted work. No other potential conflicts of interest were disclosed.
* https://covid.cdc.gov/covid-data-tracker/#vaccinations
† https://ourworldindata.org/coronavirusexternal icon (Accessed September 21, 2021).
§ Among nine VSD sites, (all health care organizations), data is included from seven sites: Kaiser Permanente (KP) Southern California, Pasadena, California; KP Northern California, Oakland, California; KP Colorado, Denver, Colorado; KP Northwest, Portland, Oregon; KP Washington, Seattle, Washington; HealthPartners, Minneapolis, Minnesota; and Marshfield Clinic, Marshfield, Wisconsin. Harvard Pilgrim Health Care Institute, Boston, Massachusetts, did not participate in this study because it is not a data-contributing site; Denver Health, Denver, Colorado, did not participate in this study because of limited resources.
¶ Persons who were vaccinated during December 14, 2020–May 31, 2021 were included in the vaccinated group. In each VSD site, age group, and sex stratum, the distribution of vaccination dates of dose 1 were obtained and used to assign index dates to all persons. Among vaccinated persons, if the index date was before the vaccination date of dose 1, follow-up started on the index date, and persons in this group contributed both unvaccinated person-time (from index date to the day before vaccination date) and vaccinated person-time (from vaccination date); if the index date was on or after the vaccination date of dose 1, follow-up started on the vaccination date, and persons in this group only contributed person-time after vaccination. Follow-up ended upon death, disenrollment from health plans, receipt of a COVID-19 vaccine for unvaccinated persons during June 1, 2021–July 31, 2021, or end of follow-up (July 31, 2021), whichever occurred first.
** All available eligible comparators were used for analysis of mRNA COVID-19 vaccines. Because the Janssen COVID-19 vaccine was authorized months after the mRNA COVID-19 vaccines and demographic characteristics of Janssen versus mRNA COVID-19 vaccine recipients might differ, a separate group of comparators was selected for Janssen vaccine recipients on the basis of calendar time and demographic characteristics of Janssen vaccine recipients. Because the number of Janssen vaccine recipients was smaller, four eligible comparators were randomly selected for each vaccinated individual to achieve optimal statistical power.
†† The procedure STDRATE was used to conduct rate ratio tests, and the procedure GENMOD was used to fit Poisson models.
§§ All activities were approved by the institutional review boards at some participating institutions or as public health surveillance activities at other participating institutions.
¶¶ 45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. Sect. 241(d); 5 U.S.C. Sect. 552a; 44 U.S.C. Sect. 3501 et seq.
*** https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/adolescents.html (Accessed October 13, 2021).
References
- Polack FP, Thomas SJ, Kitchin N, et al.; C4591001 Clinical Trial Group. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N Engl J Med 2020;383:2603–15. https://doi.org/10.1056/NEJMoa2034577external icon PMID:33301246external icon
- Baden LR, El Sahly HM, Essink B, et al.; COVE Study Group. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021;384:403–16. https://doi.org/10.1056/NEJMoa2035389external icon PMID:33378609external icon
- Food and Drug Administration. Janssen COVID-19 vaccine Emergency Use Authorization letter. Silver Spring, MD: US Department of Health and Human Services, Food and Drug Administration; 2021. https://www.fda.gov/media/146303/downloadexternal icon
- Finney Rutten LJ, Zhu X, Leppin AL, et al. Evidence-based strategies for clinical organizations to address COVID-19 vaccine hesitancy. Mayo Clin Proc 2021;96:699–707. https://doi.org/10.1016/j.mayocp.2020.12.024external icon PMID:33673921external icon
- Bardenheier BH, Gravenstein S, Blackman C, et al. Adverse events following mRNA SARS-CoV-2 vaccination among U.S. nursing home residents. Vaccine 2021;39:3844–51. https://doi.org/10.1016/j.vaccine.2021.05.088external icon PMID:34092431external icon
- Breslow NE, Day NE. Statistical methods in cancer research. Volume II—the design and analysis of cohort studies. IARC Sci Publ 1987;82:1–406. PMID:3329634external icon
- Jackson LA, Nelson JC, Benson P, et al. Functional status is a confounder of the association of influenza vaccine and risk of all cause mortality in seniors. Int J Epidemiol 2006;35:345–52. https://doi.org/10.1093/ije/dyi275external icon PMID:16368724external icon
- Simonsen L, Taylor RJ, Viboud C, Miller MA, Jackson LA. Mortality benefits of influenza vaccination in elderly people: an ongoing controversy. Lancet Infect Dis 2007;7:658–66. https://doi.org/10.1016/S1473-3099(07)70236-0external icon PMID:17897608external icon
- Sukumaran L, McCarthy NL, Li R, et al. Demographic characteristics of members of the Vaccine Safety Datalink (VSD): a comparison with the United States population. Vaccine 2015;33:4446–50. https://doi.org/10.1016/j.vaccine.2015.07.037external icon PMID:26209836external icon
- Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol 2008;167:492–9. https://doi.org/10.1093/aje/kwm324external icon PMID:18056625external icon
TABLE 1. Demographic characteristics of COVID-19 vaccine recipients and unvaccinated comparison group — seven integrated health care organizations, United States, December 14, 2020–July 31, 2021
Characteristic
No. (%)
mRNA vaccine*
Janssen vaccine
Pfizer-BioNTech vaccine recipients
Moderna vaccine recipients
Unvaccinated comparison group†,§
Janssen vaccine recipients
Unvaccinated comparison group†
Total
3,452,126 (100.0)
2,604,066 (100.0)
3,243,112 (100.0)
342,169 (100.0)
1,346,445 (100.0)
Age group, yrs
12–17
316,587 (9.2)
NA
311,445 (9.6)
NA
NA
18–44
1,322,147 (38.3)
951,899 (36.6)
1,153,735 (35.6)
141,317 (41.3)
558,996 (41.5)
45–64
1,072,819 (31.1)
913,075 (35.1)
987,703 (30.5)
158,157 (46.2)
624,106 (46.4)
65–74
440,879 (12.8)
454,391 (17.4)
468,679 (14.5)
28,721 (8.4)
109,143 (8.1)
75–84
219,888 (6.4)
216,968 (8.3)
233,870 (7.2)
9,835 (2.9)
37,745 (2.8)
≥85
79,806 (2.3)
67,733 (2.6)
87,680 (2.7)
4,139 (1.2)
16,455 (1.2)
Sex
Male
1,586,867 (46.0)
1,185,265 (45.5)
1,395,196 (43.0)
177,867 (52.0)
696,190 (51.7)
Female
1,865,259 (54.0)
1,418,801 (54.5)
1,847,916 (57.0)
164,302 (48.0)
650,255 (48.3)
Race/Ethnicity
Hispanic
738,931 (21.4)
600,654 (23.1)
871,863 (26.9)
69,602 (20.3)
329,921 (24.5)
White, non-Hispanic
1,472,716 (42.7)
1,151,826 (44.2)
1,397,345 (43.1)
154,188 (45.1)
585,489 (43.5)
Asian, non-Hispanic
573,754 (16.6)
369,069 (14.2)
432,782 (13.3)
45,909 (13.4)
200,430 (14.9)
Black, non-Hispanic
175,066 (5.1)
145,127 (5.6)
189,592 (5.8)
20,996 (6.1)
73,174 (5.4)
Multiple races/Other/Unknown
491,659 (14.2)
337,390 (13.0)
351,530 (10.8)
51,474 (15.0)
157,431 (11.7)
Abbreviations: Janssen = Johnson & Johnson; NA = not applicable.
* Among Pfizer-BioNTech COVID-19 vaccine recipients, 2,980,152 received the second dose by May 31, 2021; among Moderna COVID-19 vaccine recipients, 2,362,157 received the second dose by May 31, 2021.
† Unvaccinated comparison group included unvaccinated persons and COVID-19 vaccine recipients before COVID-19 vaccination. The assignment of index dates allowed COVID-19 vaccinees to contribute unvaccinated person-time before vaccination, thus avoiding immortal time bias.
§ mRNA vaccines included Pfizer-BioNTech and Moderna COVID-19 vaccines.
TABLE 2. Number of deaths and standardized mortality rate (deaths per 100 person-years) not associated with COVID-19 among COVID-19 vaccine recipients and unvaccinated comparison groups, by age, sex, and race/ethnicity — seven integrated health care organizations, United States, December 14, 2020–July 31, 2021
Characteristic
No. of deaths* (standardized mortality rate per 100 person-years)
mRNA vaccine
Janssen vaccine
Pfizer-BioNTech vaccine recipients†
Moderna vaccine recipients†
Unvaccinated comparison group§
Vaccine recipients¶
Unvaccinated comparison group§
After dose 1
After dose 2
After dose 1
After dose 2
Overall**
1,157 (0.42)
5,143 (0.35)
1,202 (0.37)
4,434 (0.34)
6,660 (1.11)
671 (0.84)
2,219 (1.47)
Age group,†† yrs
12–17
2 (0.01)
3 (0.01)
NA
NA
7 (0.01)
NA
NA
18–44
20 (0.02)
73 (0.02)
24 (0.03)
57 (0.02)
161 (0.07)
19 (0.04)
63 (0.08)
45–64
117 (0.16)
409 (0.13)
123 (0.16)
421 (0.17)
910 (0.51)
130 (0.25)
497 (0.66)
65–74
235 (0.79)
994 (0.62)
249 (0.63)
920 (0.58)
1,407 (2.13)
144 (1.49)
466 (2.77)
75–84
338 (2.32)
1,591 (1.89)
376 (2.00)
1,425 (1.77)
1,861 (6.34)
176 (5.59)
549 (9.13)
≥85
445 (7.90)
2,073 (6.85)
430 (7.16)
1,611 (6.57)
2,314 (18.76)
202 (15.35)
644 (23.76)
Sex§§
Male
587 (0.49)
2,584 (0.41)
640 (0.45)
2,352 (0.42)
3,265 (1.30)
326 (0.96)
1,102 (1.68)
Female
570 (0.35)
2,559 (0.29)
562 (0.30)
2,082 (0.28)
3,395 (0.96)
345 (0.75)
1,117 (1.31)
Race/Ethnicity**
Hispanic
144 (0.36)
584 (0.29)
197 (0.35)
701 (0.33)
1,230 (1.07)
92 (0.91)
365 (1.24)
White, non-Hispanic
781 (0.47)
3,560 (0.39)
732 (0.39)
2,804 (0.37)
3,993 (1.17)
416 (0.85)
1,364 (1.58)
Asian, non-Hispanic
72 (0.23)
408 (0.23)
67 (0.18)
317 (0.21)
460 (0.78)
56 (0.83)
157 (1.09)
Black, non-Hispanic
84 (0.54)
300 (0.37)
130 (0.65)
340 (0.44)
623 (1.53)
65 (0.99)
187 (1.97)
Multiple races/Other/Unknown
76 (0.38)
291 (0.28)
76 (0.32)
272 (0.29)
354 (0.82)
42 (0.68)
146 (1.22)
Abbreviations: Janssen = Johnson & Johnson; NA = not applicable.
* Number of deaths as of July 31, 2021; deaths that occurred ≤30 days after an incident COVID-19 diagnosis or receipt of a positive SARS-CoV-2 test result were excluded.
† Vaccinated with mRNA COVID-19 vaccines during December 14, 2020–May 31, 2021.
§ Unvaccinated comparison group included unvaccinated persons and COVID-19 vaccine recipients before COVID-19 vaccination. The assignment of index dates allowed COVID-19 vaccinees to contribute unvaccinated person-time before vaccination, thus avoiding immortal time bias.
¶ Vaccinated with Janssen COVID-19 vaccine during February 27, 2021–May 31, 2021.
** Overall mortality rates and race- and ethnicity-specific mortality rates were age- and sex-standardized.
†† Age-specific mortality rates were sex-standardized.
§§ Sex-specific mortality rates were age-standardized.
TABLE 3. Adjusted relative risks for mortality of COVID-19 vaccine recipients and unvaccinated comparison groups*— seven integrated health care organizations, United States, December 14, 2020–July 31, 2021
Characteristic
Vaccine type, aRR, (95% CI)
Pfizer-BioNTech
Moderna
Janssen
After dose 1
After dose 2
After dose 1
After dose 2
After dose 1
Overall†
0.41 (0.38–0.44)
0.34 (0.33–0.36)
0.34 (0.32–0.37)
0.31(0.30–0.33)
0.54 (0.49–0.59)
Age group,§ yrs
12–17
0.85 (0.38–1.90)
0.73 (0.33–1.64)
NA
NA
NA
18–44
0.37 (0.24–0.57)
0.36 (0.28–0.46)
0.46 (0.31–0.69)
0.38 (0.29–0.50)
0.55 (0.36–0.82)
45–64
0.35 (0.29–0.42)
0.28 (0.25–0.31)
0.31 (0.26–0.37)
0.33 (0.29–0.37)
0.40 (0.34–0.49)
65–74
0.39 (0.33–0.47)
0.32 (0.29–0.35)
0.32 (0.27–0.37)
0.28 (0.26–0.32)
0.50 (0.39–0.63)
75–84
0.38 (0.33–0.46)
0.32 (0.29–0.35)
0.32 (0.27–0.38)
0.29 (0.26–0.32)
0.58 (0.48–0.71)
≥85
0.46 (0.39–0.54)
0.39 (0.36–0.43)
0.38 (0.32–0.45)
0.35 (0.31–0.39)
0.68 (0.56–0.82)
Sex¶
Male
0.41 (0.37–0.46)
0.35 (0.33–0.38)
0.36 (0.32–0.40)
0.33 (0.31–0.35)
0.52 (0.46–0.60)
Female
0.41 (0.36–0.45)
0.33 (0.31–0.36)
0.33 (0.29–0.37)
0.30 (0.28–0.32)
0.56 (0.49–0.64)
**Race/Ethnicity****
Hispanic
0.36 (0.30–0.42)
0.29 (0.26–0.32)
0.33 (0.29–0.39)
0.31 (0.28–0.34)
0.58 (0.46–0.73)
White, non-Hispanic
0.44 (0.38–0.50)
0.37 (0.34–0.40)
0.35 (0.30–0.40)
0.32 (0.30–0.35)
0.53 (0.46–0.61)
Asian, non-Hispanic
0.31 (0.25–0.39)
0.32 (0.28–0.36)
0.23 (0.18–0.30)
0.27 (0.23–0.30)
0.68 (0.52–0.88)
Black, non-Hispanic
0.38 (0.31–0.47)
0.27 (0.24–0.31)
0.42 (0.35–0.49)
0.29 (0.25–0.32)
0.47 (0.36–0.63)
Multiple races/Other/Unknown
0.46 (0.36–0.60)
0.35 (0.30–0.41)
0.40 (0.30–0.51)
0.36 (0.30–0.42)
0.52 (0.38–0.71)
Abbreviations: aRR = adjusted relative risk; CI = confidence interval; Janssen = Johnson & Johnson; NA = not applicable; VSD = Vaccine Safety Datalink.
* Unvaccinated comparison groups included unvaccinated persons and COVID-19 vaccine recipients before COVID-19 vaccination. The assignment of index dates allowed COVID-19 vaccinees to contribute unvaccinated person-time before vaccination, thus avoiding immortal time bias.
† Overall relative risks were adjusted for age, sex, race and ethnicity, and VSD site.
§ Relative risks by age were adjusted for sex, race and ethnicity, and VSD site.
¶ Relative risks by sex were adjusted for age, race and ethnicity, and VSD site.
** Relative risks by race and ethnicity were adjusted for age, sex, and VSD site.
Suggested citation for this article: Xu S, Huang R, Sy LS, et al. COVID-19 Vaccination and Non–COVID-19 Mortality Risk — Seven Integrated Health Care Organizations, United States, December 14, 2020–July 31, 2021. MMWR Morb Mortal Wkly Rep 2021;70:1520–1524. DOI: http://dx.doi.org/10.15585/mmwr.mm7043e2external icon.