Monthly Shaarli
November, 2021
 a.image2.image-link.image2-928-1456 { padding-bottom: 63.73626373626373%; padding-bottom: min(63.73626373626373%, 928px); width: 100%; height: 0; } a.image2.image-link.image2-928-1456 img { max-width: 1456px; max-height: 928px; }
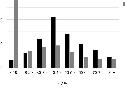
a.image2.image-link.image2-928-1456 { padding-bottom: 63.73626373626373%; padding-bottom: min(63.73626373626373%, 928px); width: 100%; height: 0; } a.image2.image-link.image2-928-1456 img { max-width: 1456px; max-height: 928px; }Yet again I had to draw this graph myself, and yet again, the UK Health Security Agency wants you to know that these rates are extremely, totally, absolutely unadjusted. They just don’t know precisely why or how.
As I noted on Twitter, it’s emerged that UKHSA inserted all of their ill-advised disclaimers after coming under fire from the Office of Statistics Regulation, a regulatory body which periodically complains about statistics published by the British government.
OSR director Ed Humpherson met with UKHSA hours before they published their Week 43 report, demanding they do something about these awkward graphs. They responded by ditching the graphs altogether and calling every last number unadjusted. This failed to satisfy him, so in the days afterwards he issued this unbelievable open letter.
Dear Jenny,
COVID-19 vaccine surveillance statistics
Thank you for the constructive meeting on Thursday 28 October to discuss the UK Health Security Agency’s (UKHSA) COVID-19 vaccine surveillance statistics. We focused on the risk that the data presented on rates of positive cases for those who are vaccinated and those who are unvaccinated have the potential to mislead – and indeed we noted that these data have been used to argue that vaccines are ineffective.
We welcome the changes you have made to the Week 43 surveillance report, published on 28 October. It is also very good that you are working closely with my team and with the relevant teams in the Office for National Statistics (ONS).
The UK has backed itself into publishing some less-than-useful numbers. Now the office responsible for this publishing will have to work closely with a gaggle of political commissars, responsible for cleansing official discourse of anything that might be “used to argue that vaccines are ineffective.”
Because he appears to be a genuinely stupid man, Humpherson spells this point out explicitly:
It remains the case that the surveillance report includes rates per 100,000 which can be used to argue that vaccines are not effective. I know that this is not the intention of the surveillance report, but the potential for misuse remains. In publishing these data, you need to address more comprehensively the risk that it misleads people into thinking that it says something about vaccine effectiveness.
Emphasis mine. The next time somebody tells you that UKHSA reports show substantial protection against severe outcomes, draw their attention to Ed Humpherson’s letter. He thinks these numbers don’t tell you anything about anything. This is the first step towards not publishing them at all.
This is not just about the choice of denominator. It is about recognising that the comparison of case rates for vaccinated and unvaccinated groups is comparing datasets with known differences – including, potentially, the greater propensity of people who are vaccinated to come forward for tests. So the data reflect a behavioural phenomenon, not just a feature of how well vaccines work. I do not think your surveillance report goes far enough in explaining this crucial point.
Emphasis mine again. Humpherson has no idea what behavioural factors might be at issue. He is just throwing random ideas at the wall, here. And notice how he slithers from what is “potentially” true to totally unqualified and unsupported assertions about is true (“the data reflect a behavioural phenomenon”). Maybe the higher unvaccinated death rates also “reflect a behavioural phenomenon“ and are “not just a feature of how well vaccines work.” As long as we are allowed to speculate baselessly, let’s do it in both directions.
He goes on to voice the old and tired complaint about the NIMS data. He wants UKHSA to use ONS population estimates instead. While the former might well understate the case rate among the unvaccinated, the latter is sure to overstate it, but Humpherson doesn’t care.
One possibility would be to only publish rates in the vaccinated population, which are known accurately, but I recognise your concern that you are already publishing rates for both groups.
Confirmation yet again of the obvious: They are only publishing these numbers because they locked themselves into doing so early on, when they looked good.
The alternative would be to use the ONS population estimates, which are used in the main coronavirus dashboard but which may be flawed for some age groups, as you have pointed out. … In the meantime, you should consider setting out these uncertainties more clearly, including by publishing the rates per 100,000 using both denominators, and making clear in the table, perhaps through formatting, that the column showing case rates in unvaccinated people is of particular concern.
That column is of particular concern because Humpherson doesn’t like the numbers in that column. He doesn’t care about the other columns because those numbers are neutral or pleasing to him.
And he closes with this:
I recognise that you want to maintain transparency and consistency, but these qualities should not be at the expense of informing the public appropriately.
Remember, always, that all Corona statistics are propaganda.
The UKHSA have issued a separate set of disclaimers on their website. Every line is fairly hilarious. And the Office of Statistical Regulation provides their own wall of text, where they show that if you understate the unvaccinated population with ONS numbers, indeed you can get the unvaccinated case rate to go up. Humpherson and his crack team of statistics regulators just love the ONS numbers, but UKHSA don’t like them so much. This is because UKHSA actually have to compile minimally plausible tables and for this they are unworkable. From p. 15 of the Week 44 report:
When using ONS, vaccine coverage exceeds 100% of the population in some age groups, which would in turn lead to a negative denominator when calculating the size of the unvaccinated population.
This letter from Marc Wathelet, PhD, Expert in Molecular Biology and Immunology, is addressed to the Belgian Minister of Health, Frank Vandenbroucke, and analyzes not only the mandates imposed on health care workers but also the vaccination of children and the “Safe Ticket” vaccination passport intended for the general population. The content of the letter is relevant not only to the Belgian situation but also to that of other countries adopting this kind of coercive measures, that are particularly questionable as for their public health benefits.
(The letter is available in French at this LINK)
Dear Mr. Vandenbroucke , Deputy Prime Minister and Minister of Social Affairs and Public Health
Thank you for your response to our letter concerning the compulsory vaccination of health care workers, which you justify based on a certain number of assertions which are however not supported by documentation of scientifically established facts.
On the contrary,
the scientific data available to date contradict all of your arguments and, as detailed below, we can only conclude that the compulsory vaccination of health care workers is not only useless, but also counterproductive from a public health perspective. Such compulsory vaccination also violates the principles of bio-ethics and medical ethics as well as our human rights.
1) Compulsory Vaccination of Health Care Workers is Unnecessary
Mandatory vaccination of health care workers is unnecessary because studies show beyond a reasonable doubt that it does not prevent the contamination of an individual, nor does it reduce the viral load of infected people, and therefore their ability to transmit the virus to others.
In appendix A you will find a long list of facts, scientific publications and official statements from qualified agencies and individuals, such as Dr. Fauci, who confirms our assertion that vaccination does not prevent the disease. the contamination of an individual and his ability to transmit the delta variant circulating today to others.
We will only take a recent example here: on September 23, the Irish Examiner announced that in the city of Waterford, 99.7% of those over 18 were fully vaccinated, which is the highest total in the entire European Union . On October 11, Waterford News & Star reported that the city had the highest incidence rate in Ireland.
There is only one conclusion to be drawn, which cannot be disputed in good faith: beyond studies, in the real world, in practice: vaccination does not make it possible to prevent the transmission of SARS-CoV-2 in the community.
2) Mandatory Vaccination of Health Care Workers is Counterproductive from a Public Health Point of View
The message that COVID vaccines would be “safe and effective,” an unsupported claim if only for the lack of the necessary hindsight, was hammered out constantly for months in all the media. One of the negative effects of this campaign is the acceptance of this assertion as an established fact, not only by the population but also by its leaders.
As a result, vaccinated people respect less behaviors such as social distancing or wearing a mask. And since they are more likely to be asymptomatic when infected, which makes them less aware of the risk they pose to others, they are actually more likely to spread the virus than non-vaccinated people.
In practice, this means that the COVID Safe Ticket (Belgian vaccination passport) is not only useless but also counterproductive. It is a license for vaccinated people to infect others, whether they are vaccinated or not.
The same reasoning applies to health care workers, even if they observe social distancing more scrupulously: vaccinating all health care workers will not prevent the contamination of “sick or vulnerable people because of their great age” which you are rightly concerned about.
We agree with you that “people taken care of have the right to maximum safety”. We offer two non-exclusive alternatives to the compulsory vaccination of health care workers, which will be much more effective in preventing nosocomial infections:
1) Have all nursing staff, vaccinated or not, tested at high frequency. In this regard, note that nasopharyngeal tests are not without risk, as reported by the Academy of Medicine in France. Two other safer methods can be considered: an oro-pharyngeal antigen test or an oral PCR test.
2) Establish a voluntary ivermectin prophylaxis program: There are 14 studies that support the effectiveness of this approach.
Finally, the compulsory vaccination of health care workers is counterproductive from a public health point of view because those who still refuse to be vaccinated will no longer be able to work, and therefore the number of health care workers, already in short supply, will be even smaller, with a negative impact on public health.
In France, there are ~ 300,000 unvaccinated health care workers (~10%), and 15,000 of them are already suspended from their job. In Belgian hospitals, 9.4% of health care workers are not vaccinated and in elderly / nursing homes, 13.1% are not.
3) The Illusion of Herd Immunity
You say: “Scientists say that 70% of the total population (including children) would need to be fully vaccinated for everyone to be protected. With the Delta variant, which is more contagious than the first variants, we continue to aim for that 70%, but we are striving to achieve the highest percentage possible.”
This opinion seems to be shared above all by the experts appointed by the government. On the contrary, many scientists had anticipated that vaccinating during a pandemic was not a sufficient approach to control the virus, and events proved them right (see Appendix A for a list of citations).
You say that “Vaccination reduces the circulation of the virus”. This is contradicted by the articles cited above about the delta variant (Appendix A), the example of the City of Waterford, and now a large study shows that the increases in COVID-19 are indeed not linked to the levels of vaccination worldwide (cf the comparative study of 68 countries, as well as 2,947 counties in the United States).
4) The Dangers of COVID vs. the Dangers of Vaccination
You say, “If we’re afraid of variants, we certainly need to vaccinate more today.” Since hard data indicates that vaccination does not work in practice, even when everyone is vaccinated, the solution cannot be to vaccinate more!
There is no reason to be afraid of variants: on the one hand the lethality of the Delta variant is one tenth of the Alpha according to Public Health England, and on the other hand the lethality of COVID is intrinsically weak. It is mainly linked to the presence of comorbidities (99% of deaths occur in people with comorbidity, 96% in people with multiple comorbidities, Appendix B ).
Importantly, this lethality is comparable to that caused by other respiratory infections. Therefore, neither the COVID Safe Ticket nor the compulsory vaccination are justifiable from a public health point of view!
Those at risk have had the opportunity to be vaccinated or can take prophylactic treatment if they choose not to be vaccinated. The situation of these individuals cannot therefore justify putting other healthy individuals at unnecessary risk.
The risks inherent in COVID vaccinations, in the medium and long term, simply remain unknown, due to the lack of the necessary hindsight (we note, however, the prolonged post-vaccination syndrome, similar to long COVID). The short-term risk is evident despite the intense efforts of the health authorities, mainstream media and big tech to suppress all information on this subject.
For example, the Israeli Ministry of Health published an article on its Facebook page about severe adverse reactions, that it described as very rare only, to find itself inundated by a deluge of contrary opinions from its citizens (14,000 in a few hours), opinions that were swiftly deleted. Denying this reality is not a solution to the problem.
Facebook is routinely removing any group that identifies adverse reactions to vaccines, groups with tens of thousands of users in the United States and elsewhere. By what right? In French speaking countries alone, the (non-exhaustive) collection of screenshots of these individual reports testifies to the catastrophic scale of the phenomenon.
Pharmacovigilance databases around the world are all reporting an increase in severe adverse reactions and deaths from COVID vaccines (WHO; United States - VAERS; United Kingdom - Yellow Card; European Union - Eudravigilance).
Analysis of VAERS data, for example, shows a much higher incidence for COVID vaccines than for influenza severe adverse events (28 times more) and deaths (57 times more, see Appendix B). What’s the use of these pharmacovigilance sites if such data are brushed aside as irrelevant, when on the contrary, they should call for the suspension of the vaccination campaign?
The fact-checking sites, financed by the pharmaceutical industry, come to the rescue of the official narrative by affirming that there is no proof that these deaths are attributable to the vaccines. This is to reverse the burden of proof!
According to a report from the French medications agency ANSM (January 28, 2021), the official pharmacovigilance rule is this: “The analysis of reported cases takes into account clinical, chronological, semiological and pharmacological data. It may lead to the vaccine’s responsibility for the occurrence of an observed adverse event being dismissed only when another, certain, cause is identified.”
In fact, an audit of data reported to VAERS shows that only 14% of deaths following vaccination can be attributed to another cause, and it is not just anyone filling such reports, as 67% of the reports have been made by a doctor. Similarly, in Eudravigilance, 79% of the reports regarding a death were filed by a health care professional.
In reality, all of the Bradford Hill criteria are mostly observed, which means that these vaccines are the cause of most of the reported adverse reactions. When autopsies, which are too rarely done, are performed, between 30 and 100% of deaths are attributable to vaccination (see annex B).
These databases are poorly designed, leading to erroneous reports on both sides of the debate. For example, we see circulating for Eudravigilance a figure greater than 25,000 deaths following vaccination against COVID. A more rigorous analysis indicates 7,174 deaths as of October 9, 2021. VAERS analysis gives a number of deaths of the same order of magnitude (7,680, as of October 8, 2021).
These pharmacovigilance systems are passive, leading to a very significant underreporting of the real number of cases. A factor of 5 seems conservative, but regardless of the exact number, what is indisputable is that people in good health, without co-morbidities, young people, die from vaccination or are seriously injured.
A rotavirus vaccine was withdrawn from the market in 1999 because of only 15 cases of intussusception. The swine flu vaccination campaign in 1976 was halted after 25 deaths. We are at about 3,000 times more at the minimum (appendix B). How many more deaths will it take before we realize the obvious?
Data shows that those who are cautious about vaccines are more educated on average than those who favour vaccination, contrary to how they are portrayed in the media.
And the reality of serious adverse effects due to vaccination is confirmed by the fact that it is precisely health care workers who do not want to be vaccinated, despite their education and the fact that they are generally in favour of vaccination (they are not anti-vaxxers!), because they are on the front line and can see the damage these vaccines cause.
It is therefore deeply immoral to make vaccination compulsory, whether it concerns health care workers or any category of citizens. Likewise, it is unethical to encourage the vaccination of groups of individuals who were excluded from the Phase 3 of the clinical trials, in particular pregnant women and those under the age of 18.
Children deaths due to COVID are extremely rare and observed exclusively in individuals suffering from severe co-morbidities. Therefore the deaths of healthy children already recorded following vaccination should lead to an immediate moratorium on the vaccination of children. This should also apply to pregnant women, especially given the absence of information on the long-term effects of these injections.
Compulsory vaccination violates not only ethics, but also fundamental concepts of rights, as demonstrated by Alessandro Negroni, professor of philosophy of law at the University of Genoa.
In light of European and international law, genetic anti-covid vaccines constitute a medical experiment on human beings. From an ethical as well as a legal point of view, no one can be obliged to submit to a form of medical experimentation in the absence of free and informed consent.
We hope that you will take this analysis into account and that you will realize that we must abandon the idea of compulsory vaccination with experimental products for anyone, as well as the implementation of a COVID Safe Ticket based on anything else than a recent test.
Let us also abandon therapeutic nihilism, and treat infected individuals early, as medicine had always done before the start of this crisis.
Yours faithfully,
By ReinfoCovid Belgium and the non-profit “Notre Bon Droit”
Analysis by Marc G. Wathelet, Ph.D. (Molecular Biology)
APPENDIX A – Data on the Effects of Vaccination on Infection and Transmission
The effect of vaccination on the risk of SARS-CoV-2 infection and its transmission to others was modest in the initial studies, but the rapid decline in immunity in vaccinated individuals and the appearance of more contagious variants makes this effect negligible today, as discussed in detail in this document https://www.linkedin.com/pulse/questions-sur-limmunisation-et-la-transmission-de-marc-wathelet/?published=t , drafted as part of a legal action by the non-profit organization “Notre Bon Droit” in opposition to the “COVID Safe Ticket” — the Belgian Government’s vaccination passport.
This document dates from July 28, 2021, and contains 50 references and the studies that have appeared since that date only confirm this analysis:
- https://www.medrxiv.org/content/10.1101/2021.07.28.21261295v1
- https://onlinelibrary.wiley.com/doi/10.1111/joim.13372
- https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v1
- https://www.medrxiv.org/content/10.1101/2021.08.12.21261951v2
- https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w
- https://www.medrxiv.org/content/10.1101/2021.09.28.21264262v1.full.pdf
- https://www.medrxiv.org/content/10.1101/2021.09.02.21262979v1
- https://www.medrxiv.org/content/10.1101/2021.09.28.21264260v1.full.pdf
- https://link.springer.com/article/10.1007/s10654-021-00808-7
- https://www.nejm.org/doi/pdf/10.1056/NEJMoa2114583?articleTools=true
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(2102183-8/fulltext)
Data from Public Health England up to the 40th week of 2021
The most recent data from Public Health England indicate that in all cohorts the rate of infection is higher in vaccinated than in unvaccinated people from the age of 30. In these conditions, the obligation of vaccination is simply absurd.
The CDC and Dr. Fauci recognized the impact of the greater contagiousness of the Delta variant and did reinstate the wearing of the mask for the vaccinated.
In addition, the document cited above also [compares immunity against SARS-CoV-2 acquired following vaccination and that following natural infection and shows that the latter is more robust, wider and more balanced regarding the production of antibodies and T cells. It also lasts longer than the vaccine-induced immunity, which translates into better and longer lasting protection against infection for individuals having recovered from COVID compared to vaccinees.
Health care workers are among those who have been most exposed to the virus so far, so it would be absurd to impose a vaccination on them when, for many of them, their natural immunity is more effective. Here too, the studies that have appeared since only confirm this analysis:
- https://www.medrxiv.org/content/10.1101/2021.08.12.21261951v2
- https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1
- https://www.bmj.com/content/bmj/374/bmj.n2101.full.pdf
The #Covidrationnel collective in Belgium, which includes around thirty university professors, researchers and doctors, carried out a similar analysis and reached the same conclusions
These studies are confirmed by observations in the real world, in the jurisdictions with the highest vaccination rates such as the Seychelles, Gibraltar and Iceland. The high rate of vaccination does not prevent significant waves of infections that follow shortly the vaccination campaign.
More recently, in the city of Waterford in Ireland where 99.7% of the people over 18s are fully vaccinated, one observes the highest incidence rate in Ireland (618.9 infected per 100,000 over the last 2 weeks).
A recent global study shows increases in COVID-19 cases are indeed unrelated to immunization levels across the world (68 countries and 2,947 counties in the United States).
APPENDIX B – The Dangers of COVID vs. the Dangers of COVID Vaccination
From a public health point of view, it is not helpful to consider the general case fatality rate. Rather, it’s a question of identifying populations at risk.
-
a. The Dangers of COVID
The dangers of COVID are related to age and the presence of comorbidities. 99% of deaths occur in people with comorbidity, 96% in people with multiple comorbidities according to the US CDC
COVID survival rates by age group according to Dr. Ioannidis’ team:
Age Survival rate 0-19 99.9973% 20-29 99.986% 30-39 99.969% 40-49 99.918% 50-59 99.73% 60-69 99.41% 70+ 94.5% These figures do not distinguish COVID from other respiratory infections in terms of lethality, and therefore do not justify a different approach to manage this disease from a public health perspective. Therefore, neither the COVID Safe Ticket nor compulsory vaccination are justified from a public health point of view!
-
b. The Dangers of COVID Vaccination
There are excellent vaccines, with a very favorable risk-benefit ratio, against severe diseases, such as tetanus or yellow fever, for example. However, the benefit-risk ratio sometimes turns out to be unfavorable, and the vaccine in question is then withdrawn from the market.
For example, a rotavirus vaccine was taken off the market in 1999 due to only 15 cases of intussusception .
The swine flu vaccination campaign in 1976 was interrupted after 25 deaths . It also caused 532 cases of Guillain-Barré syndrome.
What about the COVID Vaccines?
A simple correlation is not synonymous with causation. We rely on the Bradford Hill criteria, which are widely verified for these vaccines as shown below. They are:
1) Strength of the association (the larger the magnitude of the effects associated with the association, the more likely a causal link is, even if a small effect does not imply no causal link);
2) Stability of the association (its repetition in time and space)
3) Consistency (the same observations are made in different populations);
4) Specificity (a cause produces a particular effect in a particular population in the absence of other explanations);
5) Temporal relationship (temporality). The causes must precede the consequences;
6) Dose-effect relationship (a larger dose leads to a larger effect);
7) Plausibility (biological plausibility, possibility of explaining the mechanisms involved);
8) Experimental evidence (in animals or in humans);
9) Analogy (possibility of alternative explanations).
For example, temporality ( # 5 ) shows a very high incidence of death in the days following vaccination, before falling back to the normal level
The same profile of adverse reactions is observed in Europe and the United States ( # 3 ), listed below, in decreasing order of frequency compared to their respective norm:
pulmonary embolism, stroke, deep vein thrombosis, thrombosis, increased fibrin D dimers, appendicitis, tinnitus, cardiac arrest, death, Parkinson’s disease, slow speech, aphasia (inability to speak), fatigue, pericardial effusion, headache head, chills, pericarditis, deafness, myocarditis, intracranial hemorrhage, spontaneous abortion, cough, Bell’s palsy, paresthesia, blindness, dyspnea (difficulty breathing), myalgia, dysstasia (difficulty standing), convulsions, anaphylactic reaction, suicide , speech disorder, thrombocytopenic thrombotic purpura, paralysis, swelling, diarrhea, neuropathy, multiple organ dysfunction syndrome, depression.
Their number increases with the level of vaccination, and there is specificity ( # 4 ), the adverse effect profile shown above is different from that observed for influenza vaccines but is similar to the effects of COVID; also, some populations are affected differently, for example myocarditis and pericarditis affect more young men.
Biological plausibility ( # 7 ): COVID vaccines produce the SARS-CoV-2 spike protein in our cells just as infection with the virus does, and the side effects mimic those seen in disease; the Spike protein shows in vitro intrinsic toxicity towards endothelial cells and cardiac pericytes:
- https://www.sciencedirect.com/science/article/pii/S096999612030406X?via%3Dihub
- https://www.biorxiv.org/content/10.1101/2021.04.30.442194v1
- https://www.biorxiv.org/content/10.1101/2020.12.21.423721v2
- https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
Experimental evidence (animal or human, # 8 ), mouse experiments reproduce myopericarditis.
Strength of association ( # 1 ) and stability ( # 2 ):
Report of serious adverse reactions and deaths for all COVID vaccines per million doses compared to annual influenza vaccines from 2016 to 2021, to the H1N1 strain of influenza vaccine in 2009-2010, and to all vaccines except those against COVID from 2006 to 2021 in the US VAERS system.Analysis of VAERS data shows a much higher incidence for COVID vaccines than for influenza severe side effects (28X plus) and death (57X plus).
Absolute numbers of serious adverse reactions and deaths in VAERS for the 3 vaccines in the United States against COVID, and their ratio by number of injections
An audit of VAERS data shows that only 14% of deaths following vaccination can be attributed to another cause; at least 67% of reports were initiated by a physician
As the VAERS system is passive, only a small proportion of real cases are recorded there. This proportion can be estimated on the basis of a study of 64,900 employees of a Massachusetts hospital measuring the serious reactions compatible with anaphylaxis that can occur immediately after vaccination: they occurred at a rate of 2.47 per cent. 10,000 vaccinations. The incidence rate of anaphylaxis confirmed in this study is higher than that reported by the CDC on the basis of passive methods (VAERS) of spontaneous notification (0.025-0.11 per 10,000 vaccinations).
These data suggest that the under-reporting in VAERS is by a factor of between 22.5 and 98.8!
This indicates that the number of deaths exceeds 150,000 and the number of severe side effects exceeds one million in the United States:
Absolute figures of serious adverse reactions and deaths in the European Economic Area for the 4 vaccines against COVID, and their ratio by number of injections. 79% of death reports were initiated by healthcare personnel.
The official rule in pharmacovigilance:
The analysis of reported cases takes into account clinical, chronological, semiological and pharmacological data. It may lead to the vaccine’s responsibility for the occurrence of an observed adverse event being dismissed as soon as another, certain cause is identified.
When autopsies, which are too rarely done, are performed, between 30 and 100% of deaths are attributable to vaccination. Peter Schirmacher, chief pathologist at Heidelberg University, determined that autopsy reports indicate that, conservatively, at least 30-40% of a sample of 40 people who died within two weeks of vaccination actually died from the vaccine. .
Professors Arne Burkhardt and Walter Lang, forensic pathologists, presented the results of ten autopsies in Reutlingen on Monday, September 20. Of the ten deaths, seven are “probably” related to the injections, of which five are “very likely”. For the last three cases, one of them remains to be evaluated, another seems to be “a coincidence”, and for the last, the link “is possible but not certain”.
In Norway, when 23 deaths following vaccination occurred in an EHPAD, the authorities carried out 13 autopsies and these 13 deaths were found to be linked to vaccination .
A French drug assessment center concluded that COVID vaccination should be discontinued, for all 4 products. And the Moderna vaccine is abandoned by some countries for the youngest (Norway, Sweden, Denmark; France for the second dose).
Finally, in an article titled “Why are we vaccinating children against COVID?, the authors conclude that not only is their vaccination contraindicated, but that even for the most vulnerable subjects over 65 years of age, the risk-benefit analysis shows that there are 5 times more deaths attributable to vaccination than to disease.
It is against bioethics and the law to vaccinate groups of individuals who were excluded from phase 3 clinical trials, especially those under the age of 18.
Society, by vaccinating children, puts them at risk in order to protect adults without considering their well-being, while it is the responsibility of adults to protect themselves.
It is also not only incorrect that the delta variant would be more dangerous for children, but data from the British National Statistics Office (ONS) indicates a 46% increase in deaths in the 15-19 age group since their vaccination was authorized (+ 63% in young men, + 16% in young women # 4 ), compared to the same period in 2020.
This letter, dated October 17, is translated from French and reproduced with permission from a post on LinkedIn. Please refer to the original version in French for any formal reference.

Pfizer/BioNTech’s Comirnaty COVID shot was approved (licensed) by the U.S. Food and Drug Administration in late August 2021, but only for adults, and only when carrying the Comirnaty label. No other COVID shot has been FDA approved. However, Comirnaty is currently not available, and while the experimental, emergency use authorized (EUA) Pfizer shot is substituted for Comirnaty, the two products are clearly legally distinct and not the same
A licensed vaccine is not shielded from liability until or unless it’s added to the recommended childhood vaccination schedule by the CDC. So, if you were injured by Comirnaty, you could sue Pfizer. You cannot sue if injured by the EUA Pfizer shot (or any of the other EUA COVID injections)
Even though several hundred claims have been filed with the Countermeasures Injury Compensation Program (CICP) for injuries resulting from the COVID shots — which is the only possible avenue to obtain damages — not a single claim has been paid out
Natural immunity is much stronger than what you can achieve from the injection, which only provides antibodies against the SARS-CoV-2 spike protein and wanes within a few months. The shots may in fact permanently limit the kind of immune response you would make were you to later be exposed or infected with COVID
Children’s Health Defense has filed a lawsuit arguing you cannot have a vaccine that is both an emergency use product and a licensed product at the same time. That’s against the law, but the government has done it anyway. Remarkably, the request for an injunction was initially thrown out, but the CHD has not given up and is still pursuing the case
In this interview, Dr. Meryl Nass, an internist specializing in toxicology, vaccine-induced illnesses and Gulf War illness, shares her insights into the dangers of the COVID jab, which received an emergency use authorization October 26, 2021, for children as young as 5.
We also discuss the conflicts of interest within the U.S. Food and Drug Administration that seem to be behind this reckless decision, and how the agency pulled the wool over our eyes with its approval of Pfizer/BioNTech’s Comirnaty COVID injection.
Is the COVID Jab Approved or Not?
As explained by Nass:
“All of the COVID ‘vaccines,’ and most of the COVID treatment products, have not been [FDA] approved. Approved means licensed. All except one, which is the Pfizer vaccine for adults, age 16 and up, which got approved, i.e., licensed on August 23 [2021].
But every other vaccine, and for every other age group, including the boosters, have only been authorized under emergency use authorizations (EUAs). There’s a critical difference [between licensing and EUA]. Once a drug is fully licensed, it is subject to liability.
If the company injures you with that product, you can sue them, unless it later gets put on the CDC’s childhood schedule or is recommended by the CDC [U.S. Centers for Disease Control and Prevention] [during] pregnancy, in which case it obtains a different liability shield.
It then becomes part of the National Vaccine Injury Compensation Program (NVICP, established under the 1986 National Childhood Vaccine Injury Act), and 75 cents from every dose of vaccine that is sold in the United States goes into a fund to pay for injuries that way.”
The National Childhood Vaccine Injury Act removed liability for all vaccines recommended by the CDC for children. Since 2016, they’ve also removed liability for vaccines given to pregnant women, a category that has become the latest “gold rush” for vaccines. Naturally, once a company is no longer liable for injuries, the profitability of the product in question increases dramatically.
Countermeasures Injury Compensation Program Is Nearly Useless
Products under emergency use have their own special government program for liability called the Countermeasures Injury Compensation Program (CICP). “It is a terrible program,” Nass says. CICP is an offshoot of the 2005 PREP Act.
“The PREP act enabled the CICP to be created by Congress,” Nass explains. “Congress has to allocate money for it. If you are injured by an emergency use product, you don’t get any legal process. The companies have had all their liability waived. There is a single process that is administered through HHS [Health and Human Services].
Some employees there decide whether you deserve to be compensated or not. The maximum in damages you can obtain is about $370,000 if you’re totally disabled or die, and the money is only to compensate you for lost wages or unpaid medical bills.”
So far, even though several hundred CICP claims have been filed for injuries resulting from the COVID shots, not a single claim has been paid out. This is important, because the statute of limitations is one year. “It’s getting close to running out for people who were vaccinated early,” Nass says.
If you fail to apply in time, you lose the opportunity to get any compensation entirely. “Of course, in fact, it’s really ‘an opportunity’ to apply and get nothing because almost nobody gets paid,” she says. At that point, you have no further recourse. There’s no appeals process to the judicial system.
“You can ask the HHS twice to compensate you, and if they say no, that’s it,” Nass explains. “You can attempt to sue the company that made the product, if you’re convinced it was improperly made, but the secretary of HHS has to give you the permission to sue.
You have to prove that there was willful misconduct and no one has ever reached that bar. So, there has never been a lawsuit under this. Anyway, that’s what you’re looking at. If you get the vaccine under EUA and are injured, you’re on your own. People have no idea about this when they vaccinate themselves or their children.”
Why Were the Shots Mandated?
As you know by now, president Biden decided to mandate the COVID jab for most federal employees (but not all) and private companies with 100 employees or more. “We don’t know why that is,” Nass says. It doesn’t make sense, as large numbers of Americans have already recovered from COVID-19 and have durable, long-lasting immunity already.
As correctly noted by Nass, natural immunity is much stronger than what you can achieve from the injection, which only provides antibodies against the SARS-CoV-2 spike protein and wears off within a few months. The shots “may in fact permanently limit the kind of immune response you would make were you to be infected with COVID later,” Nass says.
For these reasons, there’s absolutely no good reason to vaccinate people who have recovered from the infection and several bad reasons. There’s evidence showing the shot can be more harmful for those with existing immunity.
“But for reasons best known to itself, the Biden administration feels so certain it needs to vaccinate everybody that it has used illegal means to tell employers they will lose federal contracts if they don’t force their employees to be vaccinated immediately, and must fire them — if they’re health care workers, for example, or government employees, or military — if they have not been vaccinated.
Obviously that is creating a great deal of chaos, particularly within the health care industry, particularly in my state, Maine, where these draconian rules have gone into effect and many fire department, police, EMTs, nurses and doctors can no longer work.
The one thing that was necessary to push mandates forward was for the government to be able to say it had a licensed product. Before the emergency use authorization was created in 2005, you had licensed drugs and you had experimental drugs and nothing else.
There was no gray area between them. Any use of a medication or vaccine that is not fully licensed is still experimental, despite the fact that a new category of drugs has been created with emergency use authorizations.
These are still experimental drugs, so under emergency use, you can’t force people [to take them]. You have to offer them options and they have the right to refuse. Since that is part of the statute, the federal government can’t get around it.
Therefore, attorneys in the Biden administration knew they could not legally impose mandates under an EUA, and so they demanded that FDA provide a COVID vaccine full approval, aka, an unrestricted license. This was believed to enable them to impose mandates.
They must have put pressure on the FDA, and FDA gave them what they wanted, which was a license for the Pfizer vaccine called Comirnaty on August 23 [2021].”
Comirnaty Approval Includes Important Caveats
In the documents released August 23, 2021, by the FDA, there were some interesting caveats. They said the Comirnaty vaccine is essentially equivalent to the EUA vaccine and the two vaccines may be used interchangeably. However, they pointed out that the two are legally distinct. Curiously, FDA didn’t specify what these legal distinctions are.
“I concluded that the legal distinctions were the fact that under EUA, there was essentially no manufacturer liability, but once the vaccine got licensed, the manufacturer would be subject to liability claims unless and until the vaccine was placed on the childhood schedule or recommended in pregnancy, in which case it would then fall … under the NVICP,” Nass says.
“Right now, Comirnaty is still not in that injury compensation program, and it’s licensed, so it no longer falls under the CICP. So, it is in fact subject to liability if you get injured with a bottle that says Comirnaty on it. Of course, if you’re Pfizer, what do you want to do?
You don’t want to make that licensed product available until several months have gone by and Comirnaty has been put into the National Vaccine Injury Compensation Program. So, Pfizer and FDA have not made the licensed product available yet.
What has happened instead, in the military, is the FDA has made a secret deal with the military and said, certain emergency use lots can be considered equivalent to the licensed vaccine, and [told military medical staff] which QR codes — which lots can be used. [These specific lots] can then be given to soldiers as if they’re licensed.
Subsequently, we’re told that military clinics are actually putting Comirnaty labels onto bottles that are under EUA. Now, that probably can happen in the military, but only in the military, because there are likely to be memoranda of understanding within the military that we haven’t seen yet that say soldiers cannot sue Pfizer for injuries …
In the military, the government and Pfizer feel like they have set up a situation where nobody can sue, but in the civilian world, that has not happened, and so there is no Comirnaty available.
Yet, on the basis that FDA licensed this product, the federal government is still telling employers that they can mandate it and that they must fire employees that have not taken the vaccine, or they will lose government contracts. We’re in a very interesting situation that is ripe for litigation, and Children’s Health Defense, which is an organization I represent, is litigating some of this.
However, the litigation situation has been very difficult since the pandemic began. Cases that normally would’ve been easy wins are being thrown out by the courts, both in the U.S. and in Europe. Something strange has happened and the judges are looking for any way out, so they don’t have to rule on the merits of these cases.”
The organization Children’s Health Defense has filed a lawsuit arguing you cannot have a vaccine that is both an emergency use product and a licensed product at the same time. That’s against the law, but the federal government did it anyway. Remarkably, the request for an injunction was initially thrown out, but Children’s Health Defense hasn’t given up and is still pursuing that case.
COVID Jab Is Authorized for 5- to 11-Year-Olds in the US
As mentioned, the FDA recently authorized the EUA COVID jab for children between the ages of 5 and 11, which is simply appalling, considering they are at virtually no risk from COVID-19. I’ve not seen a single recorded case in the entire world of anyone in that age group dying of COVID that didn’t have a serious preexisting comorbidity, such as cancer.
If you have a healthy child, they are at no risk from the infection, so there’s only danger associated with this shot, which in this age group would be one-third the adult dose. Typically, when you’re giving a drug to a child, the dose is calculated based on the child’s weight. Here, they’re giving the same dose to a 5-year-old as an 11-year-old, despite there being a significant difference in weight. So, it’s pure guesswork.
Worse yet, the mRNA vaccines produce an unpredictable amount of spike protein, and even if they produce much too much, there is no way to turn off the process once you have been injected.
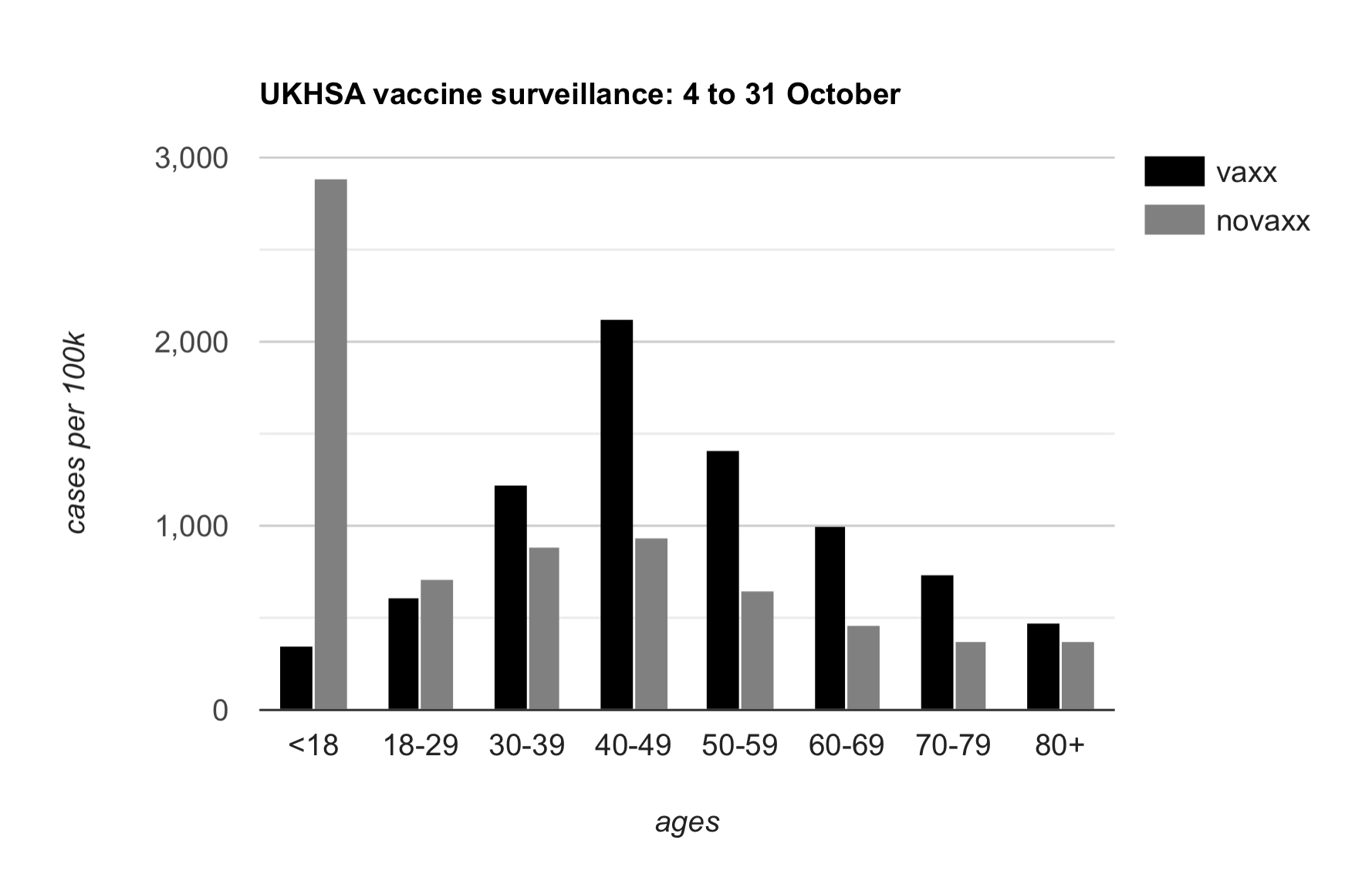
Despite clear safety signals, the FDA’s advisory committee authorized the Pfizer jab for 5- to 11-year-olds unanimously, 17-to-0 (with one abstaining vote). However, when you look at the roster of the FDA’s committee members1 who reviewed and voted to authorize the Pfizer shot for children as young as 5, the unanimous “yes” vote becomes less of a mystery.
Abhorrent Conflicts of Interest
As reported by National File2 and The Defender,3 the membership of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) has had staggering conflicts of interest. Members have included:
In addition to that, former FDA commissioner Scott Gottlieb is currently on Pfizer’s board of directors. As noted by Nass, two of the members, one permanent and one temporary, are also CDC career employees whose job it is to push vaccines at the CDC.
“If they voted against authorizing a vaccine, they would be out of a job,” Nass says. “They have no business on that committee … It’s a very unethical stew of advisory committee members …
What happened is Pfizer delivered a large package of information to the FDA on October 6, 2021. FDA staff had to go through this large packet of information on the 5- to 11-year-olds and produce their own report, which was about 40 pages long, and create talks to give to the advisory committee, and they did all of this in 17 days.
There was apparently very little critical thought that went into their presentations. Before the meeting, Children’s Health Defense, and I was one of the authors, wrote to the committee and to FDA officials saying, ‘Look, there’s all these reasons that don’t make logical or medical sense for vaccinating kids in this age group, because they almost never get very ill or die, and the side effects of the vaccine are essentially unknown.
We know there are a lot of side effects, but the federal government has concealed from us the rate at which these side effects occur. But we know that the rate from myocarditis is very high, probably at least 1 in 5,000 young males … which is a very serious side effect. It can lead, probably always leads, to some scarring. It can lead to sudden death, to heart failure.”
Trials in Young Children Were Insufficient
As explained by Nass, in the clinical trial, there were two groups of children. The first group was enrolled for two to three months, while the second group was enrolled for just 17 days after receiving the second dose. (Pfizer added the second group because FDA claimed there weren’t enough volunteers in the first group.)
These two groups comprised over 3,000 children who got the jab and 1,500 or 2,000 who got a placebo. None suffered serious side effects. This was then translated into the claim that the injection was safe. However, as noted by Nass:
“They didn’t look at safety in all these kids. Even though FDA had said, ‘Add kids to your clinical trial,’ Pfizer created a ‘safety subset’ of one-tenth of the vaccinated subjects.
It was this small number of kids from whom they drew blood to show they had adequate levels of neutralizing antibodies, which was a surrogate for efficacy, because they didn’t have enough cases of COVID in this abbreviated trial to show that the vaccine actually works in this age group.”
Even though the advisory committee acknowledged that the blood test done for efficacy had not been validated, and wasn’t reliable evidence of effectiveness, they still decided that all children, regardless of health status, would benefit from the injection.
They also ignored the fact that at least half the children are already immune, and giving them the injection will provide no additional benefit in terms of immunity, while putting them at increased risk for serious side effects.
“Nobody said, ‘Look, the parents of healthy kids may be dying for a vaccine, but that’s because we haven’t told them the truth about the vaccine. We haven’t told them their kids don’t need it. We haven’t told them it’s going to potentially damage future immunity.
We haven’t told them they’re at higher risk of side effects than if they never had COVID. We’re not allowing them to go get antibody tests to establish that they’re already immune and therefore should be waved from being vaccinated.’
The committee members were aware of all this stuff, but in the end [they voted yes] … apart from one very smart member of the committee who works for the National Institutes of Health. He abstained. He didn’t have the guts to vote no, but he knew this was a bad idea.”
Children Are Being Injected Without Parental Consent
While all of that is bad enough, parents of young children now face the possibility of their children being injected against their will and without their knowledge. Nass comments:
“As I said, we don’t know why the government wants everybody vaccinated, but there’s probably a reason that goes beyond protecting us from COVID.
The government got the FDA to authorize the vaccine for 12- to 15-year-olds on May 10 [2021], and subsequently that group, which is about 6 million kids, has been getting vaccinated across the country. That’s under emergency use so, again, you can’t sue.
But something kind of evil happened, which was many cities began vaccinating 12- to 15-year-olds in the absence of parental permission. So, a child could show up with their friends or a friend’s mother at a vaccine center and get vaccinated with no one asking about their medical history, nobody calling the parents. No notation got entered into the child’s medical record that they were vaccinated.
Vaccinators were told to make their own assessment. If they thought this child could give consent, go ahead and vaccinate. Now, that is a gross violation of our laws, and yet it was happening in Boston, in Philadelphia, in Seattle, in San Francisco, and we have good documentation of it.
The government currently is planning for mobile vaccination clinics for kids and vaccinations in schools, and they may take this program of vaccinating without parental consent down to the 5- to 11-year-olds …
In fact, we may see clinics popping up that don’t require informed consent in the 5- to 11-year-old group. Let me just mention that the chief medical officer in Canada’s British Columbia said they have brought laws that allow children of any age to consent for themselves. Think about that. A baby can consent for vaccinations for itself. It would be funny if it wasn’t so diabolical.”
All of this goes against the most basic concept of medical ethics, which is informed consent. No one has the right to perform a medical procedure on you without your consent, or the consent of a legal guardian. The government, again, without establishing any new laws, is simply bypassing the legal system.
Will Young Children Be at Risk for Myocarditis?
Based on her review of the scientific literature, Nass suspects younger children in the now COVID jab-approved, 5- to 11-year-old age group will be at exponentially higher risk of myocarditis and other side effects compared to the 12- to 15-year group, where we’ve already seen a documented increase.
“In the letter that Children’s Health Defense wrote to the advisory committee for the FDA, we created a graph based on the reporting rate of myocarditis versus age, and we showed there was an exponential curve.
Men aged 65 and up had a rate that was 1/100th the rate of boys aged 12 to 17. If that exponential curve keeps going up, the rate in the 5- to 11-year-olds could be even dramatically higher. In those young men, a 1 in 5,000 rate was reported to VAERS [Vaccine Adverse Events Reporting System]. That’s not a real rate.
That just tells us how many people got diagnosed with myocarditis, and then went to the trouble of reporting it to the FDA. The FDA and CDC have a large number of other databases from which they can gather rates of illness.
VAERS is considered passive reporting. It is not considered fit for purpose to establish illness rates because we don’t know how many people report. Do 1 in 10 report, 1 in 100, 1 in 50? Nobody knows.
However, again, because everything is crazy since the pandemic came in, the CDC has tried to pull the wool over our eyes and has claimed that the rate of anaphylaxis in the population from COVID vaccines is identical to their reporting rate to VAERS. We know that’s not true.
On the CDC’s website, that’s what they have. Elsewhere on the website, they say you can’t take a VAERS rate and call it an actual rate of reactions, but they’ve done that [for anaphylaxis]. And they’re trying to obfuscate the fact that they’re not giving you real rates, and sort of pretending that the myocarditis rate is probably the VAERS reporting rate of myocarditis, although they’re not saying so directly.”
Nass goes on to recount an example from the smallpox vaccine, which also caused myocarditis. A military study that just looked at cases sent to specialists found roughly 1 in 15,000 developed myocarditis. A military immunologist then dug deeper, and drew blood on soldiers before and after vaccination, and found a myocarditis rate of 1 in 220 after receiving the smallpox vaccine.
However, 1 soldier in 30 developed subclinical myocarditis where troponin rose from normal to more than two times the upper limits of normal. While asymptomatic, 1 in 30 had measurable inflammation of the heart. “Right now, in terms of what the rate is for COVID, nobody is looking, no federal agency wants to find out the real rate,” Nass says.
You Can’t Find Problems You Refuse to Look For
A simple study that measures troponin levels — a marker for heart inflammation and damage — before and after each dose, could easily determine what the real rate of myocarditis is, yet that is not being done.
“This is what we’re dealing with,” Nass says. “All these databases, which is about a dozen different databases, that CDC and FDA said they could access to determine the rates of side effects after vaccination with COVID vaccines, they’re either not being used or being used improperly,” Nass says.
“It was discovered that a new algorithm was being used to study the VAERS database that only came into use in January 2021, immediately after the vaccines were authorized, and the algorithm was developed such that you compare two vaccines to each other.
If the pattern of side effects was similar between the two vaccines — which is often the case because there’s a limited number of general vaccine adverse reactions — even if one vaccine has a thousand times more side effects as the one it is being compared to, by using this flawed algorithm, if the pattern of reactions was the same, even though the rates were 1,000 times higher for one, the algorithm would fail to detect a problem.
That is the algorithm they’re using to analyze VAERS [data]. They’re also using bad methods … to analyze the vaccine safety database, which encompasses 12 million Americans who enrolled in HMOs around the country. The CDC pays for access to their electronic medical records and their data.
Somehow when these databases have been looked at carefully, they’re finding very low rates of myocarditis in boys, approximately equal to the VAERS reporting. It was said months ago, ‘We can’t find a safety signal for myocarditis. We’re not finding an anaphylaxis signal. we’re not finding a Bell’s palsy signal.’
The FDA’s and CDC’s algorithms couldn’t pick up for most known side effects. So, there’s something wrong with the analytic methods that are being used, but the agencies haven’t told us precisely what they are. What we do know is that the rates of side effects that are being reported to VAERS are phenomenal.
They’re orders of magnitude higher than for any previous vaccines used in the United States. An order of magnitude is 10-fold, so rates of reported adverse reactions are 10 to 100 times higher than what has been reported for any other vaccine. Reported deaths after COVID in the United States are 17,000+. It’s off the charts.
Other side effects reported after COVID vaccinations total over 800,000. Again, more deaths and more side effects than have ever been reported for every vaccine combined in use in the U.S. cumulatively over 30 years.”
Despite all this shocking data, our federal agencies look the other way, pretending as if nothing is happening, and no matter how many people approach them — with lawsuits, with public comments, reaching out to politicians — they refuse to address blatantly obvious concerns. This is clear evidence that they’re acting with intentional malice.
FDA has become Clown World, and what they do now is to perform a charade of all the normal regulatory processes that they are expected to perform … You’re the guinea pigs, but they’re not collecting the data. Nobody should get these shots. ~ Dr. Meryl Nass
The FDA and CDC are supposed to protect the public. They’re supposed to identify safety concerns. They’re not supposed to act as marketing firms for drug companies, but that’s precisely what they’ve been converted to.
New Formulations Have Never Been Tested
Another truly egregious fact is that Pfizer has altered its formulation, allegedly to make it more stable, but this new formulation has never been included in any of the trials. Nass explains:
“During the October 26, 2021, VRBPAC [Vaccines and Related Biological Products Advisory Committee] meeting, Pfizer said, ‘Look, we want to give the vaccines in doctor’s offices and we’ve found a way to stabilize the vaccine so we don’t need those ultra-cold fridges anymore. We can put these vials in a doctor’s office and, once defrosted, they can sit in a regular fridge 10 weeks and they’ll be fine.’
Some committee members asked, ‘OK, what’d you do? How did you make this marvelous discovery?’ And they said, ‘We went from the phosphate buffered saline buffer to a Tris buffer, and we slightly changed some electrolytes.’ A committee member asked, ‘OK, how did that make it so much more stable?’ And everybody in the meeting from FDA and Pfizer looked at each other and said, ‘We don’t know.’
An hour later, Pfizer had one of their chemists get on the line, but he couldn’t explain how the change in buffer led to a huge increase in stability, either. Then, later in the meeting, one of the members of the committee asked, ‘Did you use this new formulation in the clinical trial?’
And Dr. Bill Gruber, the lead Pfizer representative, said, ‘No, we didn’t.’ In other words, Pfizer plans, with FDA connivance, to use an entirely new vaccine formulation in children, after their clinical trials used the old formulation. This is grossly illegal. They’ve got a new formulation of vaccine. It wasn’t tested in humans. And they’re about to use it on 28 million American kids.”
It’s nothing short of a dystopian nightmare. Completely surreal. You can’t make this stuff up. Yet as shocking as all this is, earlier this year, Dr. Anthony Fauci projected that these COVID jabs would be available for everyone, from infants to the elderly. Now they’ve got the 5-year-olds, and there’s every reason to suspect they’ll go after newborns and infants next.
Whose Babies Will Be Offered Up as Sacrificial Lambs?
According to Nass, Pfizer and the FDA have struck a deal that will allow Pfizer to test on babies even younger than 6 months old, even if there’s no intention to inject infants that young. Those trials may begin as early as the end of January 2022.
“This arrangement between FDA and Pfizer will give Pfizer its extra six months of patent protection, whether or not these vaccines are intended to be used in those age groups. So, you can look at these trials as a way of almost sacrificing little children, because when you start a trial, you don’t know what the dangers are going to be.
I could be wrong, but I doubt we’re going to give these to newborn babies the way we give the hepatitis B vaccine on the date of birth, yet they will be tested in very young babies. The question is, whose babies get tested? In the past, sometimes the babies that got tested were foster children, wards of the state. Sometimes parents offer up their children. But there will be clinical trials.”
When will we get the data from those trials? It turns out that in the agreements reached between Pfizer and the FDA, some of those trials won’t conclude until 2024, 2025 and 2027. The goal here is to vaccinate all Americans, children and adults, within the coming few months or a year, yet it’ll be five years before we actually know from clinical trials what the side effects may be.
We’re Living in Clown World
As noted by Nass, this is yet another crime. It may fulfill the letter of the law, but it doesn’t fulfill the meaning of the law. It makes no sense to run clinical trials that won’t be completed until five years after your mass vaccination program has been completed and the entire population is injected.
“It’s just a joke to do that,” Nass says. “But FDA has become Clown World, and what they do now is to perform a charade of all the normal regulatory processes that they are expected to do, but they’re only doing them in an abbreviated or peculiar manner so that they don’t really collect the important data.
For example, the control group has been vaccinated two months into the Pfizer trials, which effectively obscures side effects that develop after two months. Blood is not tested for evidence of myocarditis or blood clots using simple tests (troponin and D-dimer levels).
For all the Americans out there who haven’t spent 20 years examining the FDA procedures like I have, these FDA advisory committee meetings are it’s designed to make you think a real regulatory process is going on, when it’s not. Instead we are all guinea pigs, but no one is collecting the data that would normally be required to authorize or approve a vaccine. Therefore, in my opinion, nobody should get these shots.“
To make matters even worse, it’s actually illegal to grant EUAs for these vaccines, because there are drugs that can prevent the condition (COVID), as well as treat it. EUAs can only be granted if there are no existing approved, available alternatives to prevent or treat the infection.
The effective drugs most have already heard of are ivermectin and hydroxychloroquine, but there are a number of other drugs that also have profound effects on COVID, Nass says, including TriCor and cyproheptadine (Periactin).
TriCor, or fenofibrate, emulsifies lipid nanoparticles and fatty conglomerations that contain viruses and inflammatory substances. The drug essentially allows your body to break down the viral and inflammatory debris better. As such, it might also help combat complications caused by the nanoliposomes in the COVID shot.
According to Nass, Pepcid at high doses of up to 80 milligrams three times a day is also useful for treatment. Dr. Robert Malone is starting a clinical trial using a combination of Pepcid and celecoxib (brand name Celebrex). Many are also recommending aspirin to prevent platelet activation and clotting.
I believe a far better alternative to aspirin is lumbrokinase, and/or serapeptase. Both are fibrinolytic enzymes that address blood clotting. You can develop sensitivity to them, so I recommend alternating the two on alternate days for about three months if you’ve had COVID.
You could rule out blood clotting by doing a D-dimer test. If your D-dimer is normal, you don’t need an anticlotting agent. If clotting is a concern, you could also use NAC in addition to these fibrinolytic enzymes. It too helps break up clots and prevent clot formation.

NNTV, the standard policy tool that Pharma, the FDA, & CDC no longer want to talk about
A funny thing happened this afternoon. Not funny as in “haha”. More like funny as in, “ohhhhh that’s how the FDA rigs the process.”
I was reading the CDC’s “Guidance for Health Economics Studies Presented to the Advisory Committee on Immunization Practices (ACIP), 2019 Update” and I realized that the FDA’s woeful risk-benefit analysis in connection with Pfizer’s EUA application to jab children ages 5 to 11 violates many of the principles of the CDC’s Guidance document. The CDC “Guidance” document describes 21 things that every health economics study in connection with vaccines must do and the FDA risk-benefit analysis violated at least half of them.
Today I want to focus on a single factor: the Number Needed to Vaccinate (NNTV). In four separate places the CDC Guidance document mentions the importance of coming up with a Number Needed to Vaccinate (NNTV). I did not recall seeing an NNTV in the FDA risk-benefit document. So I checked the FDA’s risk-benefit analysis again and sure enough, there was no mention of an NNTV.
Because the FDA failed to provide an NNTV, I will attempt to provide it here.
First a little background. The Number Needed to Treat (NNT) in order to prevent a single case, hospitalization, ICU admission, or death, is a standard way to measure the effectiveness of any drug. It’s an important tool because it enables policymakers to evaluate tradeoffs between a new drug, a different existing drug, or doing nothing. In vaccine research the equivalent term is Number Needed to Vaccinate (NNTV, sometimes also written as NNV) in order to prevent a single case, hospitalization, ICU admission, or death (those are 4 different NNTVs that one could calculate).
Pharma HATES talking about NNTV and they hate talking about NNTV even more when it comes to COVID-19 vaccines because the NNTV is so ridiculously high that this vaccine could not pass any honest risk-benefit analysis.
Indeed about a year ago I innocently asked on Twitter what the NNTV is for coronavirus vaccines.
Pharma sent a swarm of trolls in to attack me and Pharma goons published hits pieces on me outside of Twitter to punish me for even asking the question. Of course none of the Pharma trolls provided an estimate of the NNTV for COVID-19 shots. That tells us that we are exactly over the target.
Various health economists have calculated a NNTV for COVID-19 vaccines.
-
Ronald Brown, a health economist in Canada, estimated that the NNTV to prevent a single case of coronavirus is from 88 to 142.
-
Others have calculated the NNTV to prevent a single case at 256.
-
German and Dutch researchers, using a large (500k) data set from a field study in Israel calculated an NNTV between 200 and 700 to prevent one case of COVID-19 for the mRNA shot marketed by Pfizer. They went further and figured out that the “NNTV to prevent one death is between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate.”
You can see why Pharma hates this number so much (I can picture Pharma’s various PR firms sending out an “All hands on deck!” message right now to tell their trolls to attack this article). One would have to inject a lot of people to see any benefit and the more people who are injected the more the potential benefits are offset by the considerable side-effects from the shots.
Furthermore, the NNTV to prevent a single case is not a very meaningful measure because most people, particularly children, recover on their own (or even more quickly with ivermectin if treated early). The numbers that health policy makers should really want to know are the NNTV to prevent a single hospitalization, ICU admission, or death. But with the NNTV to prevent a single case already so high, and with significant adverse events from coronavirus vaccines averaging about 15% nationwide, Pharma and the FDA dare not calculate an NNTV for hospitalizations, ICU, and deaths, because then no one would ever take this product (bye bye $93 billion in annual revenue).
Increased all cause mortality in the Pfizer clinical trial of adults
As Bobby Kennedy explains, Pfizer’s clinical trial in adults showed alarming increases in all cause mortality in the vaccinated:
In Pfizer’s 6 month clinical trial in adults — there was 1 covid death out of 22,000 in the vaccine (“treatment”) group and 2 Covid deaths out of 22,000 in the placebo group (see Table s4). So NNTV = 22,000. The catch is there were 5 heart attack deaths in the vaccine group and only 1 in placebo group. So for every 1 life saved from Covid, the Pfizer vaccine kills 4 from heart attacks. All cause mortality in the 6 month study was 20 in vaccine group and 14 in placebo group. So a 42% all cause mortality increase among the vaccinated. The vaccine loses practically all efficacy after 6 months so they had to curtail the study. They unblinded and offered the vaccine to the placebo group. At that point the rising harm line had long ago intersected the sinking efficacy line.
Former NY Times investigative reporter Alex Berenson also wrote about the bad outcomes for the vaccinated in the Pfizer clinical trial in adults (here). Berenson received a lifetime ban from Twitter for posting Pfizer’s own clinical trial data.
Pfizer learned their lesson with the adult trial and so when they conducted a trial of their mRNA vaccine in children ages 5 to 11 they intentionally made it too small (only 2,300 participants) and too short (only followed up for 2 months) in order to hide harms.
Estimating an NNTV in children ages 5 to 11 using Pfizer’s own clinical trial data
All of the NNTV estimates above are based on data from adults. In kids the NNTV will be even higher (the lower the risk, the higher the NNTV to prevent a single bad outcome). Children ages 5 to 11 are at extremely low risk of death from coronavirus. In a meta-analysis combining data from 5 studies, Stanford researchers Cathrine Axfors and John Ioannidis found a median infection fatality rate (IFR) of 0.0027% in children ages 0-19. In children ages 5 to 11 the IFR is even lower. Depending on the study one looks at, COVID-19 is slightly less dangerous or roughly equivalent to the flu in children.
So how many children would need to be injected with Pharma’s mRNA shot in order to prevent a single hospitalization, ICU admission, or death?
Let’s examine Pfizer’s EUA application and the FDA’s risk-benefit analysis. By Pfizer’s own admission, there were zero hospitalization, ICU admissions, or deaths, in the treatment or control group in their study of 2,300 children ages 5 to 11.
So the Number Needed to Vaccinate in order to prevent a single hospitalization, ICU admission, or death, according to Pfizer’s own data, is infinity. ∞. Not the good kind of infinity as in God or love or time or the universe. This is the bad kind of infinity as in you could vaccinate every child age 5 to 11 in the U.S. and not prevent a single hospitalization, ICU admission, or death from coronavirus according to Pfizer’s own clinical trial data as submitted to the FDA. Of course Pfizer likes this kind of infinity because it means infinite profits. [Technically speaking the result is “undefined” because mathematically one cannot divide by zero, but you get my point.]
Estimating an NNTV and risk-benefit model in children ages 5 to 11 using the limited data that are available
Everyone knows that Pfizer was not even trying to conduct a responsible clinical trial of their mRNA shot in kids ages 5 to 11. Pfizer could have submitted to the FDA a paper napkin with the words “Iz Gud!” written in crayon and the VRBPAC would have approved the shot. They are all in the cartel together and they are all looking forward to their massive payoff/payday.
But let’s not be like Pharma. Instead, let’s attempt to come up with a best guess estimate based on real world data. Over time, others will develop a much more sophisticated estimate (for example, Walach, Klement, & Aukema, 2021 estimated an NNTV for 3 different populations based on “days post dose”). But for our purposes here I think there is a much easier way to come up with a ballpark NNTV estimate for children ages 5 to 11.
Here’s the benefits model:
-
As of October 30, 2021, the CDC stated that 170 children ages 5 to 11 have died of COVID-19-related illness since the start of the pandemic. (That represents less than 0.1% of all coronavirus-related deaths nationwide even though children that age make up 8.7% of the U.S. population).
-
The Pfizer mRNA shot only “works” for about 6 months (it increases risk in the first month, provides moderate protection in months 2 through 4 and then effectiveness begins to wane, which is why all of the FDA modeling only used a 6 month time-frame). So any modeling would have to be based on vaccine effectiveness in connection with the 57 (170/3) children who might otherwise have died of COVID-related illness during a 6-month period.
-
At best, the Pfizer mRNA shot might be 80% effective against hospitalizations and death. That number comes directly from the FDA modeling (p. 32). I am bending over backwards to give Pfizer the benefit of considerable doubt because again, the Pfizer clinical trial showed NO reduction in hospitalizations or death in this age group. So injecting all 28,384,878 children ages 5 to 11 with two doses of Pfizer (which is what the Biden administration wants to do) would save, at most, 45 lives (0.8 effectiveness x 57 fatalities that otherwise would have occurred during that time period = 45).
-
So then the NNTV to prevent a single fatality in this age group is 630,775 (28,384,878 / 45). But it’s a two dose regimen so if one wants to calculate the NNTV per injection the number doubles to 1,261,550. It’s literally the worst NNTV in the history of vaccination.
If you inject that many children, you certainly will have lots and lots of serious side effects including disability and death. So let’s look at the risk side of the equation.
Here’s the risk model:
-
Because the Pfizer clinical trial has no useable data, I have to immuno-bridge from the nearest age group.
-
31,761,099 people (so just about 10% more people than in the 5 to 11 age bracket) ages 12 to 24 have gotten at least one coronavirus shot.
-
The COVID-19 vaccine program has only existed for 10 months and younger people have only had access more recently (children 12 to 15 have had access for five months; since May 10) — so we’re looking at roughly the same observational time period as modeled above.
-
During that time, there are 128 reports of fatal side effects following coronavirus mRNA injections in people 12 to 24. (That’s through October 22, 2021. There is a reporting lag though so the actual number of reports that have been filed is surely higher).
-
Kirsch, Rose, and Crawford (2021) estimate that VAERS undercounts fatal reactions by a factor of 41 which would put the total fatal side effects in this age-range at 5,248. (Kirsch et al. represents a conservative estimate because others have put the underreporting factor at 100.)
-
With potentially deadly side effects including myo- and pericarditis disproportionately impacting youth it is reasonable to think that over time the rate of fatal side effects from mRNA shots in children ages 5 to 11 might be similar to those in ages 12 to 24.
So, to put it simply, the Biden administration plan would kill 5,248 children via Pfizer mRNA shots in order to save 45 children from dying of coronavirus.
For every one child saved by the shot, another 117 would be killed by the shot.
The Pfizer mRNA shot fails any honest risk-benefit analysis in children ages 5 to 11.
Even under the best circumstances, estimating NNTV and modeling risk vs. benefits is fraught. In the current situation, with a new and novel bioengineered virus, where Pfizer’s data are intentionally underpowered to hide harms, and the FDA, CDC, & Biden Administration are doing everything in their power to push dangerous drugs on kids, making good policy decisions is even more difficult.
If the FDA or CDC want to calculate a different NNTV (and explain how they arrived at that number) I’m all ears. But we all know that the FDA refused to calculate an NNTV not because they forgot, but because they knew the number was so high that it would destroy the case for mRNA vaccines in children this age. Your move CDC — your own Guidance document states that you must provide this number.
Update: CDC finally mentions NNTV, but . . .
Toward the end of the six-hour CDC’s Advisory Committee on Immunization Practices (ACIP) Nov. 2 meeting where the committee voted to recommend Pfizer’s EUA vaccine for children 5 - 11, there was finally a mention of NNTV. It was on slide 36 of a presentation by CDC official D.r Sara Oliver. Unfortunately the CDC estimate was untethered from reality. I’ll explain:
Oliver claimed the NNTV to prevent a single case is 10, even though the best lower bound estimate is 88 and other estimates are 200 or higher (see calculations here and here).
Then she claimed the NNTV to prevent a single hospitalization is between 2,213 and 8,187. This is dishonest and a violation of scientific norms.
NNTV is calculated by dividing 1 by the Absolute Risk Reduction. There was no Absolute Risk Reduction in hospitalizations in the Pfizer clinical trial in kids 5 to 11, because no one was hospitalized in either the treatment or control group. 1/0 is “undefined” not 8,187.
Oliver made no estimate of NNTV to prevent a single COVID-19-related death because that is also undefined (again, there were no COVID-related deaths in the treatment or placebo group in the trial so the absolute risk reduction was zero).
Oliver also did not model injuries or deaths from the vaccine (she immuno-bridged from an older age group to show benefits but ignored the reported harms from the vaccine in the older age group).
I should also note that my estimates of NNTV were based on CDC data showing 170 deaths from COVID-19-related illness in kids ages 5 to 11 over the last 18 months (I got the number directly from the CDC COVID tracking website).
However at the ACIP meeting, the CDC said the number of children in this age group who have died of COVID-19-related illness is 94.
If 94 is the correct number to use, then the NNTV to prevent a single death from COVID-19 related illness in this age group would be 28,384,878 / 31 = 915,641. But it’s a two-dose regimen, so if one wants to calculate the NNTV-per-injection the number doubles to 1,831,282.
I imagine that at most, half of American parents will be foolish enough to inject this toxic product into their kids. At a 50% uptake rate, the ACIP decision to approve the Pfizer shot will likely kill 2,624 children via adverse reactions in order to potentially save 12 from COVID-19-related illness.
Now you know why the CDC did not release the meeting materials prior to the ACIP meeting — they could not stand up to any public scrutiny.
Update 11/05/21:
I see that El Gato Malo engaged in a similar set of calculations back in September when Pfizer first released its “results.” He faced the same challenges as I did — namely, there is no usable data from Pfizer and so one has to pull from others sources. He builds a steel man case (the most generous possible defense of the Pfizer product) and yet his results are still in line with mine (my numbers are higher though because I use a lower estimate of vaccine effectiveness and correct for VAERS underreporting). So again, even under the most generous assumptions, the Pfizer mRNA shot fails any honest risk benefit assessment in connection with children 5 to 11.

Author: MOS Medical Group – Eglise Bell

Since Tokyo summer Olympic Game ended on August 8, 2021, the urgent status of the pandemic as Japan is now in its worst surge of the COVID-19 pandemic since the onset of the crisis in such a megacity of 14 million. Most recently, a record number of new cases were reported at 20,140 on August 14. Deaths aren’t as high as successive waves of the pandemic from February 2021 to the end of May, but nerves are frayed with record numbers of infections. Dr. Ozaki, The chairman of the Tokyo Metropolitan Medical Association, recently led an emergency press conference on August 13, Dr. Haruo Ozaki shared those 18,000 new infections are reported daily. However, the death count has eased as compared to previous surges.

Image Credit: Novikov Aleksey / Shutterstock
How to deal with the current dilemma is a huge challenge to Japanese government and medical agencies? Fortunately, India has an excellent testimonial. Since April 28, India medical officials started providing Hydroxychloroquine and ivermectin to its massive population. As India is the major pharmaceutical manufacture in the world, they were ready for this massive drug distribution. Miraculously, COVID cases were plummeting quickly since then thanks to the new rules.

Much like what was successfully accomplished in India, parts of Bangladesh, and places like Argentina and Mexico, Chairman Ozaki calls for the immediate use of ivermectin as cases surge in Japan.
Dr. Ozaki declared that ivermectin has demonstrated significant benefits in reducing infections and deaths where the regimen is prophylactically administered for another indication. With the encouraging medical data from ivermectin clinical trials’ reports worldwide, especially the one from FLCCC of US and BIRD of UK, the head of the Metropolitan Medical Association declared that while clinical trials were important, it was time to greenlight doctors to prescribe ivermectin in association with giving the patient informed consent.
Finally,greenlight for Ivermectin is on in the first developing country since the start of the COVID-19 pandemic,giving hope to all countries and regions. Perhaps this time because Japan did not have the big Pharm entering the COVID vaccine market, the government did not get much pressure, so the Japanese government’s anti-epidemic policy basically reflects a normal democratic regime should do, that is, to protect the health of the people. Expect the miracle of ivermectin in India to happen again.
References:

Could the mystery be revealed here? Perhaps you may notice how this article artfully omits an obvious possibility.
TOKYO (AP) — Almost overnight, Japan has become a stunning, and somewhat mysterious, coronavirus success story.
Daily new COVID-19 cases have plummeted from a mid-August peak of nearly 6,000 in Tokyo, with caseloads in the densely populated capital now routinely below 100, an 11-month low.
The bars are packed, the trains are crowded, and the mood is celebratory, despite a general bafflement over what, exactly, is behind the sharp drop.
Japan, unlike other places in Europe and Asia, has never had anything close to a lockdown, just a series of relatively toothless states of emergency.
Some possible factors in Japan’s success include a belated but remarkably rapid vaccination campaign, an emptying out of many nightlife areas as fears spread during the recent surge in cases, a widespread practice, well before the pandemic, of wearing masks and bad weather in late August that kept people home.
But with vaccine efficacy gradually waning and winter approaching, experts worry that without knowing what exactly why cases have dropped so drastically, Japan could face another wave like this summer, when hospitals overflowed with serious cases and deaths soared — though the numbers were lower than pre-vaccination levels.
Many credit the vaccination campaign, especially among younger people, for bringing infections down. Nearly 70 percent of the population is fully vaccinated.
“Rapid and intensive vaccinations in Japan among those younger than 64 might have created a temporary condition similar to herd-immunity,” said Dr. Kazuhiro Tateda, a Toho University professor of virology.
Tateda noted that vaccination rates surged in July to September, just as the more infectious delta variant was spreading fast.
He cautioned, however, that breakthrough infections in the U.S., Britain and other places where inoculations began months earlier than in Japan show that vaccines alone are not perfect and efficacy gradually wears off.
Japan’s vaccinations started in mid-February, with health workers and the elderly first in line. Shortages of imported vaccines kept progress slow until late May, when the supply stabilized and daily inoculation targets were raised to above 1 million doses to maximize protection before the July 23-Aug. 8 Olympics.
The number of daily shots rose to about 1.5 million in July, pushing vaccination rates from 15% in early July to 65% by early October, exceeding the 57% of the United States.
Daily new cases surged just weeks ahead of the Olympics, forcing Japan to hold the Games with daily caseloads of more than 5,000 in Tokyo and around 20,000 nationwide in early August. Tokyo reported 40 cases Sunday, below 100 for the ninth straight day and lowest this year. Nationwide, Japan reported 429 cases Sunday for an accumulated total of about 1.71 million and 18,000 deaths since the pandemic began early last year.
So why the drop?
“It’s a tough question, and we have to consider the effect of the vaccinations progress, which is extremely big,” said Disease Control and Prevention Center Director Norio Ohmagari. “At the same time, people who gather in high-risk environments, such as crowded and less-ventilated places, may have been already infected and acquired natural immunity by now.”
Though some speculated that the drop in cases might be due to less testing, Tokyo metropolitan government data showed the positivity rate fell from 25% in late August to 1% in mid-October, while the number of tests fell by one-third. Masataka Inokuchi, the Tokyo Medical Association deputy chief, said falling positivity rates show infections have slowed.
Japan’s state of emergency measures were not lockdowns but requests that focused mainly on bars and eateries, which were asked to close early and not serve alcohol. Many people continued to commute on crowded trains, and attended sports and cultural events at stadiums with some social distancing controls.
The emergency requests have ended and the government is gradually expanding social and economic activity while allowing athletic events and package tours on a trial basis using vaccination certificates and increased testing.
To speed up inoculations, former Prime Minister Yoshihide Suga, who left office recently, expanded the number of health workers legally eligible to give shots, opened large-scale vaccination centers and promoted workplace vaccinations beginning in late June.
Kyoto University professor Hiroshi Nishiura told a recent government advisory board meeting that he estimates vaccinations helped some 650,000 people avoid infection and saved more than 7,200 lives between March and September.
Many experts initially blamed younger people, seen drinking on the streets and in parks when the bars were closed, for spreading the virus, but said data showed many in their 40s and 50s also frequented nightlife districts. Most serious cases and deaths were among unvaccinated people in their 50s or younger.
Takaji Wakita, director of the National Institute of Infectious Diseases, told reporters recently he is worried people have already resumed partying in nightlife districts, noting that the slowing of infections may have already hit bottom.
“Looking ahead, it is important to further push down the caseloads in case of a future resurgence of infections,” Wakita said Thursday.
On Friday, new Prime Minister Fumio Kishida said a preparedness plan to be compiled by early November would include tougher limits on activities and require hospitals to provide more beds and staff for COVID-19 treatment in case infections soar in a “worst-case scenario.”
He did not elaborate on details.
Many people are cautious about letting down their guard, regardless of the numbers.
Mask-wearing “has become so normal,” said university student Mizuki Kawano. “I’m still worried about the virus,” she said.
“I don’t want to get close to those who don’t wear masks,” said her friend, Alice Kawaguchi.
Public health experts want a comprehensive investigation into why infections have dropped off.
An analysis of GPS data showed that people’s movements in major downtown entertainment districts fell during the most recent, third state of emergency, which ended Sept. 30.
“I believe the decrease of people visiting entertainment districts, along with the vaccination progress, has contributed to the decline of infections,” said Atsushi Nishida, the director of the Research Center for Social Science & Medicine Sciences at the Tokyo Metropolitan Institute of Medical Science.
But people headed back to entertainment districts as soon as the recent emergency ended, he said, and that may “affect the infection situation in coming weeks.”
By MARI YAMAGUCHI October 18, 2021
AP journalist Chisato Tanaka contributed to this report.
Is it so, as some wags say, that industry no longer makes money; only finance does? That’s been the operating theory for much of the West lately. Of course, that invites the question: what then is finance supposed to finance… that is, put money into? Why… industry, of course, and in the broadest sense of the word: the production of goods… goods being things that have value (that’s what’s good about them). How quaint! But most of the industry that used to be here has gone to other lands.
What about all that money (capital) flowing into technology: Facebook, Google, Amazon? Hmmmm. What does Facebook produce, besides conflict between its users? Okay, it harvests data about them to sell to advertisers. And what are the advertisers advertising? Their products. Who produces the products? Mostly those people in other lands. Facebook users, then, are increasingly not employed, at least not in the production of goods. Perhaps in services like nursing, trucking, garbage pickup, food prep, police, firemen, prison guards, government bureaucracy (is that a service or a dis-service?) and et cetera.
Anyway, those service people are being fired left-and-right now because they refuse to be coerced into taking a vaccine that was never properly tested and has many scary side-effects. By the way, as of Sunday, the “newspaper-of-record” (The New York Times) finally had to come clean, after months of whistling past the graveyard, and admit what the public already knows: mRNA vaccines are dangerous:

While we’re on the subject, what does Google produce? Supposedly, answers to questions, plus, like Facebook, it harvests information about the people who ask the questions and then sells the info, blah blah. And whutabout Amazon? Don’t they sell a lot of products? Yeah, mostly produced by those people in other lands. What Amazon really produces is a phenomenal amount of motion — trucks going hither and thither, at increasing cost now as the price of gasoline and diesel fuel shoots up. To me, that looks like a problem for Amazon’s business model. Another problem is the growing number of people without gainful employment who have little money to buy stuff from Amazon, wherever it comes from.
That last problem has been papered-over for two years by “helicopter money” from the federal government — direct payment to the people for doing nothing, producing neither goods nor services. This has been an impressive trick. The money comes from nowhere and for nothing. The trick is based on simple accounting fraud. The second law of thermodynamics, a.k.a. entropy, suggests that eventually this process will degrade the value of the money (or “money”) issued by the fraudsters.
The hand in play for the moment is the spending legislation proposed by “Joe Biden.” It would generate a whole helluva lot more helicopter money from nowhere for nothing, and would theoretically keep the game going a little bit longer — except the process will only generate more unwanted entropy, causing decay in the value of that “money” and canceling the desired effect of spreading it around. That’s called inflation. If the value of money drops hard and fast, that is called hyperinflation. It would be politically and socially devastating, and probably lead to the downfall of the government. The net effect would be a nation bankrupt at all levels and that will segue into an epic economic depression.
If the legislation doesn’t get passed, the USA will perhaps skip the hyperinflationary intermezzo and move straight into a deflationary depression, which is what you get when nobody has any money. When that happens, especially in a system with money actually based on debt-creation, debts do not get paid (mortgages, car payments, credit cards, perhaps even coupons on US Treasury bonds), and when debts are not paid, money disappears. Poof! No money! It’s a vicious cycle. The more money disappears the more money keeps disappearing. None of this bodes well for the winter ahead.
Add to that the growing breakdown in global trade operations. Even many of those goods produced in other lands aren’t making it to the docks, and the reduced flow of goods that happened to already land on the docks can’t get unloaded and delivered to its various destinations because of disruptions in the US trucking sector. To some degree, those disruptions are caused by bonehead government regulations, especially in California, where most of the stuff from Asia lands. The bonehead regulations (like, outlawing trucks more than three years old) can be thought of as typical government “dis-services.”
Now add to that the rising cost of oil, natural gas, and coal — the global economy’s primary resources — and disruptions in the industries that produce these vital resources and you’ve got another layer of disorder being introduced into the system (entropy again). For the moment, government propaganda tries to divert your attention to a possible shortage of Christmas presents as the nation’s main concern. Don’t be fooled. It’s more about total systemic economic breakdown, as in US citizens having no heat and no food. Also, no gasoline and no parts for fixing broken cars (and trucks).
Do you suppose the capital markets will keep rising as all this spins out? I would suppose that the capital markets will lose 80 to 90 percent of their value when all is said and done. The fabled “One Percent” will finally feel the pain that was previously distributed among the rest of us. Don’t make the mistake of thinking the One Percent can control the situation. They are mere Wizards of Oz, barfing into their laptops. If working-from-home wasn’t a thing, they’d be jumping out of windows on Wall Street.
It’s a grim outlook, I admit, but you could see it coming over the horizon from a thousand miles away. Where I differ from other observers is that I doubt that any sort of extreme government surveillance state can be imposed on the public under these conditions. The people will be too pissed-off and, anyway, the current regime will be broke and out of mojo — possibly to the degree that it has to be shoved aside. “Let’s Go Brandon” is serious business. It’s the end of something.
In the background lurks this virus thing, and the insane vaccination program it prompted. We know that people have been harmed by the vaccinations, but not how many people altogether will be affected moving forward. The possibility, though, is for a nation both broke and sick struggling to get through a dark passage of history. Stay nimble, stay local, stay reality-based, be helpful, be honest, be brave, and be kind to each other. We’ll get through it.