Monthly Shaarli
September, 2021
Friday September 17, 2021
University of Guelph
50 Stone Rd. E.
Guelph, ON, N1E 2G1
Dear Dr. Charlotte A.B. Yates, President and Vice-Chancellor,
I will forewarn you that this is a lengthy letter. However, it only represents a fraction of the information that I would like to be able to share with you. I have found it necessary to write this so you can fully understand my perspective. With my life and that of my family, many friends and treasured colleagues being destroyed under your watch, I figure the least you can do is read and consider this very carefully. It is incredible to note that many, if not most, of my on-campus detractors have judged me without reading any of my scientific arguments or talking to me about them.
The COVID-19 Vaccine Mandate at the University of Guelph
You issued a mandate that everyone within the University of Guelph community must receive a COVID-19 vaccine. I have spent most of my lifetime learning to be a very deep and critical thinker and to follow the weight of scientific evidence. I am a well-recognized expert in vaccinology. As per my extensive funding, research, publication, and teaching records, I am a vaccine lover and an innovator in this field. I promote highly effective vaccines that have undergone extensive, rigorous, and proper safety testing as the most efficient type of medicines that exist. Vaccines that meet these criteria have prevented a vast amount of mortality and morbidities around the world. However, I could not be in stronger disagreement with you forcing the current COVID-19 vaccines upon everyone who is part of our campus community. I respect the challenges that a university president faces when trying to manage a large and dynamic academic institution. However, your roots are as a scholar. As a publicly funded institution of advanced learning, it is incumbent on us to demonstrate an ability to view the world around us in a constructively critical fashion such that we can improve the lives of others. We should be able to do this free of political or financial pressures and without bias or prejudice or fear of censorship and harassment. As a viral immunologist that has been working on the front lines of the scientific and medical community throughout the duration of the declared COVID-19 pandemic, I feel compel ed to speak on behalf of the many who will not, due to extreme fear of retribution. We now live in a time when it is common practice for people to demand and expect to receive confidential medical information from others. I will not be coerced into disclosing my private medical information. However, for the sake of highlighting some of the absurdities of COVID-19 vaccine mandates I choose, of my own free will, to freely disclose some of my medical information here…
Those with Naturally Acquired Immunity Don’t Need to be Vaccinated and are at Greater Risk of Harm if Vaccinated
I participated in a clinical trial that has been running for approximately 1.5 years. The purpose is to develop a very sensitive and comprehensive test of immunity against SARS-CoV-2; in large part to inform the development of better COVID-19 vaccines (https://insight.jci.org/articles/view/146316 ). My personal results prove that I have naturally acquired immunity against SARS-CoV-2. With this test, spots indicate a positive result for antibodies against a particular part of the virus. Darker spots correlate with more antibodies. Antibody responses correlate with the induction of memory B cells. Antibodies will wane over time, but B cells can survive for many years and rapidly produce massive quantities of antibodies upon re-exposure to a pathogen. On the following page are my results, along with a map of which part of the virus each spot represents…


The dark spot at position D26 is the positive control and indicates that the assay worked. My results demonstrate that I have broad immunity against multiple components of SARS-CoV-2, including the spike protein. Importantly, spot B26 shows that I have antibodies against the membrane protein. This protein is not highly conserved across coronaviruses. As such, it provides evidence that I was infected with SARS-CoV-2. Note that I was sick only once since the pandemic was declared. It was a moderately severe respiratory infection that took four weeks to recover from. The SARS-CoV-2 PCR test was negative, despite being run at an unreasonably high number of cycles. This suggests that I was one of the many for whom SARS-CoV-2 has proven to be of low pathogenicity or not even a pathogen (i.e. no associated disease).
There is a plethora of scientific literature demonstrating that naturally acquired immunity against SARS-CoV-2 is likely superior to that conferred by vaccination only. Indeed, it is much broader, which means that emerging variants of SARS-CoV-2 will have more difficulty evading it as compared to the very narrow immunity conferred by the vaccines. Importantly, the duration of immunity (i.e. how long a person is protected) has proven to be far longer than that generated by the current vaccines. The duration of immunity for the mRNA-based COVID-19 vaccines appears to be a horrifically short 4.5 months. I actually wrote a lay article back in February 2021 to explain why a vaccine of this nature would fail to be able to achieve global herd immunity on its own (https://theconversation.com/5-factors-that-could-dictate-the-success-or-failure-of-the-covid-19-vaccine-rollout- 152856). This is why places like Canada, the USA, and Israel have found it necessary to roll out third doses. And now there is talk (and a commitment in Israel) to roll out fourth doses (yes, that’s four doses within one year). The World Health Organization recognized the value of natural immunity quite some time ago. Unfortunately, in Canada and at the University of Guelph, we have failed to recognize that the immune system works as it was designed to. Its ability to respond is not limited solely to vaccines.
Here are some references to support this: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Natural_immunity-2021.1; https://academic.oup.com/jid/advance-article/doi/10.1093/infdis/jiab295/6293992; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7803150/.
As someone who develops vaccines, I can tell you that it is difficult to make a vaccine that will perform as poorly as the current COVID-19 vaccines. Indeed, most vaccines given in childhood never require a booster shot later in life. The take-home message here is that people like me, who have naturally acquired immunity, do not need to be vaccinated. Nor is it needed to protect those around the person who already has immunity. Worse, research from three independent groups has now demonstrated that those with naturally acquired immunity experience more severe side-effects from COVID-19 vaccines than those who were immunologically naïve prior to vaccination (https://www.thelancet.com/journals/eclinm/article/PI S2589- 5370(21)00194-2/fulltext; https://www.medrxiv.org/content/10.1101/2021.04.15.21252192v1; https://www.medrxiv.org/content/10.1101/2021.02.26.21252096v1). In other words, for those with natural immunity, vaccination is not only unnecessary, but it would put them at enhanced risk of harm. Knowing this, nobody should ever mandate COVID-19 vaccination. Instead, it would be in the best interest of helping everyone make the most informed health decisions for themselves to make voluntary testing for immunity available.
Testing for Natural y Acquired Immunity was a Viable Option but was Ignored
You and the provost met with me and two other colleagues back in March 2021 and we presented the opportunity for the University of Guelph to show leadership and offer testing for immunity to our campus community in support of a safe return to in-person teaching and learning. You embraced this idea with enthusiasm and promised to move forward with it. This did not materialize so one of my colleagues contacted you. Once again, you agreed it was an excellent idea and that you would move forward with it. Nothing happened. So, my two colleagues and I met with one of our vice-presidents in May 2021. They also thought that making an antibody test available was an excellent idea and promised to work on getting it implemented on campus. Nothing materialized. They were contacted again by one of my colleagues. There was no response. There is no excuse for forcing vaccines on people, especially after having been given the opportunity to implement testing for immunity and refusing to do so.
The University of Guelph won’t pay for me to receive a booster vaccine against rabies unless I can demonstrate that my antibodies are below what has been deemed to be a protective titer. This is because it would not be appropriate to give me a vaccine that is not without risk if I don’t need it. Also, the university does not want to pay the $850 cost of the vaccination regimen unless I absolutely need it. In short, you will not allow me to receive that booster vaccine without first evaluating me on an annual basis for evidence of immunity (or lack thereof). So why was this principle rejected for the SARS-CoV-2 vaccines, for which there is vastly less reliable safety data available, and none for the long-term? Canada should have been acquiring data about immunity starting a long time ago. It is a particularly poor precedent for a university to reject the concept of acquiring data that could inform safer and more effective COVID-19 policies. Immunity testing would even benefit vaccinated individuals. It is well known that responses to vaccines in outbred populations follows a normal curve and includes individuals that are non-responders (i.e. they are left without immunity and are, therefore, unprotected following vaccination) and low-responders (insufficient protection). In fact, this concept has been the focus of an internationally recognized research program on our campus that has brought many accolades and awards to our institution.
You have banned me from campus for at least the next year. I can show proof of immunity against SARS-CoV-2 but you will not allow me to enter buildings. But someone else can show a receipt saying that someone saw two needles go into their arm and you will allow them to enter. You actually have no idea if that person has immunity. There have even been reported cases of people accidental y or even intentionally (e.g. a case in Germany) being administered saline instead of the vaccine. Does it make sense to ban someone who is immune from campus but al ow people who are presumed, but not confirmed, to be immune? This is a scenario that you have created. As a fellow academic, I am requesting that you provide me with a strong scientific rationale why you are al owing thousands with an unconfirmed immunity status onto our campus, but you are banning people like me who are known to have immunity. Further, please explain how you feel it is ethical to force COVID-19 vaccines on people who are uncomfortable with being coerced when you do not know their immunity status. Despite attempts to halt the spread of SARS-CoV-2 via masking and physical distancing, the reality is that the virus has not complied with these attempts to barricade it. Indeed, it has infected many people across Canada, many of whom may not have even realized it because it is not a dangerous pathogen for them. From the perspective of a medical risk-benefit analysis, this is a no-brainer. A medical procedure that adds no value but carries known and still-to-be-defined risks should never be mandated!
The University Back-Tracked on Advice from its Own Legal Counsel
I, along with two colleagues, attended a meeting with one of our vice-presidents in May 2021. In that meeting the legal advice that was provided to the University of Guelph was disclosed. We were told this included making COVID-19 vaccines voluntary, that nobody on campus should be made to feel coerced into being vaccinated, and that nobody should feel pressured to disclose their vaccination status. On this basis, I was to serve as one of the on- campus faculty contacts for anyone who experienced any of these issues. Did Canada’s laws change during the summer in a way that rendered this legal advice no longer valid? Now I am having to spend an inordinate amount of time trying to help the many people whose lives have imploded due to the university’s vaccine mandate.
I am a Scientist Who is Knowledgeable and Values Integrity Despite What So-Cal ed ‘Fact Checkers’ Have Claimed
There are many on our campus who repeatedly put my name out to the public with claims that I disseminate misinformation. Not one of these individuals has ever given me the courtesy of a conversation prior to publicly attacking me. None of them will engage me in public discussions of the science to allow people to judge the legitimacy, or lack thereof, of what I am saying. Censorship on our campus has become as prevalent as it is off- campus. My detractors, rather than showing a deep understanding of the science underlying COVID-19 vaccines, continually refer to the so-cal ed ‘fact checks’ that have been posted about me. Let me tell you some things about the so-called ‘fact checkers’. Firstly, they give scientists and physicians of integrity unreasonably short periods of time to respond to their requests for answers. For example, as I write this letter, I have 13,902 unread messages in my inbox and my voice mail is at maximum capacity. I have yet to see a ‘fact check’ request prior to its expiry, which remarkably, is often within mere hours of an e-mail being sent. This is an unreasonable expectation from a busy professional. Also, many ‘fact checkers’ lack sufficient expertise. In some cases, ‘fact checker’ sites have had to rely on postdoctoral trainees in other countries to write responses.
Most of the harassment against me began after ‘fact checkers’ cherry-picked one short radio interview that I gave to a lay audience. Some have accused me of only giving half the story in that interview. They were most kind; I was only able to reveal 0.5% of the story. It is unfair to critique a tiny portion of one’s arguments that were presented off-the-cuff to a lay audience with no opportunity for me to respond in real-time. For your information, I have rebutted every single one of the ‘fact checks’ that I am aware of in various public interviews. Let me give you one example that some of our colleagues on our campus have repeatedly misused while harassing me in social media…
One of the many issues that I have raised with the vaccines is that should a reasonable concentration of the free spike protein get into systemic circulation, it could potentially harm the endothelial cells lining our blood vessels. I cited this study: https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902. The authors were contacted, and they claimed I had misinterpreted the study. They said that spike-specific antibodies would mop up any spike proteins in the blood, thereby protecting the blood vessels. They argued that this demonstrated that vaccinating people against the spike protein is a good thing.
However, the authors are not immunologists and they failed to recognize the limitations of their own study in drawing these kinds of conclusions. Specifically, they did not recognize that in a naïve individual receiving a mRNA-based COVID-19 vaccine, there are no antibodies; either pre-existing in the host, or in the vaccine formulation. In fact, it will take many days for the antibody response to be induced and for titers to begin reaching substantial concentrations. This leaves a large window of time in which any free spike proteins could exert their biological functions/harm in the body before there are any antibodies to neutralize them. Worse, most of the spike proteins should be expressed by our own cells. In that case, the antibodies will target and kill them in a form of autoimmunity. The authors of the paper forgot that their model was in the context of natural infection, where vaccination would precede exposure to SARS-CoV-2. In that case, I agree that there would be pre-existing antibodies that could neutralize spike proteins of viral origin entering the circulation. This was perceived to be one of the ‘strongest’ arguments used by others to try to discredit me. The reality is that it is completely incorrect and represents an embarrassing misinterpretation by the authors of the original paper and the many ‘fact-checkers’ that believed them without question.
Criminal Harassment
You have allowed colleagues to harass me endlessly for many consecutive months. They have lied about me, cal ed me many names, and have even accused me of being responsible for deaths. I submitted a harassment claim and your administrators ruled that it did not meet the bar of civil harassment. In stark contrast, I have been contacted by members of off-campus policing agencies who have told me that it exceeds the minimum bar of criminal harassment. I am sorry, but a faculty member can only take so much bullying and see such a lack of adherence to scientific and bioethical principles before it becomes necessary to speak up. Under your watch, you have allowed my life to be ruined by turning a blind eye to on-campus bullying, ignoring our campus principles of promoting mental well-being and a workplace in which I can feel safe. In addition to this you have banned me from the campus because I have robust, broadly protective, and long-lasting immunity against SARS-CoV-2 but lack a piece of paper suggesting that it was obtained via two injections.
Did you see this front page of one of Canada’s major newspapers?

…remarkably, the on-campus COVID-19 policies you are promoting fuel this kind of pure hatred from people, most of whom have not confirmed their own immunity status, against someone like me who is immune to SARS-CoV-2!!! Does that make any sense? My workplace has become a poisoned environment where the bullying, harassment, and hatred against me have been incessant. Are you ever going to put an end to the childish and irrational behaviours being demonstrated by our colleagues? I have received thousands of emails from around the world that indicate the university should be embarrassed and ashamed to allow such childish behaviour from faculty members to go unchecked in front of the public.
I have invested a decade of my life into the University of Guelph. I have conducted myself professionally and worked to an exceptional y high standard. I have consistently received excellent ratings for my research, teaching, and service. I have received rave reviews from students for my teaching. I have received prestigious research and teaching awards. I have brought funding to our campus from agencies that had never partnered with the University of Guelph in our institution’s history. I have brought in
$1 million-worth of equipment to improve our infrastructure, etc., etc. I am a man of integrity and a devoted public servant. I want to make Canada a better place for my family and for my fellow Canadians. We are a public institution. My salary is covered by taxpayers. This declared pandemic involves science that is in my ‘wheelhouse’. Since the beginning, I have made myself available to answer questions coming from the public in a fashion that is unbiased and based solidly on the ever-exploding scientific literature. My approach has not changed. Has some of it contradicted the very narrow public health narrative carried by mainstream media? Yes. Does that make it wrong? No. I will stand by my track record. When Health Canada authorized the use of AstraZeneca’s vaccine I, along with two colleagues, wrote an open letter requesting that this vaccine not be used, in part on the grounds that it was being investigated for a link to potentially fatal blood clots in many European countries. I was accused at that time by so-called ‘fact checkers’ of providing misinformation. Less than two months later, Canada suspended the AstraZeneca vaccination program because it was deemed to be too unsafe as a result of causing blood clots that cost the unnecessary loss of lives of Canadians. More recently, I was heavily criticized for raising concerns in a short radio interview about a potential link between the Pfizer BioNTech COVID-19 vaccine and heart inflammation in young people, especially males. This is now a well recognized problem that has been officially listed as a potential side-effect of the mRNA COVID-19 vaccines. It was also the subject of a recent Public Health Ontario Enhanced Epidemiological Summary Report highlighting the increased risk of myocarditis and pericarditis to young males following COVID-19 mRNA vaccination. As such, I have a proven track record of accurately identifying concerns about the COVID-19 vaccines.
A Lack of Safety Data in Pregnant Females as Another Example of Why Vaccines Should Not be Mandated
I would like to give another disconcerting safety-related example of why a COVID-19 vaccine mandate could be dangerous. We have pregnant individuals or those who would like to become pregnant on campus. There was a highly publicized study in the prestigious New England Journal of Medicine that formed the foundation of declaring COVID-19 vaccines safe in pregnant females (https://www.nejm.org/doi/ful /10.1056/nejmoa2104983). The authors of this study declared that there was no risk of increased miscarriage to vaccinated females. This study resulted in many policies being instituted to promote vaccination of this demographic, for which the bar for safety should be set extremely high.
Did you know that this apparent confirmation of safety had to be rescinded recently because the authors performed an obvious mathematical error? I witnessed several of my colleagues from Canada and other countries bravely push for a review of this paper under withering negative pressures. Once the editor finally agreed to do so, the authors had no choice but to admit that made a mathematical error. Most of the world does not realize this. This admission of using an inappropriate mathematical formula can be found here: https://www.nejm.org/doi/ful /10.1056/NEJMx210016. This means that the major rationale for declaring COVID-19 vaccines safe in pregnant females is gone! How can someone force a COVID-19 vaccine on a pregnant female when there are insufficient safety data available to justify it?
Advocating for the Vulnerable and Those Fearful of Retribution
My concern is not primarily for myself. I am using my case to highlight how wrong your vaccine mandate is. I am more concerned for the more vulnerable on our campus. I hold tenure, and if ever there was a time when this was important, it is now. However, I have had to bear witness to numerous horrible situations for students and staff members. Students have been physically escorted off our campus, sometimes being removed from their residence, sometimes with their parents also being escorted off. Staff members have been escorted off campus and immediately sent home on indefinite leaves without pay, leaving them unable to adequately care for their families.
In many of these situations it seemed like the interactions intentionally occurred in very public settings with it being made clear to all onlookers that the person or people were not vaccinated. Parents have been denied attending meetings with their children who are entering the first year of a program. They recognize that adult learners would normally not have their parents accompany them, but we are living in unusual times with excessive and unfair (arguably illegal?) pressures being applied and these parents are entitled to advocate and defend the best interests of their sons and daughters.
Many students have deferred a year in the desperate hope that our campus community will not be so draconian next year. Others fought hard to earn their way into very competitive programs and are not being guaranteed re-entry next year. Many faculty members refused to offer on-line learning options for those who did not wish to be vaccinated.
On the flip-side, there are also faculty members, like many students and staff, who are completely demoralized. This includes some who were happily vaccinated but are upset by the draconian measures of your COVID-19 policies and/or will be unwilling to receive future booster shots. I can tell you many stories of students and staff members who couldn’t resist the pressure to get vaccinated because they were losing vast amounts of sleep and experiencing incredible anxiety and were on the verge of mental and/or physical breakdowns. In some of these cases, they were crying uncontrollably before, during, and after their vaccination, which they only agreed to under great duress. This does not represent informed consent!
I have had several members of our campus community contact me with concerns that they may have suffered vaccine-induced injuries ranging from blood clots to chest pain to vision problems to unexpected and unusual vaginal bleeding. Can I prove these were due to the vaccine? No. But can anyone prove they were not? No. And it is notable that these are common events reported in adverse event reporting systems around the world. In all cases, the attending physicians refused to report these events, even though it is supposed to be a current legal requirement to do so. These people obediently got vaccinated and were then abandoned when they became cases that did not help sell the current public health messaging.
A World Where Everyone is Vaccinated Looks Nothing Like Normal
The two-week lockdown that was supposed to lead into learning to live with SARS-CoV-2 has turned into the most mismanaged crisis in the history of our current generations. I ask you to look around with a very critical eye. You just reported that 99% of the campus community is vaccinated. Congratulations, you have far exceeded the stated standard for what is apparently the new goal of ‘herd vaccination’. I cannot use the typical term ‘herd immunity’ here because immunity is not being recognized as legitimate; only inferred immunity based on receiving two needles counts. We were told that achieving herd immunity by vaccination alone was the solution to this declared pandemic. This has been achieved on our campus in spades. I sat in on our town hall meetings with our local medical officer of health who confidently told us that the risk of breakthrough infections in the vaccinated was almost zero. Why, then are people so petrified of the unvaccinated. Look at vaccines for travellers going to exotic locations.
These are vaccines of some quality. Travellers take these vaccines, and not only do they not avoid the prospective pathogen, but they happily travel to the location where it is endemic (i.e. they enthusiastically enter the danger zone because they are protected). So, what does our campus look like with almost every person vaccinated? Everyone must remain masked and physically distanced. There is no gathering or loitering allowed in stairwells or any open spaces in buildings or outside. People are still being told which doors to enter and exit, when they can do so, where to stand in line, when to move. Incredibly, time restrictions are even being implemented in some eating areas because some students were deemed to be “snacking too long” with their masks off and, therefore, putting others at risk of death. In short, the on-campus COVID-19 policies are even more draconian than they were last year, but everyone is vaccinated. It doesn’t seem like the vaccines are working very well when a fully vaccinated campus cannot ease up on restrictions.
But, of course, we already know how poorly these vaccines are performing. Based on fundamental immunological principles, parenteral administration of these vaccines provides robust enough systemic antibody responses to allow these antibodies to spill over into the lower respiratory tract, which is a common point at which pathogens can enter systemic circulation due to the proximity of blood vessels to facilitate gas exchange. However, they do not provide adequate protection to the upper respiratory tract, like natural infection does, or like an intranasal or aerosolized vaccine likely would. As such, people whose immunity has been conferred by a vaccine only are often protected from the most severe forms of COVID-19 due to protection in the lower lungs, but they are also susceptible to proliferation of the virus in the upper airways, which causes them to shed equivalent quantities of SARS-CoV-2 as those who completely lack immunity. Dampened disease with equal shedding equals a phenotype that approaches that of a classic super-spreader; something that we erroneously labelled healthy children as until the overwhelming scientific evidence, which matches our historical understanding, clarified that this was not the case.
I have been in meetings where faculty have demanded to know who the unvaccinated students will be in their classes so they can make them sit at the back of the classroom! I can’t believe that some of my colleagues are thinking of resorting to the type of segregation policies that heroes like Viola Desmond, Rosa Parks, Martin Luther King Jr., Carrie M. Best, and Lulu Anderson fought so hard against so many years ago.
The Exemption Fiasco
With respect to exemptions for COVID-19 vaccines, the University of Guelph provided a number based on creed or religion but then, remarkably, rescinded these. These previously exempt individuals were required to resubmit applications using a more onerous form; many that had been honoured previously were rejected upon re- submission. Many have been rejected since. Based on the reports I have received from many people these rejections of exemption requests were typically not accompanied by explanations. Nor have many been told, despite asking, who it is that sits on the committee making decisions about these exemptions.
I would never be allowed to assign marks to students anonymously, nor without being able to justify them. Yet there seems to be a lack of transparency with exemptions and many of these decisions are destroying people’s lives; the outcomes are not trivial. Could you please disclose the names of the people serving on the University of Guelph’s committee that reviews exemptions? Also, could this committee please provide to applicants, retroactively, comments to justify their decisions? I have even heard it said in recent meetings that a lot of people are happy to hear that exemptions, including some medical exemptions are being denied. Why are our faculty celebrating refusals of medical exemptions for students?
A Lack of Consultation with the Experts on Vaccines
You have stated on numerous occasions that your COVID-19 policies have only been implemented after extensive consultation with local and regional experts. Interestingly, however, you have refused, for some unknown reason, to consult with any of the senior non-administrative immunologists on your campus. I would like to remind you that vaccinology is a sub-discipline of immunology. Notably, all three of us have offered repeatedly to serve on COVID-19 advisory committees, both on-campus and for our local public health unit, which also lacks advanced training in immunology and virology. The three of us have stayed on top of the cutting-edge scientific findings relevant to COVID-19 and meeting regularly with many national and international collaborative groups of scientists and physicians to debate and discuss what we are learning. I think it is notable that the senior non-administrative immunologists unanimously agree that COVID-19 vaccines should not be mandated for our campus based on extensive, legitimate scientific and safety reasons.
Mandating COVID-19 Vaccines is Criminal
I am no legal expert but have consulted with many lawyers who have told me that these vaccine mandates break many existing laws. Here is one example copied from the Criminal Code of Canada: Extortion • 346 (1) Every one commits extortion who, without reasonable justification or excuse and with intent to obtain anything, by threats, accusations, menaces or violence induces or attempts to induce any person, whether or not he is the person threatened, accused or menaced or to whom violence is shown, to do anything or cause anything to be done. In your case, you are demanding that members of our academic community submit to receiving a COVID-19 vaccine against their will (a medical procedure that may very well be unnecessary and carry enhanced risk of harm) or face banishment from the campus. Again, I am not an expert in this area, but I am confident there will be lawyers willing to test this in court. Those responsible for issuing vaccine mandates will need to decide how confident they are that they will not lose these legal battles.
Integrity of Teaching
In this new world where followers of scientific data are vilified, I also worry about my ability to teach with integrity. Unbelievably, the Minister of Health of Canada, Patty Hajdu, told Canadians that vitamin D being a critical and necessary component of the immune system in its ability to clear intracellular pathogens like SARS-CoV-2 is fake news! Do you now that I have taught all my students about the importance of vitamin D (often in the historical context of how it was discovered as being critical for positive outcomes in patients with tuberculosis that were quarantined in sanatoriums).
I also teach the concept of herd immunity, with vaccination being a valuable tool to achieve this. I do not teach the concept of ‘herd vaccination’ while promoting ignorance of natural immunity. There are other basic immunological principles that I teach that have either not been recognized during the pandemic as legitimate scientific principles or they have been altogether contradicted by public health and/or government officials. Will I still be allowed to teach immunology according to the decades of scientific information that I have built my course upon? Or will I be disciplined for teaching immunological facts? There are many attempts to regulate what I can and cannot say these days, so these are serious questions.
Instilling Fear of a Minority Group Breeds Hatred
We live in an era where issues of equity, diversity, and inclusion are supposed to be at the forefront of all discussions at academic institutions. However, you are openly discriminating against and excluding a subset of our community that happens to be highly enriched with people engendered with critical thinking; a quality that we are supposed to be nurturing and promoting. With COVID-19 mandates, an environment has been created on our university campus that promotes hatred, bullying, segregation, and fear of a minority group whose only wrongdoing has been to maintain critical thinking and decision-making that is based on facts and common sense. I have yet to meet an anti-vaxxer on our campus. Everyone I know of is simply against the mismanagement of exceptionally poor- quality COVID-19 vaccines. History tells us that instilling fear of a minority group never ends well. This scenario must be rectified immediately if our campus is ever to return to a safe and secure working and learning environment for all.

Committing to Abolishing the COVID-19 Vaccine Mandate
President Yates, the favour of a reply is requested. Not the kind that defers to public health officials, or a committee, or anyone else. Instead, a reply with the scientific rigour expected from a scholarly colleague rebutting each of my comments and addressing each question. Surely, you know the science underpinning COVID-19 vaccines inside and out by now. I strongly suspect that nobody would made a decision that disrupts an entire community and destroys the lives of some of its members without a fully developed rationale that can point to the weight of the peer-reviewed scientific literature to back it up. If it would be easier, I would be happy to have an open and respectful, but public and blunt moderated conversation about your vaccine mandate in front of our campus community; much like in the spirit of old-fashioned, healthy scientific debates. You can have your scientific and medical advisors attend and I will invite an equal number.
I am not saying this to be challenging. I honestly think it would be a great way to educate our campus community and expose them to the full spectrum of the science. And, if I am as wrong as my ‘fact checkers’ say, I would love for them to demonstrate this for my own sake as much as anyone else’s. So far, despite hundreds of invitations, not one person has done this in a scenario where I can respond in real-time. You need to understand; all I want is my life back and to be able to recognize my country again. I want to see the lives of the students, staff, and other faculty members that I have seen destroyed be restored again. I want to be able to return to my workplace and not be fearful of being hated or exposed to social, mental, and physical bullying. Instead, I want to be able to turn my talents and full attention back to being an academic public servant who can design better ways to treat diseases and help train Canada’s next generation of scientific and medical leaders. I simply cannot know all that I have shared in this letter and have suffered as much as I have and be silent about it.
My great uncles and family members before them served heroically in the World Wars to ensure Canada would remain a great and free democracy. I think they would be horrified by what they see in Canada today. Indeed, many of my friends who immigrated from Communist countries or countries run by dictatorships are sharing fears about the direction our country is heading; it is reminding them of what they fled from. Further, mandating COVID-19 sets a scary precedent.
Did you know that multiplex tests for both SARS-CoV-2 and influenza viruses are on the horizon, along with dual- purpose vaccines that will use the same mRNA-based technology to simultaneously target SARS-CoV-2 and influenza viruses (https://www.ctvnews.ca/health/coronavirus/moderna-developing-single-dose-covid-19-flu-combo- vaccine-1.5578445). Rhetorically, will the University of Guelph consider masking, distancing, and/or mandating vaccines for influenza in the future? Please rescind your COVID-19 vaccine mandate immediately. It is doing more harm than good. Unbelievably, among many other problems, it is even discriminating against those who can prove they are immune to SARS-CoV-2!
Mandating COVID-19 Vaccines Creates Absurd Situations
In closing, and to highlight the absurdity of mandating COVID-19 vaccines… President Yates, I have proven to you that I am immune to SARS-CoV-2, but you have banned me from the campus and ruined my life because I don’t have a piece of paper saying that someone saw two needles go into my shoulder. You have a piece of paper that says that someone saw two needles go into your shoulder, but you have not proven that you are immune to SARS-CoV-2. However, you are allowed on campus and your life can proceed uninterrupted. How is that fair?
Respectfully and in the mutual interest of the health and well-being of all members of our community,
Dr. Byram W. Bridle, PhD
Associate Professor of Viral Immunology
Department of Pathobiology
University of Guelph

Painting by Carmen Costello Calligraphy by Ari Honarvar
Rumi’s Desert

Out beyond ideas of wrongdoing and rightdoing,
there is a field. I’ll meet you there.
When the soul lies down in that grass, the world is too full to talk about.
Ideas, language, even the phrase “each other” doesn’t make any sense.
Translated by Coleman Barks
This is one of the most popular Rumi quotes in the west. This translation finds itself recited at wedding ceremonies, when intellectuals have a particularly contentious debate, and in therapists’ offices and meditation halls all over. When I speak of my love of Rumi, a common response is to inquire whether I know this poem.
And to be frank, until recently I hadn’t come across this poem in Farsi. I eventually did some research and found these verses:
از کفر و ز اسلام برون صحرائی است
ما را به میان آن فضا سودائی است
عارف چو بدان رسید سر را بنهد
نه کفر و نه اسلام و نه آنجا جائی است
When I translate these verses, I arrive at a very different place. Not the attractive field where we drop all of our ideas and disagreements into the grass in which we lay and become filled with oneness, but a stark desolate land of disillusionment:
Out beyond wrongdoing and right doing, there is a desert
The desert beckons us as if it were the oasis
We long to hold one another in its lush grass
and drink from the clear spring
The moon whispers in my ear:I have one foot in that desert
But don’t ask me to meet you there
For in that desert of disillusionment,
just as with right and wrong,
you and I and even oneness
cease to exist.
This poem has brilliantly tapped into both the dissatisfaction and the illusion-conjuring power of the mind. It is as if the poet has gone through different stages of seeking and has found each stage a mirage and unsatisfactory at its core. First, seeking the love of others, becoming dissatisfied, and turning to fame and wealth as salvation. And when that failed too, the seeker turns to spirituality, but that can become a mirage too. In the end, it is the great illusionist of the mind that takes on the challenging feat: To make an illusion of disillusionment.
The desert beckons us as if it were the oasis…
In this verse, Molana Rumi hints at the desperation and longing of a man who has gone through all the stages of seeking and has arrived at the final one. But before entering, non-duality is seen as a state in which one can comfortably take a neutral stance at every happening since, after all in this land, no wrongdoing or right doing exists. This illusion, like all illusions, is a deeply personal one in which we seek and ask God, the universe, and the saints to grant us the winning lottery ticket, making us the chosen one, so through our wealth, insight and in this case enlightenment, we can truly help others. In essence, this illusion is trickle-down economics at its finest, in its most grand and exulted conclusion. In this luxurious land, no hardship of life can touch us and this can only be good because others can only benefit from being in our presence.
The moon whispers in my ear…
Here, Molana Rumi talks of the realized one. In my translations, I use the metaphor of the moon as the witness, the realized one. She knows that in a non-dual state, there is only emptiness. There is no grass, no clear spring and no lovers to be united. It is the greatest disillusionment, naked, unadorned, and devoid of everything, including love.
So if we dare to venture into the barren land of Nothingness as Attar, Rumi’s teacher, wrote about it in the “Seven Valleys of Love”, yes, we must forego the ideas of wrongdoing and right doing. But unlike a personal illusion, this land is the embodiment of the impersonal. There is no family, no friends, no personal comfort, and no You or I. We must abandon everything and everyone we know and love. Still eager for your jaunt into that grassy field?
Here’s a recording of the poem in Farsi
Ari Honarvar
Speaker, performer, refugee advocate | @guardian @washingtonpost and more| The author of Rumi’s Gift and upcoming novel, A Girl Called Rumi rumiwithaview.com
A newly published medical study found that infection from COVID-19 confers considerably longer-lasting and stronger protection against the Delta variant of the virus than vaccines.
“The natural immune protection that develops after a SARS-CoV-2 infection offers considerably more of a shield against the Delta variant of the pandemic coronavirus than two doses of the Pfizer-BioNTech vaccine, according to a large Israeli study that some scientists wish came with a ‘Don’t try this at home’ label,” Science reported Thursday. “The newly released data show people who once had a SARS-CoV-2 infection were much less likely than vaccinated people to get Delta, develop symptoms from it, or become hospitalized with serious COVID-19.”
Put another way, vaccinated individuals were 27 times more likely to get a symptomatic COVID infection than those with natural immunity from COVID.
In Israel, vaccinated individuals had 27 times higher risk of symptomatic COVID infection compared to those with natural immunity from prior COVID disease [95%CI:13-57, adjusted for time of vaccine/disease]. No COVID deaths in either group.https://t.co/hopImCD1D0
— Martin Kulldorff (@MartinKulldorff) August 25, 2021
A Death Blow to Vaccine Passports?
The findings come as many governments around the world are demanding citizens acquire “vaccine passports” to travel. New York City, France, and the Canadian provinces of Quebec and British Columbia are among those who have recently embraced vaccine passports.
Meanwhile, Australia has floated the idea of making higher vaccination rates a condition of lifting its lockdown in jurisdictions, while President Joe Biden is considering making interstate travel unlawful for people who have not been vaccinated for COVID-19.
Vaccine passports are morally dubious for many reasons, not the least of which is that freedom of movement is a basic human right. However, vaccine passports become even more senseless in light of the new findings out of Israel and revelations from the CDC, some say.
Harvard Medical School professor Martin Kulldorff said research showing that natural immunity offers exponentially more protection than vaccines means vaccine passports are both unscientific and discriminatory, since they disproportionately affect working class individuals.
“Prior COVID disease (many working class) provides better immunity than vaccines (many professionals), so vaccine mandates are not only scientific nonsense, they are also discriminatory and unethical,” Kulldorff, a biostatistician and epidemiologist, observed on Twitter.
Prior COVID disease (many working class) provides better immunity than vaccines (many professionals), so vaccine mandates are not only scientific nonsense, they are also discriminatory and unethical. https://t.co/d14kTPnCWk
— Martin Kulldorff (@MartinKulldorff) August 27, 2021
Nor is the study out of Israel a one-off. Media reports show that no fewer than 15 academic studies have found that natural immunity offers immense protection from COVID-19.
“Among the most fraudulent messages of the CDC's campaign of deceit is to force the vaccine on those with prior infection, who have a greater degree of protection against all versions of the virus than those with any of the vaccines.”
15 studies show…https://t.co/oXaI3L0Y3S
— Thomas Massie (@RepThomasMassie) August 26, 2021
Moreover, CDC research shows that vaccinated individuals still get infected with COVID-19 and carry just as much of the virus in their throat and nasal passage as unvaccinated individuals
“High viral loads suggest an increased risk of transmission and raised concern that, unlike with other variants, vaccinated people infected with Delta can transmit the virus,” CDC Rochelle Director Walensky noted following a Cape Cod outbreak that included mostly vaccinated individuals.
These data suggest that vaccinated individuals are still spreading the virus much like unvaccinated individuals.
The Bottom Line
Vaccine passports would be immoral and a massive government overreach even in the absence of these findings. There is simply no historical parallel for governments attempting to restrict the movements of healthy people over a respiratory virus in this manner.
Yet the justification for vaccine passports becomes not just wrong but absurd in light of these new revelations.
People who have had COVID already have significantly more protection from the virus than people who’ve been vaccinated. Meanwhile, people who’ve not had COVID and choose to not get vaccinated may or may not be making an unwise decision. But if they are, they are principally putting only themselves at risk.


The hands of an elderly member of the Japanese mafia (the "Yakuza"). In addition to the tattoos, note the amputation of the little finger. It is one of the many forms of ritual mutilation practiced in human society. The idea is that the suffering involved proves the will of the sufferer to belong to a specific group.
Translated from Italian and slightly modified from "Effetto Seneca"
Until recently, there existed a criminal organization in Japan whose members went by the name of Yakuza. It was similar to the Italian mafia, so much that it is often called the "Japanese mafia." The Yakuza practiced various forms of ritual mutilation, one was the amputation of the last phalanx of the little finger. Fosco Maraini describes it in his "Meeting with Japan" (1958), telling us that he himself cut his little finger as a protest against the Japanese government during WW2.
Cutting off a phalanx of the little finger is a good example of a ritual mutilation. As an impairment, it is minor, but it is visible, painful, and a test of courage for those who do it. Thus, it is a testimony of belonging to a certain group - in this case the Yakuza. Today, they have almost disappeared in Japan and with them the hands with the amputated little finger. But ritual mutilation in other forms is common in other regions of the world.
In the western part of Eurasia, there are two types of widespread ritual mutilations: male circumcision and infibulation in its various forms of female genital mutilation. For both, there is talk of possible health benefits, but there is no definite evidence for that. They are, rather, evidence of belonging to a social or religious group. As we know, circumcision is mandatory for Jews, it is common, but not mandatory, among Muslims although, it is less common but not rare among Christians. In Europe, about 20% of the males are circumcised, a percentage that rises to about 80% in the United States.
All in all, circumcision does not have great effects on the body of the circumcised, but as far as infibulation is concerned, we are talking about a real mutilation that heavily affects the sexuality of the woman who undergoes the practice. It is condemned by the Christian religion, it is not part of the Jewish tradition, and has been the subject of Islamic Fatwas that prohibit it. In many states, it is explicitly prohibited by law.
Yet, infibulation in its various forms tenaciously resists in certain areas of the world where it is an ancient tradition, especially in Africa. It is difficult for us Westerners to realize why women in these regions do not see it as an imposition, but as a source of pride, a proof of maturity, and of belonging to the society in which they live. In these societies, the non-infibulated woman is considered an outcast, an enemy to be isolated and demonized. It is a perverse mechanism that persists despite many attempts to eradicate the practice.
There are, and were in the past, many other ritual mutilation practices that affect both men and women. It is said that in ancient times the Amazons amputated one of their breasts to shoot better with the bow. It is almost certainly a legend. Even if it were true, it's unlikely it would have improved their ability to skewer enemies with arrows. If the Amazons (assuming they ever existed) did that, it was for the same reason that led the Yakuza to sever a phalanx of their little finger: publicly showing that they belonged to the group.
In China, the binding of girls' feet was practiced until recently. It was a form of mutilation: a real daily torture with consequences that lasted for a lifetime. As adults, these women were unable to walk alone. Fortunately, today it is no longer practiced, but some elderly Chinese women who underwent this practice in their youth are still alive.
In the West, the prevalence of the Christian vision starting from Paul of Tarsus tended to reject any irreversible intervention on the human body. Nonetheless, minor forms of mutilation remained common, such as piercing the earlobes for earrings.
More often than not, in recent times, mutilations were performed with the support of "Science." One example was the removal of children's tonsils, as it was fashionable to do in the 1970s. An operation that probably did not cause much harm, but whose usefulness is at least questionable. It is still performed nowadays.
Much worse is the case of radical mastectomy for the treatment of breast cancer. As Siddhartha Mukherjee describes in his book. "The Emperor of All Maladies" (2010), it was an invasive therapy that in some cases involved "the complete excision of all breast tissue, axillary contents, removal of the latissimus dorsi, major pectoral muscles and minor and internal mammary lymph node dissection". And all this without a real medical reason to justify it. The result was a radical and irreversible mutilation that turned the woman into an invalid for the rest of her life.
In our society, theoretically rational, we might think that we have freed ourselves from these customs that we consider superstitions or at least errors of evaluation of a still imperfect science. But the "suffering-based proof of belonging" mechanism is deeply ingrained in our thinking and tends to pop up in one way or another, with or without medical justifications.
Let's just think about the use of tattoos, considered primitive and barbaric in the West until a few decades ago, today widespread among young people. Getting a tattoo is painful and therefore a test of courage for those who do it. It is also irreversible so that it is proof of definitive belonging to a certain social group. So it is not surprising that it has spread so quickly in a society that gives to the young little or nothing, apart from beatings, real or virtual.
It is impossible to deny that, under a smattering of rationality, our mentality is still that of much older times. And when we are under social stress, obsessive and punitive tendencies come out easily and are impossible to stop. Thankfully, women today don't have to cut their breasts for better accuracy with the bow (for now), and men don't have to slice off their little fingers to show their courage (for now).
But society changes in unpredictable ways and today it would be possible to use new ways to prove that someone willingly underwent some kind of painful ritual in order to belong to a certain group. No need to show actual scars, a digital certificate will be enough. Whether this will actually take place is left to the reader to ponder.
Introduction
This article aims at giving an overview of the ivermectin controversy, including current practices of research, publishing and governmental policy formation, by presenting a timeline of relevant events, compiled from peer-reviewed academic journals indexed in PubMed, preprint servers such as medRxiv, chemRxiv, SSRN, Research Square and ResearchGate, international clinical trials registers, international newspapers and medical news service providers as well as websites. As there have been a lot of sparsely documented events internationally, the search has not been systematic, the timeline is unavoidably incomplete, and there may naturally be some personal bias with regard to what has been selected. Also, the main focus of the article is on the last quarter of the 2020s and the first quarter of 2021. Despite these limitations the timeline may serve as a template for more detailed inquiries.
Due to the large number of studies and limited space, each study is mentioned only briefly, without a possibility to analyze methodologies or results in depth. Statistically significant endpoints are reported, with nonsignificant endpoints mostly left out. For consistency, results are in most cases formatted as they appear in a meta-analysis by the Covid Analysis research group, possibly reformulated in comparison to the original sources (e.g. odds ratios converted to relative risk or methodological errors corrected) [1];[2];[3].
Ivermectin was invented in Japan in 1975 by Kitasato University professor emeritus Satoshi ¯ Omura, for which he won the 2015 Nobel Prize in physiology or medicine [4]. The drug has proven effective in eradicating parasitic infections and it is therefore best known as an antiparasitic agent, with several billion doses having been administered since 1981. The patent for the product was owned by Merck & Co/MSD. In most countries the patent expired in 1996. Currently, ivermectin preparations are available internationally from many sources, with the production cost of a single dose estimated to be less than 0.1 US dollars [5].
For prophylaxis of onchocerciasis (river blindness) and strongyloidiasis ivermectin is administered as a single oral yearly dose of 0.15-0.20 mg/kg [6];[7]. For lymphatic filariasis, a once-yearly dose of 0.3-0.4 mg/kg or bi-yearly dose of 0.15–0.2 mg/kg is administered [6]. For classic scabies, two doses of 0.2 mg/kg approximately one week apart are recommended, and for crusted scabies three to seven doses of 0.2 mg/kg depending on the infection severity [8];[9]. With regard to malaria, repurposing ivermectin as a complement to current malaria vector control tools is currently being investigated, with a proposed dosing regime of 0.4 mg/kg repeated three times during the malaria season, and another proposed dosing regime of 0.3 mg/kg on three consecutive days in combination with two other pharmaceuticals also repeated three times during the season [10].
With regard to its in vitro antiviral action, ivermectin has shown robust antiviral action towards a range of RNA and DNA viruses, including HIV-1, dengue, Zika and West Nile Virus, Venezuelan equine encephalitis virus, Chikungunya, pseudorabies virus, adenovirus, and SARS-CoV-2 (COVID-19) [11]. For dengue virus, a combined phase II/III patient randomized controlled trial (RCT) has been completed[12].
Another recent line of research has been an investigation into ivermectin’s efficacy in cancer. A study found out that ivermectin at a very low dose drastically reversed the resistance of the tumor cells to the chemotherapeutic drugs both in vitro and in vivo [13]. Ivermectin could thus be used in combination with chemotherapeutic agents to treat drug-resistant cancers.
With regard to the mechanism of action of ivermectin as an antiparasitic medication, Chung et al. describe that ivermectin interacts with vertebrate and invertebrate γ-aminobutyric acid (GABA) receptor and invertebrate glutamate-gated chloride channels, increasing chloride ion influx with subsequent paralysis and death in the target organism [14]. Ivermectin is effective in killing nematodes and arthropods with a single dose of 0.1-0.3 mg/kg but has has a very wide margin of safety in mammals because in mammals GABA-mediated nerves occur only in the central nervous system and ivermectin does not readily cross the blood-brain barrier [14].
With regard to safety of overdosing, in chickens and most dogs subcutaneous doses of approximately 5 mg/kg have been shown to cause mild symptoms and doses of approximately 15 mg/kg severe symptoms up to coma and death. In two described cases on humans, a 16-month-old child ingesting 6.7 to 8.72 mg/kg ivermectin resulted in frequent vomiting, somnolence, mild tachycardia, and hypotension, and a 61-year old woman became comatose three hours after ingesting 15.4 mg/kg agricultural ivermectin, requiring supportive intensive care but was discharged uneventfully on day 9 [14].
A double-blind, placebo-controlled dose escalation study with 68 healthy volunteers found no indication of central nervous system or general toxicity, or a difference in adverse effects between ivermectin and placebo groups for doses up to 2 mg/kg (ten times the highest FDA-approved dose of 0.2 mg/kg), in either single doses of 90 mg (1.0-1.5 mg/kg) or 120 mg (1.4-2.0 mg/kg), or in a repeated dosing regime with 30 mg (0.35-0.54 mg/kg) or 60 mg (0.71-1.1 mg/kg) on days 1, 4 and 7 (a total of three doses) [15]. Mean plasma concentrations were 2.6 times higher when administered with food.
The FDA-approved dosing for treatment of parasitic diseases is 0.2 mg/kg. The doses used in COVID-19 related clinical trials described in this article varied between 0.2-0.6 mg/kg. With regard to safety of ivermectin in general, a current World Health Organization (WHO) document on the treatment of onchocerciasis states that “ivermectin is safe and can be used on a wide scale” [16]. With regard to safety for children, a recent systematic review and and an individual patient data meta-analysis of ivermectin use in children weighing less than 15 kg concluded that existing limited data between January 1980 and October 2019 suggest that oral ivermectin in children weighing less than 15 kilograms is safe [17]. Overall a total of 1.4% (15/1,088) of children experienced 18 adverse events all of which were mild and self-limiting. No serious adverse events were reported.
With regard to safety of ivermectin during pregnancy, a document from 2004 published by the WHO titled “Mass treatment with ivermectin: an underutilized public health strategy” describes safety during pregnancy, noting that “a number of follow-up studies have found that inadvertent filariasis mass campaign use of ivermectin during pregnancy has not been associated with adverse pregnancy outcomes or negative effects on pregnant women or their offspring”, referring to a study by Gyapong et al. who concluded “there is no evidence of a higher risk of congenital malformation or abortions in those who are inadvertently exposed” [18];[19].
April 2020
On April 3, a Monash University of Australia in vitro ivermectin study by Caly et al. reported that ivermectin is an inhibitor of SARS-CoV-2 virus in vitro, that a single treatment effected approximately 5000-fold reduction in virus at 48 h in cell culture, and that ivermectin is FDA-approved for parasitic infections and included on the WHO model list of essential medicines, thus being widely available [20];[21];[22];[23].
On April 6, a French biotechnology company MedinCell which had been studying ivermectin for malaria announced an initiative to develop an injectable form of ivermectin for prophylaxis of COVID-19 [24];[25];[26].
On April 10, mentioning increased interest in ivermectin after the Australian in vitro study, US FDA issued a warning against using veterinary ivermectin as treatment for COVID-19 in humans, citing safety concerns [27]. It noted additional testing is needed to determine whether ivermectin might be safe or effective in COVID-19 in humans.
On April 13, two Florida, US pulmonologists Rajter and Cepelowicz-Rajter were said to be pioneering early treatments with ivermectin, reporting a nearly 100% response rate with early administration, adding that they were initiating clinical studies [28].
On April 13, a preprint by Patel et al. described an observational registry-based study from 169 hospitals claiming that a single dose of 0.15 mg/kg of ivermectin produced a significant mortality reduction (7.7% vs. 18.6%) in 1,970 patients requiring mechanical ventilation [29];[30].
On April 14, two medical doctors, Gustavo Elera Arévalo and Fernando Polanco Hinostroza in La Merced (Chanchamayo) in Peru, begun treating a COVID-19 outbreak in a prison with ivermectin, later also treating the local police [31].
... and hundreds more events to April 3 2021. Go to the source to read the full chronology.
Discussion
A central question in the communications was whether more studies were needed. In October 2020, when the FLCCC Alliance recommendation on ivermectin was published, the decision to recommend it was assumedly largely based on the perceived consistent positivity of the effects: “seeing a ‘signal’ in the data”. This method could also be called reliance on “clinical experience” or even “intuition”. Comparing five Covid Analysis group’s meta-analyses from November 26 (n=21), December 29 (n=28),January 26 (n=35), February 27 (n=42), and March 31 (n=49) [438], calculated improvements in clinical indicators, with probabilities of an equal or greater percentage of positive results from an ineffective treatment, were as follows: improvements in prophylaxis (pre-exposure/post-exposure or total) we-re 98%/87% (p=0.063/0.25), 91%/90% (p=0.0078/0.25), 90% (p=0.00098), 89% (p=0.00049), and 89%(p=0.00024), respectively. In early treatment, the improvements were 91% (p=0.13), 87% (p=0.016), 84%(p=0.00098), 83% (p=0.00012), and 80% (p=0.0000076). In late treatment, the improvements were 60%(p=0.00024), 48% (p=0.00012), 39% (p=0.000031), 51% (p=0.0000038), and 50% (p=0.00000095). All together, the improvements were 75% (p=0.00000048), 78% (p=0.0000000037), 74% (p=0.000000000029),75% (p=0.00000000000023), and 72% (p=0.000000000000002). It appears that in 2021 the variation in estimated efficacy due to addition of more studies to the meta-analysis was too small to be clinically meaningful. Therefore, more studies provided little additional clinically relevant information, and the argument against the treatment was solely based on the assumed unreliability of all the existing data.The panel which prepared the WHO guideline of March 30, 2021 included in its meta-analysis only five studies that directly compared ivermectin with standard of care and reported mortality [428]. The result indicated 64% reduction in mortality (RR 0.36, 95% CI 0.17-0.75, no p value given, n=915,very low certainty evidence). The meta-analysis of six studies by Hill et al. indicated 75% reduction in mortality (RR 0.25, CI 0.12-0.52, p=0.0002, n=1,255) [275]. The March 31, 2021 meta-analysis of eight randomized controlled trials by the Covid Analysis group indicated 70% reduction in mortality (RR 0.31,95% CI 0.16-0.61, n=1,729, p<0.00032) [437]. The meta-analysis of thirteen trials by Bryant et al. devised using Cochrane standards indicated 68% reduction in mortality (RR 0.32, 95% CI 0.14-0.72, n=1,892,low to moderate-certainty evidence) [387]. The FLCCC group’s meta-analysis of four observational and six randomized controlled trials indicated an overall 69% reduction in mortality (RR 0.31, n=3,508,p<0.0001) [168];[214].
In addition to presenting the new meta-analysis, the guideline presented data from the WHO living guideline [439]. The living guideline analysis indicated 70 deaths per 1,000 patients (7%) for standard of care, and 14 (1.4%) for ivermectin, respectively, i.e. an absolute difference of 56 patients (5.6%) with a 95% confidence interval of 64 to 44 fewer deaths, and a relative mortality reduction of 80%. The odds ratio for mortality was 0.19 (OR 0.19, 95% CI 0.09-0.36) based on 1,419 patients in seven studies. The certainty of evidence was estimated to be very low due to serious risk of bias and very serious imprecision.
This imprecision was explained as follows: “for mortality there were only 31 deaths across all 915 patients randomised - an extremely small number of events on which to base conclusions” (referring to five studies instead of seven), suggesting unsuitability of the chosen methodology for evaluation of medicines that might significantly reduce mortality, as conclusions could then not be made.
As a reference for the above data the guideline cited Siemieniuk et al. [440] which did not contain theabove results but instead presented a third set of mortality results, indicating a mortality of 130 per1000 patients (13%) for stardard of care. For a combination of doxycycline and ivermectin, the estimated reduction in deaths was 130 (95% CI 130-123). For ivermectin alone, the reduction was 103 (95% CI117-78). For proxalutamide, the values were 130 (95% CI 130-118), for colchicine 78 (95% CI 110-9), and significantly less for other included options.
These two additional sets of results indicated larger reductions in mortality (approximately 80%) than the meta-analysis. With regard to the earlier meta-analysis by Hill et al. [275], Siemieniuk et al. stated that “several of these trials could not be included in the analysis . . . ten trials that reported no outcomesof interest”, citing the Hill et al. meta-analysis among the trials reporting no outcomes of interest. Thenew meta-analysis was presented in Rochwerg et al. [441]. This article mentioned neither the meta-analysis by Hill et al. nor the mortality results of Siemieniuk et al. Rochwerg et al. also noted that “we currently lack persuasive evidence of a mechanism of action for ivermectin in covid-19; any observed clinical benefit would be unexplained”, possibly suggesting that not even an effective intervention could be utilized unless the mechanism of action was “explainable”.
Based on their meta-analyses the other groups (FLCCC, CovidAnalysis, BIRD) recommended treatment, the WHO panel did not, referring to “the strong likelihood that chance may be playing a role in the observed findings” [441]. None of the authors of the WHO-funded meta-analysis by Hill et al. were included in the panel. The low cost and wide availability of ivermectin did not, in the panel’s view, mandate the use of a drug with uncertain benefits and possible harms. Resource considerations, accessibility,feasibility and impact on health equity “did not alter the recommendation”. The panel worried about drug shortages in helminth control and elimination programmes [441];[428]. The panel listed the risk of severe adverse events leading to drug discontinuation as a reason for non-adoption, apparently suggesting that a pharmaceutical should not be adopted at all if a small subset of patients might stop using it. For some reason the panel “inferred that almost all well-informed patients would want to receive ivermectin only in the context of a randomized trial, given that the evidence left a very high degree of uncertainty . . . the panel anticipated little variation in values and preferences between patients when it came to this intervention”, giving an impression of dictating patients’ preferences without asking them or giving them a choice.
The panel “raised concerns about diverting attention and resources away from care likely to provide a benefit such as corticosteroids in patients with severe COVID-19 and other supportive care interventions”. Considering that in the majority of countries, no prophylaxis or early treatment method was officiallyavailable, that corticosteroids were to be avoided in prophylaxis and early treatment, and that the useof corticosteroids in late treatment practically necessitated use of ivermectin to prevent strongyloidiasis-related hyperinflammation, this rationale appeared particularly illogical. The panel did note, however,that “ivermectin may still be considered in strongyloidiasis endemic areas, at the discretion of clinicians overseeing treatment, albeit not for treatment of COVID-19 itself”.
Considering the attitudes towards ivermectin in the industrialized countries in general, one of the main obstacles for reception of the idea of repurposed medicines may have been the Surgisphere scandal and the widespread controversy regarding hydroxychloroquine in early 2020, leading to a generalized distrust of research among the politicians, governmental administrative personnel and the public, especially in the more developed countries which appeared to put more importance on the research. This distrust, in turn, possibly opened new avenues for various kinds of societal manipulation.
The distrust appeared to have also lead to, for example, social media and video streaming platforms actively but inconsistently and indiscriminately censoring many subjects and groups, including ivermectin research groups and their results, regardless of their level of academic merit. These practices often appeared similar to censorship practices in authoritarian countries. Mainstream media appeared to maintain an inverted understanding on the process of science in which scientific knowledge was apparently assumed to flow down from the NIH and WHO to the researchers, not the other way around. Financial newspapers (Wall Street Journal, Financial Times) may have possessed a more realistic view on medical research and ivermectin than generalist press conventionally considered high quality (e.g. The New York Times, Associated Press, The Guardian), with some practically accusing researchers of not adhering to the guidelines given by the NIH, for example. The open encyclopedia Wikipedia took pains to only mention negative studies about ivermectin, listing it among the COVID-19 misinformation, even citing a commentator saying that “the narrative of ivermectin as a ‘miracle cure’ for COVID-19 is a ‘metastasized’ version of a similar conspiracy theory around the drug hydroxychloroquine, in which unspecified powers are thought to be suppressing news of the drug’s effectiveness for their own malign purposes” [442];[443];[444].
As noted by Wall Street Journal quite early on in the ivermectin saga, the majority of the medical establishment appeared to require almost absolute certainty, resulting in “too much caution killing patients”, both health-wise and financially [183]. This approach seemed to only take into account quite theoretical health risks, disregarding not only the very probable societal harms of not taking any action but also the possible health benefits of taking an action under uncertainty. Thus, the process appeared largely a failure of a relatively simple risk-benefit analysis.
The more medically oriented arguments against the adoption of ivermectin were usually based on the hypothesis that the required (as indicated by the Caly et al. in vitro study [22]) plasma and lung tissue concentrations for an antiviral effect would likely not be achievable. Another argument was based on the host-directedness and the assumed toxicity of larger doses.
An additional disagreement concerned the use of placebo in clinical trials. This disagreement may havebeen at least partly related to a long-standing divide of the research community into active-control and placebo orthodox proponents [445]. Vagueness of the Helsinki Declaration of 2013 may easily lead into opposite interpretations of what should be done [446]. For example, the sentence to allow the use of placebo “where no proven intervention exists” left open who should decide what is a “proven intervention”, easily leading to a circular reasoning according to which a proven intervention cannot exist without a placebo-controlled randomized trial, thus the use of placebo must be allowed to prove the efficacy of the intervention. Similar vagueness plagues the whole section about placebo controls. The parties involved in the ivermectin trial controversies appeared unable to find any common ground with regard to this issue.During the period there appeared to be somewhat scarce interest in treatments research, with the wealthy societies’ focus on vaccinations and lockdowns, despite vaccinations being largely unavailable and lockdowns harmful for the economy. These countries appeared to pursue expensive, narrow-spectrum vaccination and new pharmaceuticals based strategies, ignoring cheaper options, whereas developing countries put more emphasis on affordable, broad-spectrum antivirals. One factor may have been the developing nations’ clinicians’ familiarity with ivermectin and its easy availability, whereas it has been a rarely prescribed medicine in most industrialized countries. In addition, prejudices and a bias against ideas originating outside of familiar organizations or one’s own country may have played a part in the industrialized countries ignoring ivermectin research carried out in the developing countries [447]. Cost-effectiveness of government funding for development of new medications and vaccines is an important issue. The US government invested USD 356 million in 60,000-100,000 doses of MK-7110, indicating aunit price between USD 5,933.00 and USD 3,560.00, with the initial results of efficacy indicating the same or slightly smaller efficacy as that of ivermectin. A 2015 article about mass treatment of onchocerciasisin Africa stated that Merck & Co/MSD had offered ivermectin at USD 1.51 per treatment, indicating a2300 to 3900-fold difference between the prices of ivermectin and MK-7110 [448];[222]. In this example,allocation of US government funding appeared inefficient with respect to investment in an experimental product with the unit costs in thousands of dollars, versus the option to use an existing medication with similar efficacy proven at least on a similar level of evidence and the unit costs in single digits.
There was a widespread disagreement on the fundamentals: which methods were appropriate as a basis for decision making, what counted as evidence, and what was ethical. In a broader view, the appropriateness and usefulness of the evidence based medicine paradigm as it was understood and applied during the period appeared questionable. US and European governmental bodies appeared to reject or ignore most of the ivermectin-related data, referring to insufficient evidence. In the US, the paradigm appeared inconsistently applied; more specifically, not applied to US Food and Drug Administration Emergency Use Authorization of remdesivir, whereas strictly applied to other medications including ivermectin. In addition, a strict requirement to compare a significantly more effective treatment to placebo may be considered unethical with regard to high mortality of patients in control groups. These indicate a clear need for a new methodology better than the current understanding and application of evidence-based medicine.
With regard to conflicts of interest, the US Food and Drug Administration (FDA) issued an EmergencyUse Authorization (EUA) for the use of remdesivir in patients with severe disease on May 1, even before the initial results of an ongoing trial were published and despite remdesivir being an investigational drug not approved for any indication. The 1,063-patient randomized controlled trial of remdesivir publishedon May 22 only indicated that remdesivir shortened the time to recovery (11 days vs 15 days, p<0.001)[449]. There wasn’t an obvious difference in mortality rates (8% vs. 11.6%, p=0.059) and the endpoints were changed mid-study which was deemed a questionable practice [450]. The final results were published on October 8. On August 28 the EUA was extended to “no longer require a severe disease”.
The adoption of corticosteroids as a consequence of the WHO-initiated 2,000-patient RECOVERY trial results was relatively swift. Also the emergency use authorization of remdesivir in the US was swift,based on initial and conflicting evidence. Twenty randomized clinical trial results on ivermectin’s efficacy for COVID-19 were available in February 2021. These trials were predominantly carried out outside the US and the EU, and did not lead to emergency use authorizations in the US or the EU. US FDA document “Emergency Use Authorization of Medical Products and Related Authorities – Gui-dance for Industry and Other Stakeholders” section “1. Criteria for Issuance” subsection “d. No Alternatives” states that “For FDA to issue an EUA, there must be no adequate, approved, and available alternative to the candidate product for diagnosing, preventing, or treating the disease or condition. A potential alternative product may be considered ‘unavailable’ if there are insufficient supplies of the approved alternative to fully meet the emergency need. A potential alternative product may be considered ‘inadequate’ if, for example, there are contraindicating data for special circumstances or populations (e.g., children, immunocompromised individuals, or individuals with a drug allergy), if a dosage form of an approved product is inappropriate for use in a special population (e.g., a tablet for individuals who cannot swallow pills), or if the agent is or may be resistant to approved and available alternative products” [451].
It may thus be derived that licensing of repurposed medicines such as ivermectin for outpatient treatment and prophylaxis of COVID-19 would have prevented emergency use authorizations of new pharmaceuticals in development. In the case of prophylaxis, such licensing might even have affected vaccines. Thus,there appeared to exist substantial financial conflicts of interest against licensing of repurposed medicines.
Considering the total net utility of a society it is unlikely that unilateral support to only the investments of the pharmaceutical industry could ever offset the harms to other industries and the population. The society thus has a strong incentive to abolish the financial incentive structures of the pharmaceutical industry and the government that led to the current situation, in order to prevent a similar outcome in the future.
Considering the estimated efficacy of ivermectin around 90% in prophylaxis and the option of an early outpatient treatment with an estimated efficacy around 75%, an early introduction of ivermectin might have prevented a large part of COVID-19 infections post first wave in many European Union countries and in the United States.
Administrative issues, inconsistent requirements of evidence related to the evidence-based medicine paradigm, and possibly conflicts of interest with patentable, commercial products in development prevented introduction of early outpatient ivermectin treatments in the last quarter of 2020 and the first quarter of 2021. This lack of response is likely to have caused unnecessary deaths and difficult-to-repair financial and health consequences in the affected societies.
The culture of medical litigation prevalent in the United States may have created patterns of behavior that have also spread to countries with less actual litigation, yet leading to mental paradigms favoring extreme caution and non-action, in turn leading to stagnation. One of the features of a paradigm is an inability of the involved people to transcend it or even see that it is just one possible paradigm out of many options, some of which may be more optimal in a given situation.
Conclusion
The period appeared conflicted, with researchers, clinicians, governmental agencies and commercial entities holding deeply conflicting views on fundamental issues, including which methods were considered appropriate as a basis for decision making, what could be considered as sufficient evidence, and what was ethical. In a broader historical perspective, the timeline of events depicts rather dysfunctional societies unable to properly communicate and organize themselves, leading to misallocation of resources and decisions that may have conflicted with elementary ethical considerations, with this behavior rationalized by claiming adherence to mental paradigms that may have poorly matched the situation. In summary, the pandemic response especially in the United States and the European union appeared severely lacking.Further research on the details of these processes is warranted.

• Pfizer-BioNTech Vaccine Becomes First To Win FDA’s Full Approval (USAT)
• Does The FDA Think These Data Justify Approval Of A Covid-19 Vaccine? (BMJ)
• Fully Vaccinated Healthcare Workers Carry 251 Times Viral Load (McCullough)
• FDA Ignores Both Science and Law (Denninger)
• Pfizer and Moderna Lost The Clinical Trial Control Group (CTH)
• Everything You Need to Know About Informed Consent (21CW)
• Statistical Fraud in the FDA Vaccine Approval Process (JoshM)
• The More Masks Fail, The More We Need Them (Ian)
• Pentagon To Mandate Covid-19 Vaccinations For All Military Personnel (RT)
• NYC Orders 150,000 Teachers & School Staff To Get Vaccinated (ZH)
• Truckers Threaten To Shut Down Australia Due to Covid Insanity (OI)
• Keeping Fear Alive (Tierney)

It’s been an insane 24 hours. You’d think a full approval of a vaccine would be a straightforward event, but the FDA just made things more, and extremely, complicated. First, a few bits and pieces from what they issued:
“COMIRNATY is the first COVID-19 vaccine to be granted FDA approval ”
also:
“These may not be all the possible side effects of the vaccine. Serious and unexpected side effects may occur. THE VACCINE IS STILL BEING STUDIED IN CLINICAL TRIALS.”
On August 23, 2021, FDA approved the biologics license application (BLA) submitted by BioNTech Manufacturing GmbH for COMIRNATY (COVID-19 Vaccine, mRNA) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older…
…the EUA will remain in place for the Pfizer-BioNTech COVID-19 vaccine for the previously-authorized indication and uses, and to authorize use of COMIRNATY (COVID-19 Vaccine, mRNA) under this EUA for certain uses that are not included in the approved BLA…
COMIRNATY (COVID-19 Vaccine, mRNA) is the same formulation as the PfizerBioNTech COVID-19 Vaccine and can be used interchangeably with the Pfizer-BioNTech COVID-19 Vaccine to provide the COVID-19 vaccination series…
C. There is no adequate, approved, and available [see Note 9] alternative to the emergency use of Pfizer-BioNTech COVID 19 Vaccine to prevent COVID-19.
[Note 9:] Although COMIRNATY (COVID-19 Vaccine, mRNA) is approved to prevent COVID-19 in individuals 16 years of age and older, there is not sufficient approved vaccine available for distribution to this population in its entirety at the time of reissuance of this EUA. Additionally, there are no products that are approved to prevent COVID-19 in individuals age 12 through 15, or that are approved to provide an additional dose to the immunocompromised population described in this EUA.
Conditions Related to Printed Matter, Advertising, and Promotion
X. All descriptive printed matter, advertising, and promotional material, relating to the use of the Pfizer-BioNTech COVID 19 Vaccine shall be consistent with the authorized labeling, as well as the terms set forth in this EUA, and meet the requirements set forth in section 502(a) and (n) of the FD&C Act and FDA implementing regulations.
Y. All descriptive printed matter, advertising, and promotional material relating to the use of the Pfizer-BioNTech COVID 19 Vaccine clearly and conspicuously shall state that:
” This product has not been approved or licensed by FDA, but has been authorized for emergency use by FDA, under an EUA to prevent Coronavirus Disease 2019 (COVID-19) for use in individuals 12 years of age and older; and
” The emergency use of this product is only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of the medical product under Section 564(b)(1) of the FD&C Act unless the declaration is terminated or authorization revoked sooner.
The original documents. Just check the dates. What happened to those?
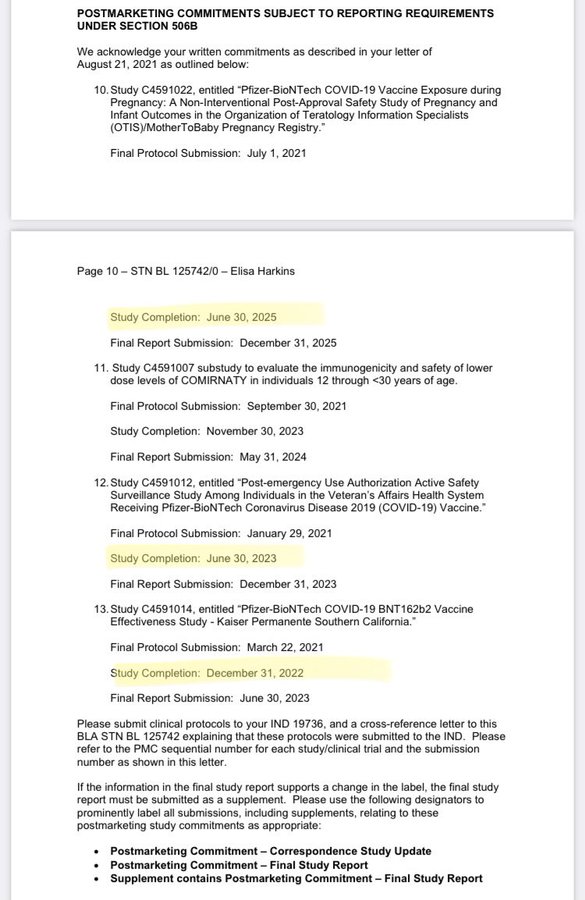
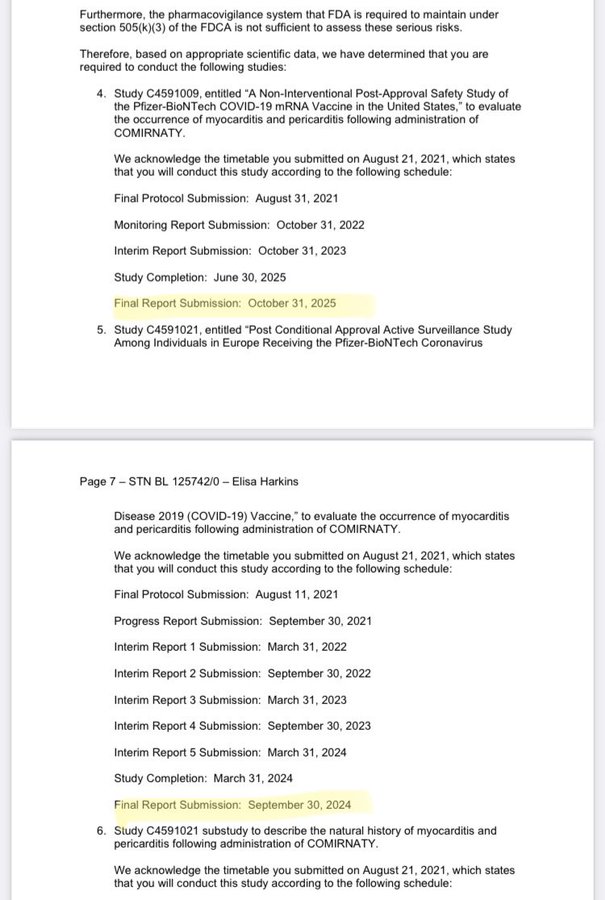
Two high vaccination rates: Iceland Full Vaxxed 74%, Israel 62%
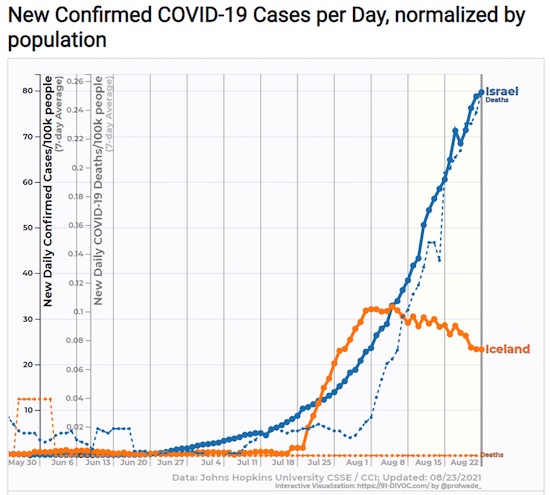
“The Pfizer-BioNTech emergency use authorization was based on clinical trials involving about 37,000 people.”
Well, not really, because they stopped those trials.
• Pfizer-BioNTech Vaccine Becomes First To Win FDA’s Full Approval (USAT)
Eight months after authorizing the Pfizer-BioNTech COVID-19 vaccine for emergency use in the USA, the Food and Drug Administration issued its full stamp of approval. Now that the companies’ detailed, so-called biologics license application has been granted, it’s likely that vaccination will be required by many companies, schools and other entities. The FDA decision clears the way for the companies to market their vaccine, which is not permitted without full licensure. And it may launch a race for booster shots, allowing doctors to prescribe extra Pfizer-BioNTech shots “off label” to anyone they think should get one. The FDA confirmed late last year through a more streamlined evaluation process that the vaccine, from pharmaceutical giant Pfizer and its partner, German startup BioNTech, was safe, effective and could be reliably produced.
The review of the 340,000-page license application was completed in just 97 days by FDA staff working “night and day,” said Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, which approves vaccines “We completed this in about 40% of the normal clock time for a submission of this magnitude,” he said. The license application was three times the size of the emergency use authorization submission, which weighed in at 110,000 pages. The companies have manufactured more than 2 billion doses, more than 200 million of which were administered in the USA, the most of any of the three vaccines allowed for use in the country. The full license includes four more months of efficacy and safety data, confirming trial results and detailing manufacturing processes.
The Pfizer-BioNTech emergency use authorization was based on clinical trials involving about 37,000 people. The full approval was based on study results involving more than 44,000 people followed for six months. The license applies only to those 16 and over, but the vaccine is allowed for those 12 to 15 under the previous authorization. “Based on the longer-term follow-up data that we submitted, today’s approval for those aged 16 and over affirms the efficacy and safety profile of our vaccine at a time when it is urgently needed,” Pfizer chairman and CEO Albert Bourla said in a statement. “I am hopeful this approval will help increase confidence in our vaccine, as vaccination remains the best tool we have to help protect lives and achieve herd immunity.”
Not sure it’s a great idea for the FDA to have pissed off Peter Doshi, senior editor at The BMJ, one of the most reputable magazines around. Much more at the original (link).
• Does The FDA Think These Data Justify Approval Of A Covid-19 Vaccine? (BMJ)
On 28 July 2021, Pfizer and BioNTech posted updated results for their ongoing phase 3 covid-19 vaccine trial. The preprint came almost a year to the day after the historical trial commenced, and nearly four months since the companies announced vaccine efficacy estimates “up to six months.” But you won’t find 10 month follow-up data here. While the preprint is new, the results it contains aren’t particularly up to date. In fact, the paper is based on the same data cut-off date (13 March 2021) as the 1 April press release, and its topline efficacy result is identical: 91.3% (95% CI 89.0 to 93.2) vaccine efficacy against symptomatic covid-19 through “up to six months of follow-up.” The 20 page preprint matters because it represents the most detailed public account of the pivotal trial data Pfizer submitted in pursuit of the world’s first “full approval” of a coronavirus vaccine from the Food and Drug Administration. It deserves careful scrutiny.
[..] The elephant named “waning immunity”…“Waning immunity” is a known problem for influenza vaccines, with some studies showing near zero effectiveness after just three months, meaning a vaccine taken early may ultimately provide no protection by the time “flu season” arrives some months later. If vaccine efficacy wanes over time, the crucial question becomes what level of effectiveness will the vaccine provide when a person is actually exposed to the virus? Unlike covid vaccines, influenza vaccine performance has always been judged over a full season, not a couple months. And so the recent reports from Israel’s Ministry of Health caught my eye. In early July, they reported that efficacy against infection and symptomatic disease “fell to 64%.” By late July it had fallen to 39% where Delta is the dominant strain. This is very low. For context, the FDA’s expectation is of “at least 50%” efficacy for any approvable vaccine.
_
Delta may not be responsible Enter Pfizer’s preprint. As an RCT reporting “up to six months of follow-up,” it is notable that evidence of waning immunity was already visible in the data by the 13 March 2021 data cut-off… And it’s hard to imagine how the Delta variant could play a real role here, for 77% of trial participants were from the United States, where Delta was not established until months after data cut-off. Waning efficacy has the potential to be far more than a minor inconvenience; it can dramatically change the risk-benefit calculus.
The “six month” preprint based on the 7% of trial participants who remained blinded at six months Despite the reference to “six month safety and efficacy” in the preprint’s title, the paper only reports on vaccine efficacy “up to six months,” but not from six months. This is not semantics, as it turns out only 7% of trial participants actually reached six months of blinded follow-up (“8% of BNT162b2 recipients and 6% of placebo recipients had ≥6 months follow-up post-dose 2.”) So despite this preprint appearing a year after the trial began, it provides no data on vaccine efficacy past six months, which is the period Israel says vaccine efficacy has dropped to 39%. It is hard to imagine that the <10% of trial participants who remained blinded at six months (which presumably further dwindled after 13 March 2021) could constitute a reliable or valid sample to produce further findings.
Severe disease And on preventing death from covid-19, there are too few data to draw conclusions—a total of three covid-19 related deaths (one on vaccine, two on placebo). There were 29 total deaths during blinded follow-up (15 in the vaccine arm; 14 in placebo). The crucial question, however, is whether the waning efficacy seen in the primary endpoint data also applies to the vaccine’s efficacy against severe disease. Unfortunately, Pfizer’s new preprint does not report the results in a way that allows for evaluating this question.
_
Approval imminent without data transparency, or even an advisory committee meeting? …But here we are, with FDA reportedly on the verge of granting a marketing license 13 months into the still ongoing, two year pivotal trial, with no reported data past 13 March 2021, unclear efficacy after six months due to unblinding, evidence of waning protection irrespective of the Delta variant, and limited reporting of safety data. (The preprint reports “decreased appetite, lethargy, asthenia, malaise, night sweats, and hyperhidrosis were new adverse events attributable to BNT162b2 not previously identified in earlier reports,” but provides no data tables showing the frequency of these, or other, adverse events.) It’s not helping matters that FDA now says it won’t convene its advisory committee to discuss the data ahead of approving Pfizer’s vaccine. (Last August, to address vaccine hesitancy, the agency had “committed to use an advisory committee composed of independent experts to ensure deliberations about authorization or licensure are transparent for the public.”)
“..the jab allows vaccinated individuals to carry unusually high viral loads without becoming ill at first, potentially transforming them into presymptomatic superspreaders.”
• Fully Vaccinated Healthcare Workers Carry 251 Times Viral Load (McCullough)
A groundbreaking preprint paper by the prestigious Oxford University Clinical Research Group, published Aug. 10 in The Lancet, includes alarming findings devastating to the COVID vaccine rollout. The study found vaccinated individuals carry 251 times the load of COVID-19 viruses in their nostrils compared to the unvaccinated. While moderating the symptoms of infection, the jab allows vaccinated individuals to carry unusually high viral loads without becoming ill at first, potentially transforming them into presymptomatic superspreaders. This phenomenon may be the source of the shocking post-vaccination surges in heavily vaccinated populations globally. The paper’s authors, Chau et al, demonstrated widespread vaccine failure and transmission under tightly controlled circumstances in a hospital lockdown in Ho Chi Minh City, Viet Nam.
The scientists studied healthcare workers who were unable to leave the hospital for two weeks. The data showed that fully vaccinated workers — about two months after injection with the Oxford/AstraZeneca COVID-19 vaccine (AZD1222) — acquired, carried and presumably transmitted the Delta variant to their vaccinated colleagues. They almost certainly also passed the Delta infection to susceptible unvaccinated people, including their patients. Sequencing of strains confirmed the workers transmitted SARS-CoV-2 to one another. = This is consistent with the observations in the U.S. from Farinholt and colleagues, and congruent with comments by the director of the Centers for Disease Control and Prevention conceding COVID-19 vaccines have failed to stop transmission of SARS-CoV-2.
_
On Feb. 11, the World Health Organization indicated the AZD1222 vaccine efficacy of 63.09% against the development of symptomatic SARS-CoV-2 infection. The conclusions of the Chau paper support the warnings by leading medical experts that the partial, non-sterilizing immunity from the three notoriously “leaky” COVID-19 vaccines allow carriage of 251 times the viral load of SARS-CoV-2 as compared to samples from the pre-vaccination era in 2020. Thus, we have a key piece to the puzzle explaining why the Delta outbreak is so formidable — fully vaccinated are participating as COVID-19 patients and acting as powerful Typhoid Mary-style super-spreaders of the infection.
_
Vaccinated individuals are blasting out concentrated viral explosions into their communities and fueling new COVID surges. Vaccinated healthcare workers are almost certainly infecting their coworkers and patients, causing horrendous collateral damage. Continued vaccination will only make this problem worse, particularly among frontline doctors and nurses workers who are caring for vulnerable patients. Health systems should drop vaccine mandates immediately, take stock of COVID-19 recovered workers who are robustly immune to Delta and consider the ramifications of their current vaccinated healthcare workers as potential threats to high risk patients and coworkers.
“..prior infection and recovery produces durable and stable immunity in essentially everyone who has a competent immune system..”
• FDA Ignores Both Science and Law (Denninger)
So the FDA has “fully approved” the Pfizer jab for Covid. In doing so standing alone they have broken the law and thus have irrevocably destroyed their authority and any reason for anyone to ever do anything based on them ever again. Let me explain. Under black letter law an EUA is illegal if there is an alternative that is considered safe, effective and available. This was the reason the FDA did not (for 18 months!) run the studies and evaluate them on other early-intervention drugs for Covid-19. We all know what they are. I’m living proof they work too, as are millions of others worldwide. But, more-importantly, this “full approval” voids all other vaccine EUAs for Covid-19. That is, under the law the Moderna and J&J instantly became illegal to offer or use within the United States.
The makers can apply for full authorization, of course, but the EUAs are void as of this morning and under black letter law cannot be administered to anyone in the United States as they are now unlicensed and unlawful products in human beings until and unless they are given full approval themselves. No medical provider can offer or administer any other than the Pfizer Covid-19 shot in the United States as of the moment of that approval. You can bet the law will be ignored; note MRNAs stock price this morning. It should have instantly been cut in half. In addition the FDA broke the law itself when it issued the “approval.” The law requires a full hearing and the data from the full set of trials; the trials are not capable of being completed until early 2022 by the original submissions and they deliberately did not hold the hearing. This is a black letter violation of the law as well, but nobody cares.
_
As for me, I don’t give a crap. I’ve been infected, 98% certain it was Delta (because that’s all that’s circulating right now in the US where the index case I got infected by came from, and I know who it was) and am recovered. I hit it with meds immediately and I’m fine. I know, scientifically, it was Covid-19 and not some other virus as I now have IgG antibodies and did not for the previous 18 months which I know factually as I repeatedly tested myself. There is thus exactly zero medical benefit I can derive from the jabs. I will walk without fear into a Covid-19 ICU unit right now without any PPE on whatsoever.
_
I have no fear of this virus because as with every other viral infection of note including those that are much more-dangerous than Covid, such as measles, prior infection and recovery produces durable and stable immunity in essentially everyone who has a competent immune system, and I do. Those of you who trust the jabs to be equally effective to an active infection and recovery are free to come with me. I will bet my life that I’m sterile immune to the virus as a result of said infection and recovery. Are you willing to place the same bet, given the many known failures to protect by the shot, including Jesse Jackson and his wife, both of whom are in the hospital with Covid-19 despite being vaccinated in a very public spectacle in January of this year? There you have it.
“..the FDA will grant approval on results that were intentionally constructed to produce only one outcome.”
• Pfizer and Moderna Lost The Clinical Trial Control Group (CTH)
According to the New York Times and multiple media outlets, Pfizer is expected to get full FDA approval today. “The move would make it the first Covid vaccine to go from emergency use authorization to full FDA approval.” With that in mind, it is worth a reminder that both Pfizer and Moderna stopped the clinical trials the FDA was using in their review: The Moderna and Pfizer vaccine tests were conducted, as customary, with a control group; a group within the trial who were given a placebo and not the test vaccine. However, during the trial -and after the untested vaccines were given emergency use authorization- the vaccine companies conducting the trial decided to break protocol and notify the control group they were not vaccinated. Almost all the control group were then given the vaccine.
Purposefully dissolving the placebo group violates the scientific purpose to test whether the vaccine has any efficacy; any actual benefit and/or safety issues. Without a control group there is nothing to compare the vaccinated group against. According to NPR, the doctors lost the control group in the Johnson County Clinicial Trial (Lexena, Kansas) on purpose: “(Via NPR) […] “Dr. Carlos Fierro, who runs the study there, says every participant was called back after the Food and Drug Administration authorized the vaccine. “During that visit we discussed the options, which included staying in the study without the vaccine,” he says, “and amazingly there were people — a couple of people — who chose that.” He suspects those individuals got spooked by rumors about the vaccine. But everybody else who had the placebo shot went ahead and got the actual vaccine. So now Fierro has essentially no comparison group left for the ongoing study. “It’s a loss from a scientific standpoint, but given the circumstances I think it’s the right thing to do,” he says.
_
People signing up for these studies were not promised special treatment, but once the FDA authorized the vaccines, their developers decided to offer the shots. Just so we are clear, the final FDA authorization and approval for the vaccines are based on the outcome of these trials. As noted in the example above, the control group was intentionally lost under the auspices of “the right thing to do”, so there is no way for the efficacy, effectiveness or safety of the vaccine itself to be measured. There’s no one left within the control group, of a statistically valid value, to give an adequate comparison of outcomes for vaxxed -vs- non-vaxxed. This is nuts. That NPR article is one to bookmark when people start claiming the vaccination is effective. How can the vaccine not be considered effective when there is no group of non-vaccinated people to compare the results to?
_
Good grief, the entire healthcare system is operating on a massive hive mindset where science, and the scientific method, is thrown out the window in favor of ideological outcomes and self-fulfilling prophecies. The fact that the researchers and doctors, apparently under the payroll of the pharmaceutical companies that have a vested financial interest in the vaccine outcome, lost the control group on purpose is alarming. Of course, Big Pharma will promote the vaccine as beneficial, and the controlled media will promote that message with a complete disconnect from the clinical trial details, and the FDA will grant approval on results that were intentionally constructed to produce only one outcome.
Another video on informed consent is way below. Also from Canada.
• Everything You Need to Know About Informed Consent (21CW)
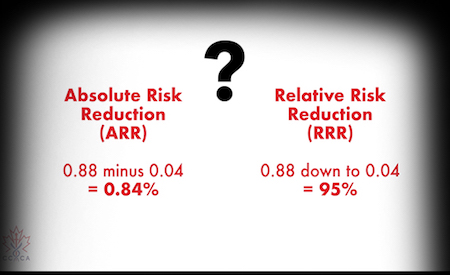
In Canada, informed consent to medical interventions – including vaccines – is the law. The same is true in the US, UK, EU, Australia, and New Zealand. But these governments, along with corrupt drug regulators, are now running roughshod over what were once sacrosanct laws prohibiting misleading and coercive medical procedures, and instead have unleashed a multibillion dollar media campaign of fear and mass-panic designed to pave-over the right to informed consent.
“Vaccine A is quite safe, and vaccine B is extremely dangerous. And yet the formula for PRR will produce the same result for vaccine A and B!”
• Statistical Fraud in the FDA Vaccine Approval Process (JoshM)
There are several systems for reporting vaccine reactions, including deaths, but the only one available to the public is VAERS. It is incomplete, because it relies on voluntary reporting, there is no incentive to report to VAERS, and it is a cumbersome process. We may compare reports of the COVID vaccines to past years, when there were also hundreds of millions of vaccinations, including annual flu shots and childhood vaccine schedules. The comparison is dramatic. There were more than twice as many deaths related to the COVID vaccines this year as the sum total of all vaccine deaths in the 30-year history of VAERS. Given this safety record, how is there any possibility of approval? Here is where the statistical fraud comes in. [I am grateful to have been alerted to this situation by Matthew Crawford]
The safety criterion they have chosen is an obscure computation called PRR for Proportional Reporting Ratio. As the name implies, it is based on RATIOS of different event types and is utterly blind to the ABSOLUTE RATE of such events. PRR measures the distribution of different kinds of adverse events, e.g. blood clots, heart attacks, and deaths. If those ratios are severely out of line with the great variety of vaccine reactions in the past, PRR would detect that. For example, if the new vaccines caused an extraordinary risk of myocarditis, but everything else was low, then PRR would flag that. But if myocarditis was just one risk among many that have been reported from past vaccines, then PRR would not pick that up.
_
The real scandal is that PRR is blind to the absolute risk numbers. PRR is defined in such a way as to look for unusual PATTERNS of adverse events, but it is completely insensitive to unusual RATES of adverse events. Of course, it is the rates and not the patterns that are of primary concern, and the PRR is designed NOT to reflect that.
For example, suppose we have 2 vaccines:
Vaccine A has 1 reported death per million vaccinations, 3 reported heart attacks per million, and 20 reported headaches per million.
Vaccine B has 1 reported death per hundred vaccinations, 3 reported heart attacks per hundred, and 20 reported headaches per hundred.
Vaccine A is quite safe, and vaccine B is extremely dangerous. And yet the formula for PRR will produce the same result for vaccine A and B!
_
Clearly, PRR is not an appropriate criterion for evaluating safety of any particular vaccine. Someone has arranged to cook the books.
“Regardless of the anti-science, despicable pieces regularly appearing in those outlets, such as suggesting that actually, masking kids is good for their learning ability.”
• The More Masks Fail, The More We Need Them (Ian)
The push for masking, as always, boils down to a combination of incompetence, cowardice, fear, and political pressure. Experts enjoy the ability to be seen as “doing something,” and must never appear to be “anti-mask,” since it would immediately discredit them in the eyes of their peers, the greater scientific community and their ideological compatriots. Politicians want the “get out of jail free” card that masking provides; the opportunity to blame others for poor results. The “it would have worked if you’d all just listened to me” line of defense. The media simply outsources all critical thinking to like-minded ideologues and refuses to acknowledge or take seriously the few brave experts willing to tell the truth.

And as a result, corporations, whose decision makers are exclusively influenced by the same media sources, like The New York Times, follow right along. Regardless of the anti-science, despicable pieces regularly appearing in those outlets, such as suggesting that actually, masking kids is good for their learning ability. But everywhere you look, the cultural groupthink is dramatically failing. Counties and states following the CDC’s new guidance are not succeeding, and those ignoring it are faring no worse. Locations that never removed masks, such as Hawaii and Japan, are seeing their highest numbers of the pandemic, but manage to escape the vitriol and hatred leveled at Ron DeSantis because they’re following orders and implementing what the hive mind of acceptable opinion mandates.
The dramatic, predictable failure resulting from the CDC’s science-ending reversal would, in a sane world, be cause for intellectually honest experts to revisit their guidance and accept that their efforts to “control” infections is always doomed to fail. But naturally, we’re seeing the exact opposite. The more masks fail, the more we need them.
Best VIDEO of 2020 pic.twitter.com/y3iK1ZoBFM
— Nicolas Teterel ∞/21 (@CryptojournalFr) August 19, 2021
One third has said they won’t comply. Maybe this is where the real fight will happen.
• Pentagon To Mandate Covid-19 Vaccinations For All Military Personnel (RT)
The Pentagon has said it will update its own guidance on Covid-19 vaccinations, mandating the jab for all military personnel, following the US drug regulator’s decision to fully approve the Pfizer vaccine. Speaking on Monday, US Department of Defense spokesman John Kirby said the military was aware of the Food and Drug Administration’s (FDA) decision to fully approve the Pfizer vaccine for use in people over 16, and was preparing to issue updated guidance to all service personnel. “We’re going to move forward making that vaccine mandatory,” Kirby told reporters. “We’re preparing the guidance to the force right now,” he stated, adding that the exact timetable for mandating the jab was still being worked out. Earlier on Monday, the FDA announced that the Pfizer jab had been fully approved for use in the US.
The shot has been administered under emergency-use authorization since mid-December 2020. The FDA added that the Pfizer vaccine will retain its emergency-use authorization for use in adolescents and for those requiring a third dose due to other health conditions. Earlier in August, the Washington Post reported that around 65% of active-duty military personnel were fully vaccinated, compared to around 59% of eligible Americans. Defense Secretary Lloyd Austin has previously encouraged all military personnel to get vaccinated against Covid. “To defend this nation, we need a healthy and ready force. I strongly encourage all DoD military and civilian personnel – as well as contractor personnel – to get vaccinated now and for military service members to not wait for the mandate,” Austin stated earlier in August.
“I do not expect a staffing shortage,” Porter said.”
• NYC Orders 150,000 Teachers & School Staff To Get Vaccinated (ZH)
As the NYT explained, education staffers are the first group of city workers to face a full vaccine mandate. The announcement also opens the door to a broader vaccine mandate of city workers, which the mayor said Monday the city was considering. Last month, Mayor Bill de Blasio issued a mandate for city workers that allowed for those unvaccinated to submit for weekly coronavirus testing. “We know this is going to help ensure that everyone is safe,” Mr. de Blasio said during a news conference on Monday, adding that city schools had extremely low virus transmission last year. The mandate, the mayor said, will help the city “build on that success.”
While the mayor’s push is likely to prove unpopular with many rank-and-file members; the city’s teacher’s unions, and unions representing other DoE staff, have signed off on the new mandate (though they’re still negotiating about what might happen to workers who continue to refuse). UFT President Michael Mulgrew acknowledged that the city had the legal right to impose the mandate, but he told reporters details were still being hashed out. The city announced last month that any teacher who failed to comply with both the vaccination requirement, and the required weekly testing for those who didn’t get the jab, would be suspended without pay.
“While the city is asserting its legal authority to establish this mandate, there are many implementation details, including provisions for medical exceptions, that by law must be negotiated with the U.F.T. and other unions, and if necessary, resolved by arbitration,” Mr. Mulgrew said in a statement. Mayor de Blasio has insisted that even if negotiations stall, the mandate will still be implemented. Meisha Porter, the chancellor of NYC’s schools, said she expects a high level of compliance from school staff on the mandate. “I do not expect a staffing shortage,” Porter said.
No clue how serious this is, but it’s a good idea.
• Truckers Threaten To Shut Down Australia Due to Covid Insanity (OI)
Australia seems to be in the grips of COVID-induced insanity as people across the country are vigorously protesting against the lockdown measures imposed to curb the spread of the renewed bout of coronavirus outbreak. After violent ruckus witnessed on the streets of major Australian cities, including Brisbane, Sydney and Melbourne, and dogs shot dead by a rural council in New South Wales to prevent volunteers from travelling during Covid restrictions, Australian truck drivers have threatened to shut down major highways across the country as a mark of protest against Covid lockdowns. Social media websites are awash with a video of a truck driver who said in his video that truck drivers are ‘planning to shut down the country’ to ‘remove the s*** government’.
He further warned the Aussies that their demonstration could end up choking supply chains and urged them to stock up on groceries to get them through the next couple of weeks. “It’s on. The truckies are doing it. The truckies are going to shut down the country,’ the man says in the video. What that means is you need to go shopping now, get what you can for the next week or two, load your fridge, freezers,” the truck driver could be seen saying in the video.
“The same progressives who regularly denounce “systemic racism” and “Western imperialism” are now enforcing policies that disproportionately punish minorities and the poor..”
• Keeping Fear Alive (Tierney)
Throughout the pandemic, American political and public-health leaders have been following Rahm Emanuel’s classic dictum for power-seeking officials: “You never want a serious crisis to go to waste.” Now they’ve adopted a corollary: you never want a crisis to end. So they are prolonging the national misery instead of easing it, which could be done with a few simple strategies. Explain to the public that the virus will never disappear but is no longer a mortal threat to the vast majority of Americans. Encourage the minority still at risk to get vaccinated by honestly discussing who is in jeopardy and what scientists have learned about infections. Promote treatments proven to prevent infection and speed recovery while avoiding unproven treatments and mandates that cause collateral damage and generate mistrust.
Above all, make it clear to Americans that we finally have reason to celebrate: what once seemed an unprecedented danger is now just one of many pathogens that we know how to live with. But the nation’s crisismongers aren’t about to relinquish their hold over the public, so they’ve set new goals that are as unachievable as they are unnecessary and harmful. Making vaccines available to every American adult is no longer sufficient; now the crisis cannot end until the entire population has been vaccinated. Instead of focusing efforts on vaccinating the vulnerable, officials obsess on compelling universal obedience, even if that means squandering vaccines on people who already have acquired natural immunity or are at minimal risk of serious illness.
_
The same progressives who regularly denounce “systemic racism” and “Western imperialism” are now enforcing policies that disproportionately punish minorities and the poor, both in the United States (the majority of black teenagers and young adults in New York have been banished from much of public life by the city’s new vaccine-passport policy) and in the rest of the world. The hypocrisy was deftly captured in a tweet by Martin Kulldorff, the Harvard epidemiologist: “If you favor university vaccine mandates for low-risk American and European students, when there is not enough vaccine for older high-risk people in Asia, Africa and Latin America, please remove your #BLM tags from your Twitter/Facebook profiles.”
Children are being sentenced to another round of unnecessary mask mandates and probably more school closures based on evidence-free warnings from Anthony Fauci and others that the Delta variant will be more deadly to them than the original virus. While the variant is more infectious, the evidence does not show it to be any more lethal. In fact, the current mortality rate among American children with Covid is lower than it was last year—and last year many more children died of the flu than of Covid. One of the most thorough studies, in England, shows that the survival rate for those under 18 with Covid is 99.995 percent. But instead of emphasizing these reassuring statistics, public-health officials like Jerome Adams, the surgeon general, keep looking for new ways to scare parents and children.
_
“I’m an anesthesiologist,” he tweeted last weekend. “And a dad. And I can assure you in both capacities that your child will be far more comfortable if they’re in a face mask, than on a ventilator. If you’re making a choice on behalf of a child, please choose based on their comfort, vs yours.” He offered no new evidence that children are at heightened risk from the virus, much less any evidence that a mask would make any difference, but he did make sure to include a gruesome photograph of a child on a ventilator. It was a new low in public-health demagoguery, but unfortunately not so different from the fearmongering of other officials, the press, and social-media platforms. They lament that a minority of the public remains reluctant to get vaccinated without recognizing that their own tactics are a likely a chief cause of this reluctance. They have been misleading people for so long—and censoring challenges to their misinformation—that it’s no wonder polls show that an overwhelming majority of unvaccinated Americans say they don’t trust Fauci or the CDC.
Nation-building in Afghanistan arrived in 2001. Western interventions into the old Eastern bloc in the 1980s and early 1990s had been spectacularly effective in destroying the old social and institutional order; but equally spectacular in failing to replace imploded societies with fresh institutions. The threat from ‘failed states’ became the new mantra, and Afghanistan – in the wake of the destruction wrought post-9/11 – therefore necessitated external intervention. Weak and failed states were the spawning ground for terrorism and its threat to the ‘global order’, it was said. It was in Afghanistan that a new liberal world vision was to be stood-up.
At another level, the war in Afghanistan became another sort of crucible. In very real terms, Afghanistan turned into a testbed for every single innovation in technocratic project management – with each innovation heralded as precursor to our wider future. Funds poured in: Buildings were thrown up, and an army of globalised technocrats arrived to oversee the process. Big data, AI and the utilization of ever expanding sets of technical and statistical metrics, were to topple old ‘stodgy’ ideas. Military sociology in the form of Human Terrain Teams and other innovative creations, were unleashed to bring order to chaos. Here, the full force of the entire NGO world, the brightest minds of that international government-in-waiting, were given a playground with nearly infinite resources at their disposal.
This was to be a showcase for technical managerialism. It presumed that a properly technical, and scientific way of understanding war and nation-building would be able to mobilize reason and progress to accomplish what everyone else could not, and so create a post-modern society, out of a complex tribal one, with its own storied history.
The ‘new’ arrived, as it were, in a succession of NGO boxes marked ‘pop-up modernity’. The 18th century British statesman Edmund Burke, of course, had already warned in Reflections on the Revolution in France, as he witnessed the Jacobins tearing down their old order: “that it is with infinite caution” that anyone should pull down or replace structures that have served society well over the ages. But this managerial technocracy had little time for old ‘stodgy’ ideas.
But, what last week’s fall of the western instituted regime so clearly revealed is that today’s managerial class, consumed by the notion of technocracy as the only means of effecting functional rule birthed instead, something thoroughly rotten — “data-driven defeat”, as one US Afghan veteran described it — so rotten, that it collapsed in a matter of days. On the extended blunders of the “system” in Afghanistan, he writes:
“A retired Navy SEAL who served in the White House under both Bush and Obama reflected,[that] “collectively the system is incapable of taking a step back to question basic assumptions.” That “system” is best understood, not simply as a military or foreign policy body, but as a euphemism for the habits and institutions of an American ruling class that has exhibited an almost limitless collective capacity for deflecting the costs of failure.
“This class in general, and the people in charge of the war in Afghanistan in particular, believed in informational and management solutions to existential problems. They elevated data points and statistical indices to avoid choosing prudent goals and organizing the proper strategies to achieve them. They believed in their own providential destiny and that of people like them to rule, regardless of their failures”.
Whatever was not corrupt before America arrived, became corrupt in the maelstrom of that $2 Trillion of American money showered on the project. American soldiers, arms manufacturers, globalised technocrats, governance experts, aid workers, peacekeepers, counter-insurgency theorists and lawyers — all made their fortunes.
The flaw was that Afghanistan as a liberal progressive vision was a hoax in the first place: Afghanistan was invaded, and occupied, because of its geography. It was the ideal platform from which to perturb Central Asia, and thus unsettle Russia and China.
No one was truly committed because there was really no longer any Afghanistan to commit to. Whomsoever could steal from the Americans did so. The Ghani regime collapsed in a matter of days, because it was ‘never there’ to begin with: A Potemkin Village, whose role lay in perpetuating a fiction, or rather the myth of America’s Grand Vision of itself as the shaper and guardian of ‘our’ global future.
The true gravity for America and Europe of the present psychological ‘moment’ is not only that nation-building, as a project intended to stand up liberal values been revealed as having ‘achieved nothing’, but Afghanistan débacle has underlined the limitations to technical managerialism in way that is impossible to miss.
The gravity of America’s present psychological ‘moment’ – the implosion of Kabul – was well articulated when Robert Kagan argued earlier, that the ‘global values’ project (however tenuous its basis in reality) nonetheless has become essential to preserving ‘democracy’ at home: For, he suggests, an America that retreats from global hegemony, would no longer possess the domestic group solidarity to preserve America as ‘idea’, at home, either.
What Kagan is saying here is important — It may constitute the true cost of the Afghanistan débacle. Every élite class advances various claims about its own legitimacy, without which a stable political order is impossible. Legitimating myths can take many forms and may change over time, but once they become exhausted, or lose their credibility – when people no longer believe in the narrative, or the claims which underpin that political ‘idea’ – then it is ‘game over’.
Swedish intellectual, Malcolm Kyeyune writes that we may be “witnessing the catastrophic end of this metaphysical power of legitimacy that has shielded the managerial ruling class for decades”:
“Anyone even briefly familiar with the historical record knows just how much of a Pandora’s box such a loss of legitimacy represents. The signs visibly have been multiplying over many years. When Michael Gove said, “I think the people in this country have had enough of experts” in a debate about the merits of Brexit, he probably traced the contours of something much bigger than anyone really knew at the time. Back then, the acute phase of the delegitimization of the managerial class was only just beginning. Now, with Afghanistan, it is impossible to miss”.
There is therefore, little mystery as to why the Taliban took over Kabul so quickly. Not only did the project per se lack legitimacy for Afghans, but that aura of claimed expertise, of technological inevitability that has protected the élite managerial class, has been exposed by the sheer dysfunctionality on display, as the West frantically flees Kabul. And it is precisely how it has ended that has really drawn back the curtain, and shown the world the rot festering beneath.
When the legitimating claim is used up, and people no longer believe in the concepts or claims that underpin a particular system or claim to rule, the extinction of that particular élite, Kyeyune writes, becomes a foregone conclusion.
Since COVID-19 emerged in Canada in March 2020, what physicians, scientists, public health
officials and citizens have understood about the virus and how to address it has changed drastically. The continually evolving information overload is understandably confusing and overwhelming, and the conflicts between information can be difficult to validate.
The following considerations may help you to more clearly consider these challenges:
| Public Perceptions | Evidence-Based Considerations |
|---|---|
| COVID-19 poses a serious threat to public health. | Risk varies with age and comorbidities. Children, adolescents and young adults have a very low risk of hospitalization or death from COVID-19. |
| There is no available, effective, approved treatment for COVID-19. | There are known safe drug protocols that are effective in COVID-19 treatment and prevention. |
| Because healthy people are considered to transmit the virus, restrictions (including social distancing and lockdowns) are the best way to reduce transmission of COVID-19. | Numerous studies have found that healthy people do not significantly contribute to transmission of the virus. Research has shown that the majority of people who have recovered from COVID-19 have developed immunity and do not transmit the virus. Targeted early treatment and empowering people to build healthy, meaningful, socially connected lives is essential to personal well being and public health. |
| COVID-19 vaccines are necessary, safe, and effective (“the benefits outweigh the risks”), and the fastest and only way to get back to, and perpetually maintain normal life. | The methods used to justify rapid COVID-19 vaccine development and rollout do not adequately measure necessity, safety, and efficacy. There have been an unprecedented number of deaths and serious, lifealtering adverse reactions occurring shortly after COVID-19 vaccination. Contrary to initial scientific assumption, the lipid nanoparticles in the COVID-19 vaccines do not stay at the injection site but travel throughout the body, cross the blood-brain barrier, and have been shown to accumulate in sensitive tissues including bone marrow and ovaries. Much remains unknown about the extremely serious short and long term adverse effects and dangers of the COVID-19 vaccines. These risks need to be independently investigated immediately and resolved before continuing with mass vaccination. |
| All COVID-19 vaccines are fully approved. | COVID-19 vaccines are authorized for use “under interim order” and are therefore investigational. The current experimental phases are not due to be completed until 2023 or 2024. |
| “The Science” is settled; anything contrary to the official narrative is not science. | “The Science” is not settled; competing evidence about COVID-19 is growing from many highly-credentialed sources and challenges the official narrative. Compelling scientific evidence is being ignored or censored. In valuing principles of equity, diversity, and inclusion, we need to encourage multiple ways of knowing, and develop public health protocols that are evidence informed and responsive to the overall health and well being of our individuals and communities. |
Dialogue over these issues is difficult, divisive, and threatens to tear us apart. As we navigate this rapidly evolving situation, we believe some ethical and legal principles should remain constant in a free and democratic society:
- First and foremost, the right and responsibility of adults to make their own decisions about their health and to be accorded respect for questioning mandates that have farreaching social implications
- Free, voluntary and “informed consent”
- Human rights and responsibilities
- Fiduciary duties for all governing authorities and adherence to professional and institutional ethical codes of conduct
- Evidence, matters of conscience, and precaution as fundamental to medical decisionmaking
- Honest and open inquiry
As caring and responsible individuals, it is crucial that we remain open to listening to each other, continuing to ask questions, and recognizing that we are all doing the best we can to keep those we love safe. This is especially true regarding concerns about scientific and medical issues which have a huge impact on the health and welfare of our population. Our COVID-19 resources are offered as learning tools. Feel free to use the information, forms and FAQs as resources with which to engage your government, representatives, health care providers, family and friends.

In his March 17, 2020, article in Stat, Stanford epidemiologist Dr. John Ioannidis argued for a vast reconsideration of the societal response to the emerging SARS-COV-2 pandemic, commonly called Covid-19. For unknown reasons, the scientific and medical tradition forming the foundation for how to respond to pandemics was being quickly disbanded. Abandoning such previously established traditions entailed filling the void with the appearance of a new global consensus: The combination of unending non-pharmaceutical interventions (masks, social distancing, etc.) and universal vaccination was the key that would end the pandemic.
The totalizing power of this new global pandemic consensus has certainly been effective over the last year and a half. However, the last month and a half has brought about a palatable instability to this apparently once-certain agreement.
Until now, Corona policy in every western country has unfolded more or less according to the same script, devised by the World Health Organization at the end of February 2020. The final act was supposed to be the wide-scale eradication of Corona after mass vaccination. It is now clear that this will never happen. For the first time since March 2020, there is no obvious international consensus on the way forward.
The global political and health managers of Western nations and their media allies increasingly seem uncertain as to where to go next. Lurking behind the uncertainty of how to respond to the variants, however, is the last remaining consensus. And while it is the last remaining consensus, it has been a little-known, yet real, part of the script from the beginning. It is as simple as it is all-encompassing: Use every available means possible to assault early treatment of the virus.
Consider one of the latest displays of this charade. Many have now seen, or heard about, the American podcaster Joe Rogan’s recent experience with Covid-19. After recognizing some of the common symptoms of Covid-19, Rogan decided to “throw the kitchen sink at it.” Following the insights offered by Dr. Peter McCullough and his multi-drug treatment protocol, Rogan pursued infusion of monoclonal antibodies. Along with antibody infusion, Rogan took a cocktail that consisted of ivermectin, Azithromyicin, the corticosteriod Predinsone, and high doses of vitamin D (through drip line). Within 72 hours after beginning the treatment regimen, Rogan declared that he felt great, and had practically recovered from the virus.
We would not have needed the gift of prophecy to have predicted what followed: The Covid machine was deployed to attack Rogan. The inspiration for the assault has been helped by a recent tweet from the FDA, which read: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” Moving on from its initial onslaught against the effective early use of hydroxychloroquine, the global consensus has now overwhelmingly shifted its ire to ivermectin. Coinciding with the attack on Rogan was a supposed news story from Rolling Stone, which claimed that access to emergency care for gunshot victims at an Oklahoma hospital was threatened due to the number of patients who had been poisoned by overdosing on ivermectin. The hospital offered a clarification that denied the claims, which had been made by a former employee. And yet, only updates have been added; thus far, the story has not been retracted.
This widespread jettisoning of the principle and effectiveness of preventative and early treatment has been described as “therapeutic nihilism.” Nearly two years into this pandemic, getting early treatment for Covid-19 that can prevent hospitalization and death is still extremely difficult. Continued attempts to undermine early treatment protocols, as well as frequented campaigns against those who are skeptical of the prevailing narrative, give the impression that certain interested parties are hesitant to bring the pandemic to an end.
The global managers writing and executing the Covid script are using it to manipulate the populace. I am reminded of the Polish philosopher and statesman Ryszard Legutko’s 2016 book The Demon in Democracy: Totalitarian Temptations in Free Societies. Following the collapse of totalitarianism regimes in 1989, Legutko began noticing something that was as confusing as it was unsettling. Supporters of communism appeared to find a somewhat comfortable home in liberal democratic societies. In an attempt to parse out and understand this political phenomenon, Legutko came to realize some shared similarities between the principles of communism and modern liberal democratic regimes:
Communism and liberal democracy proved to be all-unifying entities compelling their followers how to think, what to do, how to evaluate events, what to dream, and what language to use. They both had their orthodoxies and their models of an ideal citizen. [Emphasis added]
What Legutko’s diagnosis reveals is that the global response to the pandemic has been utilized to accelerate the conditions whereby rigorous and independent thinking may be snuffed out. The pandemic seems to have accelerated the project of Western nations transmuting into large, mechanizing systems oriented towards uniformity of thought and practice.
Here is Stanford’s Ioannidis commenting upon this disturbing integration of rapidly declining transparency and collectivism:
The retraction of a highly visible hydroxychloroquine paper from the The Lancet was a startling example: A lack of sharing and openness allowed a top medical journal to publish an article in which 671 hospitals allegedly contributed data that did not exist, and no one noticed this outright fabrication before publication. The New England Journal of Medicine, another top medical journal, managed to publish a similar paper; many scientists continue to heavily cite it long after its retraction.
Such a situation reveals the emptiness of supposed concerns about “evidence.” Abused tropes such as “follow the science” are revealing themselves to be nefarious power grabs seeking to destroy nuance. “Good” citizens should not even consider the possibility of calling into question the prevailing narrative regarding Covid. More specifically, it is anathema to even fathom the thought that preventative and early treatment should be a fundamental pillar of the response to a pandemic.
As the consensus equating vaccination with the elimination of the virus continues to weaken, Ioannidis’s original prediction continues to be persuasive: The response to SARS-COV-2 will eventually be seen as a “once in a century evidence fiasco.” But the citizens of Western nations must think critically for themselves if the coils of the Covid machine have a chance of being loosened.
Brian Jones is a Ph.D. candidate in philosophy in the Center for Thomistic Studies at the University of St. Thomas.
For more about the “Taking the Mask Off” series, click here.

The three monkeys at the Toshogu Shinto temple. They illustrate the precept of a Chinese sage: "Say nothing wrong, see nothing wrong, hear nothing wrong. They could also illustrate Western cowardice: "Say nothing of the Truth, see nothing of the Truth, hear nothing of the Truth.”
The celebrations of the 20th anniversary of the attacks of September 11, 2001 give rise to two absolutely contradictory narratives, depending on whether one refers to the written and audio-visual press or to the digital press. For some, Al Qaeda declared war on the West by plotting a high-profile crime, while for others the same crime masked a domestic coup d’état in the US.
Any debate is impossible between the supporters of these two versions. Not because both sides refuse it, but because the supporters of the official version -and only they- refuse it. They consider their opponents as "conspiracy theorists", that is to say, in their mind, at best fools, at worst evil people, accomplices -willing or not- of terrorists.
From now on, this disagreement applies to any major political event. And the worldview of the two camps keeps distancing itself from each other.
How could such a fracture between fellow citizens occur in societies that aspire to democracy? Especially since, not this fracture, but the reaction to this fracture makes any democracy impossible.

The continuous news channels privilege the speed of the retransmission of an event. They do not have the time to contextualize it and even less to analyze it; functions which are the proper of journalism. The viewer becomes a voyeur of things he does not understand.
A certain conception of journalism
We are assured today that the role of journalists is to report faithfully what they have seen. Yet when we are interviewed by a local media outlet about a story we know about and see how they have handled it, we are often disappointed. We feel that we have not been understood. Some of us lament that we have come across the wrong journalist and retain our trust in the mainstream media. Others feel that while a little distortion is possible on small issues, a lot more must be done on more complex ones.
In 1989, a crowd attending one of his speeches heard the Romanian dictator, Nicolae Ceaușescu, accuse the fascists of having invented the Timișoara massacre attributed to his regime’s torturers. Revulsed by this denial, the crowd revolted, chanting "Ti-mi-șoa-ra! Ti-mi-șoa-ra!" and overthrew him. The local television station in Atlanta (USA), CNN, broadcast live the few days of this revolution. It thus became the first live news channel and turned into an international channel. However, we know today that this massacre never existed. It was only a staged event using corpses taken from a morgue. It was later learned that a propaganda unit of the US Army had an office adjacent to the CNN newsroom.
The Timișoara manipulation only worked because it was live. Viewers had no time to check or even think. Professionally, no journalist ever drew any conclusions from the event. On the contrary, CNN became the model for the live news channels that have sprung up everywhere.
During the Kosovo war, in 1999, I was producing a daily bulletin summarizing the information from NATO and the regional news agencies (Austria, Hungary, Romania, Greece, Albania, etc.) to which I had subscribed [1]. From the beginning, what Nato was telling us in Brussels was not confirmed by the regional agencies. On the contrary, they described a completely different conflict. It was strange to see that the regional journalists, from all countries except Albania, formed a block, writing texts that were compatible with each other, but not with those of NATO. Week after week, the two versions were moving away from each other.
I n response to this situation, NATO put Jamie Shea in charge of its communications. He told a new story every day from the battlefield. The international press soon had eyes only for him. His story became the media story and the regional news agencies were no longer covered except by me. In my mind, both sides were lying and the truth had to be somewhere in between.
When the war was over, humanitarians, diplomats and UN soldiers rushed to Kosovo. To their surprise - and mine - they found that the local journalists had accurately reported the truth. Jamie Shea’s words had been nothing but war propaganda. They had been the only "reliable" source for the international media for three months.
Western journalists who went to Kosovo also found that they had trusted people who had lied to them with aplomb. Yet few of them changed their tune. And even fewer managed to convince their editors that NATO had deceived them. The narrative imposed by the Atlantic Alliance had become the Truth that the history books would repeat despite the facts.

We accept to be deceived when we think the Truth is too hard to admit.
Ancient Greece and the Modern West
In ancient Greece, plays caused strong emotions in the audience. Some feared that the gods would drag them into dark destinies. So gradually the chorus, which narrated the story, also began to explain that one must not be fooled by what one saw, but to understand that it was only a staged show.
This distancing from appearances, which is paralyzed by the myth of live information, is called in psychology the "symbolic function". Small children are incapable of this, they take everything seriously. However, at the "age of reason", at 7 years old, we can all make the difference between what is true and what is only a representation.
Reason here is opposed to rationality. To be rational is to believe only in things that are proven. To be reasonable is not to believe in impossible things. This is a very big difference. Because we don’t find the Truth with beliefs, but with facts.
When we see airplanes hitting the World Trade Center in New York and people jumping out of windows to escape the fire, we are all very moved. When the Towers collapse, we are ready to weep. But that should not stop us from thinking [[2](#nb2 "On the political significance of the September 11 attacks, read: "20th (...)")].
We can always be told that 19 hijackers hijacked four airplanes, but since these people were not on the airline’s lists of passengers on board, they could not hijack these planes.
One can always tell us that the fuel from the two burning planes slipped onto the pillars of the buildings and melted them, which would explain why the Twin Towers collapsed, but not on themselves, and not the collapse of the third tower. For a building to collapse, not on one side, but on itself, you have to blow up its foundations, then blow it up from top to bottom to destroy the floors on themselves.
One can always tell us that panic-stricken passengers phoned their relatives before dying, but since the telephone companies have no record of these calls, they did not exist.
One can always tell us that a Boeing destroyed the Pentagon, but it could not have entered through a porte cochere without damaging the doorframe.
The testimonies contradict each other. But only some are contradicted by the facts.
We accept to be deceived when we think the Truth is too hard to admit.
Why we accept to be deceived
There remains a big problem: why do we accept to be deceived? Usually because the Truth is harder for us to accept than the lie.
For example, when for years the son of the president of the National Political Science Foundation denounced the rapes he was subjected to by the president, everyone pitied the poor delusional boy and praised his father for enduring his madness without saying a word. When the victim’s sister published a book of testimonies, everyone realized who was telling the truth. The president was forced to resign. The rapist owes his escape from justice only to his status: former European deputy, president of the emblematic institution of the entire French political-media class and president of the Siècle, the most exclusive private club in France.
Why do we believe that Al Qaeda is responsible for the 9/11 attacks? Because the Secretary of State, General Colin Powell, came before the United Nations Security Council and swore it. It doesn’t matter that he lied years earlier when he validated the story of the incubators stolen from Kuwait by the Iraqis and the babies left to die. Or that he lied later about President Saddam Hussein’s weapons of mass destruction. He is a Secretary of State and we must believe him.
On the contrary, if we question his word, we should not only ask why we invaded Afghanistan, then Iraq, and so on. But also and above all why he lied.

The irremovable Anthony Fauci has managed every major epidemic in the US. He does not work as a doctor, but as a senior civil servant. He does not care about the Hippocratic oath. He has not hesitated to embezzle public money to sponsor illegal and dangerous research in a distant country. Or to promote the compulsory confinement of healthy people.
The reaction to Covid-19: another 9/11
The enigma of 9/11 is not a question of the past. Our understanding of the last twenty years depends on how it is answered. As long as we do not have contradictory debates between the two versions, we will reproduce this fracture on all global issues.
We are currently experiencing another catastrophe, the Covid-19 pandemic. We have all seen a large laboratory, Gilead Science, bribe the editors of the medical journal The Lancet to denigrate a drug, hydroxychloroquine. Gilead Science is the company formerly headed by the 9/11 Secretary of Defense, Donald Rumsfeld. It is also the company that produces a drug against Covid-19, Remdesivir. In any case, no one dared to look for drugs to treat Covid anymore. Everyone turned to the hope of vaccines.
Donald Rumsfeld had instructed his staff to develop protocols in case of a bioterrorist attack on US military bases abroad. Then he asked one of them, Dr. Richard Hachett, who was a member of the US National Security Council, to extend this protocol to an attack on the US civilian population. It was this man who proposed the compulsory confinement of healthy populations, provoking an outcry from American doctors, led by Professor Donald Henderson of John Hopkins University [3]. For them, Rumsfeld, Hatchett and their advisor, the senior civil servant Anthony Fauci, were enemies of the Hippocratic oath and of humanity.
When the Covid-19 epidemic occurred, Dr. Richard Hatchett had become the director of CEPI (Coalition for Epidemic Preparedness Innovations); an association created at the Davos Forum and funded by Bill Gates. It was Hatchett who first used the expression "We are at war", which was taken up by his friend President Emmanuel Macron. It was he who advised confining healthy populations as he had imagined 15 years earlier in the "war on terror." Anthony Fauci, on the other hand, was still at his post. He had embezzled federal money to finance illegal research in the United States. The research was conducted for him at the Chinese laboratory in Wuhan.
Normally, the medical professions would have risen up again against the compulsory confinement of healthy people. This did not happen. They overwhelmingly considered that the situation required violating the Hippocratic oath.
Today, the Western countries that followed Dr. Hatchett’s advice and believed Gilead Science’s lies have a terrifying record of this pandemic. The United States has 26 times more deaths per million people than China. And its economy is devastated.
This would deserve some debate and explanation, but no. We prefer to see our societies fractured again between supporters of Anthony Fauci or Professor Didier Raoult.
Conclusion
Instead of talking to each other, of confronting our arguments, we organize false debates between the supporters of the dominant doxa and those of the most grotesque opinions possible.
It is useless to aspire to live in a democracy, if we refuse to really discuss the most important subjects.

[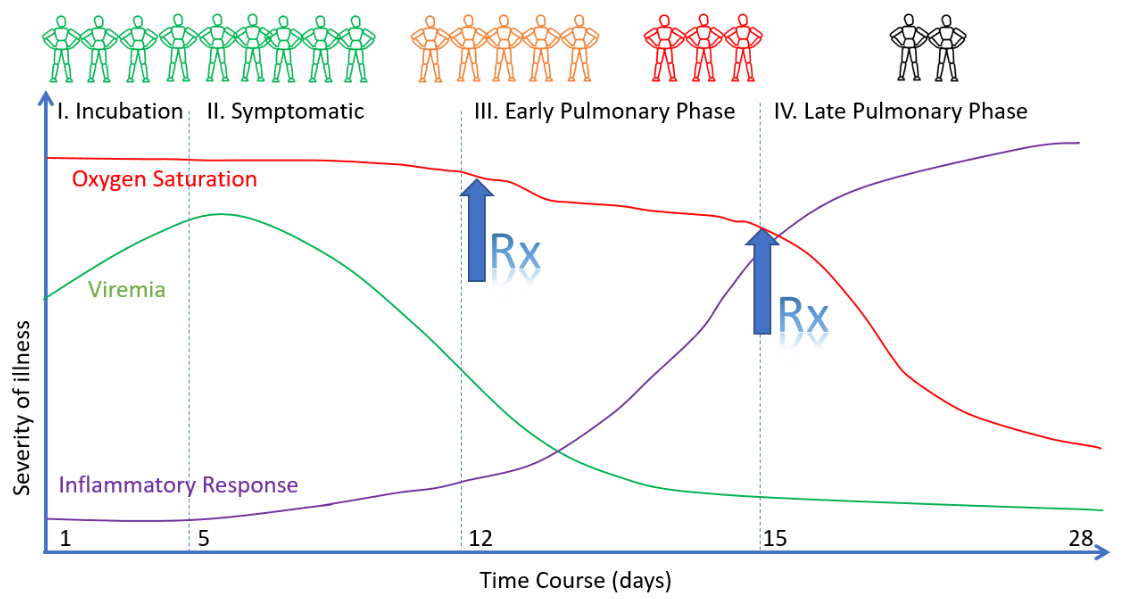
](https://swprs.org/wp-content/uploads/2020/08/covid-stages.png)
Stages and treatment of covid disease (EVMS)
Updated: September 2021
Languages: German, English
Share on: Twitter / Facebook
Based on the available scientific evidence and current clinical experience, the SPR Collaboration recommends that physicians and authorities consider the following covid-19 treatment protocol for the prophylactic and early treatment of people at high risk or high exposure.
Numerous international studies have shown that prophylactic and early treatment can significantly reduce the risk of severe and fatal covid-19 (see scientific references below).
Note: Patients are asked to consult a doctor.
Treatment protocol
Prophylaxis
- Vitamin D3 (2000 IU per day)
- Vitamin C (500mg per day)
- Zinc (20mg to 30mg per day)
- Quercetin (250mg per day)
- Mouthwashes and nasal spray
Early treatment
- Zinc (75mg to 100mg per day)
- Quercetin (500mg per day)
- Aspirin (325mg per day)*
- Bromhexine (48mg per day)*
- Artemisia annua (extract)
- Mouthwashes and nasal spray
Prescription only
- High-dose calcifediol*
- Sulodexide (LMW heparin)*
- Fluvoxamine or cyproheptadine*
- Steroids: Prednisone or budesonide*
- Monoclonal antibody treatment
- Anti-androgen treatment
- Ivermectin (see below)
(*) Notes
- The early treatment phase includes post-exposure prophylaxis (PEP).
- Bromhexine is available prescription-free in most of Europe, but not in the US.
- Steroids and cyproheptadine are only used if respiratory symptoms develop.
- Counterindications and maximum dosages must be observed for all drugs.
- On hydroxychloroquine (HCQ), see Severe covid: A postviral autoimmune attack
See also
- FLCCC Covid-19 Prophylaxis and Treatment Protocols (FLCCC)
- Early Outpatient Treatment of COVID-19 (McCullough et al.)
- Covid-19 Early Treatment Study Overview (c19early.com)
Treatment studies
Results of trials and studies on the early treatment of covid.
Ivermectin
Ivermectin (an antiparasitic drug) has anti-viral and anti-inflammatory properties.
- Several controlled and observational studies on ivermectin found anti-viral and anti-inflammatory effects and a significant reduction in covid morbidity and mortality.
- However, once low-quality studies are excluded from the analysis, the benefit is no longer statistically significant, although a limited benefit might still be possible.
- Due to a lack of large high-quality trials, the WHO, the US FDA and the European EMA do not recommend using ivermectin against covid outside of clinical trials.
- Read more: The Ivermectin Debate (SPR)
**Zinc and quercetin
**
Zinc inhibits RNA polymerase activity of coronaviruses and thus inhibits virus replication. Quercetin (a plant polyphenol) supports the cellular absorption of zinc and has additional anti-viral properties.
- A Spanish study found that low plasma zinc levels (below 50mcg/dl) increased the risk of in-hospital death of covid patients by 130%.
- US studies found an 84% decrease in hospitalizations and a 45% decrease in mortality based on risk-stratified early treatment with zinc and HCQ.
- A US case study reported a rapid resolution of covid symptoms, such as shortness of breath, based on early outpatient treatment with high-dose zinc.
- An Italian randomized trial found a significantly reduced hospitalization rate and mortality in covid patients receiving quercetin.
Bromhexine
Bromhexine (a mucolytic cough medication) inhibits the expression of cellular TMPRSS2 protease and thus the entry of the virus into the cell, as first described in 2017.
- A randomized Iranian trial with 78 patients found a decrease in intensive care treatments of 82%, a decrease in intubations of 89%, and a decrease in deaths of 100%.
- A Chinese trial found a 50% reduction in intubations in patients receiving bromhexine.
- A Russian study found a faster recovery in hospitalized patients receiving bromhexine.
- A Russian prophylaxis study found a reduction in symptomatic covid from 20% to 0%.
Vitamin D3
Vitamin D3 supports and improves the immune system response to infections.
- A Spanish randomized controlled trial found a 96% reduction in the risk of requiring intensive care in patients receiving high-dose vitamin D (100,000 IU).
- Another randomized trial in Spain with 930 hospitalized patients found a reduction in ICU treatment of 80% and in mortality of 60% in patients receiving high-dose vitamin D.
- A study in a French nursing home found an 89% decrease in mortality in residents who had received high-dose vitamin D either shortly before or during covid-19 disease.
- A retrospective British study of approximately 1000 hospitalized covid patients found an 80% reduction in mortality with high-dose vitamin D.
- A large Israeli study found a strong link between vitamin D deficiency and covid-19 severity.
- For an overview of all covid-19 vitamin D studies, see here.
**Aspirin and heparin
**
Aspirin and heparin have anti-platelet and anti-thrombotic effects.
- A meta-study including 15,000 patients found a reduction in covid mortality of 53% in patients who were receiving aspirin as early or prophylactic treatment.
- A study published in PLOS One found a reduction in covid mortality at 30 days from 10.5% (control group) to 4.3% (with aspirin) in 70,000 US veterans taking aspirin.
- A retrospective US study with 400 patients found a reduction in ICU treatments by 43% and a reduction in mortality by 47% in the group of patients treated early with aspirin.
- A Mexican randomized controlled trial found a 40% reduction in hospitalization in patients receiving sulodexide (a heparin combination).
Artemisia annua (powder, extract, or tea)
Artemisia annua plant extract has known antimalarial and antiviral properties.
- An in vitro study by the German Max Planck Institute, published in Nature Scientific Reports, found artemisia annua to be effective against SARS-CoV-2 at realistic doses.
- An in vitro study by US researchers, published in the Journal of Ethnopharmacology, found artemisia annua hot-water extracts to be effective against SARS-CoV-2 replication.
- In a small clinical trial, published in Antimicrobial Agents, the viral load decreased significantly faster in covid patients treated with artemisinin-piperaquine.
- In a 2005 in vitro study, published in Antiviral Research, artemisia annua was already identified as effective against the original SARS-1 virus.
- In Madagascar, the first country to apply Artemisia annua extract against covid, covid and all-cause mortality has remained very low, even for African standards.
- In a simulation study by a Harvard group, the anti-malaria drug amodiaquine was identified as most effective against SARS-CoV-2 replication.
Mouthwashes and nasal sprays
Mouthwashes and nasal sprays target the initial infection and viral replication.
- Several small studies found that mouthwashes (gargling) based on povidone-iodine and nasal sprays based on povidone-iodine or nitric oxide may prevent a coronavirus infection or reduce its duration or symptoms (more about this).
- The German Society for Hospital Hygiene (DGKH) recommends anti-viral mouthwashes and nasal sprays for prophylaxis and early treatment.
- Some observers argued that traditional nasal rinsing and gargling practices in South East Asia may have helped successfully limiting coronavirus infections in these countries.
- Israel started mass production of nasal sprays based on nitric oxide in early 2021.
Anti-androgen treatment
Anti-androgen treatment inhibits the expression of the TMPRSS2 cellular protease used by SARS-CoV-2, which is driven by androgen hormones (i.e. male sexual hormones).
- A first randomized, double-blinded and placebo-controlled trial in Brazil found that proxalutamide reduced hospitalization rates in male patients by 91%.
- Another randomized, double-blinded and placebo-controlled trial in Brazil found that proxalutamide reduced mortality in hospitalized patients (male and female) by 78%.
- However, the two Brazilian trials have been criticized by other researchers.
- Previous studies found that men receiving anti-androgens – typically used against prostate cancer or hair loss – were at a much lower risk of severe covid.
Fluvoxamine and Cyproheptadine
These drugs inhibit serotonin-induced pulmonary vasoconstriction.
- The TOGETHER trial found that fluvoxamine outpatient treatment of covid patients reduced disease progression (hospitalizations or ER visits) significantly by 29%.
- The results of two preliminary US trials indicate that early treatment with fluvoxamine may reduce the risk of severe covid, hospitalization and death to near zero.
- Fluvoxamine and cyproheptadine target serotonin metabolism and serotonin-induced pulmonary vasoconstriction, which according to emerging evidence may be a key mechanism driving severe covid and covid-related respiratory failure.
- Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) and reduces platelet serotonin concentration; cyproheptadine is a direct serotonin receptor antagonist.
Corticosteroids
Corticosteroids (e.g. prednisone, budesonide) reduce covid-related hyper-inflammation.
- A study by the University of Oxford, published in the Lancet, found a significant reduction in urgent care visits and hospitalizations in patients receiving budesonide (an asthma drug).
- The British PRINCIPLE trial found that budesonide accelerated recovery by 3 days and reduced hospitalizations and deaths from 10.3% to 8.5%.
- The early outpatient treatment protocol developed by McCullough et al. recommends the use of prednisone if (and only if) covid-related respiratory symptoms develop.
Monoclonal antibody therapy
Antibody therapy is intended to inhibit viral replication.
- Monoclonal antibodies are ineffective in late treatment of covid, but very effective in early treatment. This is because severe covid is characterized by hyper-inflammation, not viral replication.
- Some monoclonal antibodies have lost their effectiveness against new virus variants.
- Convalescent plasma therapy has been shown to be ineffective in both early and late treatment of covid.
Additional notes
The early treatment of patients as soon as the first typical symptoms appear and even without a PCR test is essential to prevent progression of the disease. In contrast, isolating infected high-risk patients at home and without early treatment until they develop serious respiratory problems, as often happened during lockdowns, may be counterproductive.
People at high risk living in an epidemically active area should consider prophylactic treatment together with their doctor. The reason for this is the long incubation period of covid-19 (up to 14 days): when patients first notice that they contracted the disease, the viral load is already at a maximum and there are often only a few days left to react with an early treatment intervention.
Early treatment based on the above protocol is intended to avoid hospitalization. If hospitalization nevertheless becomes necessary, experienced ICU doctors recommend avoiding invasive ventilation (intubation) whenever possible and using oxygen therapy (HFNC) instead.
See also

- Satellite imagery shows that logging activity is spreading from peripheral areas of the Amazon toward the rainforest’s core, according to groundbreaking research.
- The satellite-based mapping of seven of Brazil’s nine Amazonian states showed a “terrifying” pattern of logging advance that cleared an area three times the size of the city of São Paulo between August 2019 and July 2020 alone.
- At the state level, lack of transparency in logging data makes it impossible to calculate how much of the timber production is illegal, experts say.
- Evidence of cutting in Indigenous reserves and conservation units — where logging is prohibited — make clear that illegal logging accounts for much of the activity, according to the report.
One of the main fears about the Brazilian Amazon is beginning to materialize: logging is starting to move from the periphery of the rainforest toward the core of the biome, groundbreaking new research shows.
Tracking cut trees through satellite mapping data, the research found that logging activities cleared 464,000 hectares (1.15 million acres) of the Brazilian Amazon — an area three times the size of the city of São Paulo — between August 2019 and July 2020. More than half (50.8%) of the logging was reportedly concentrated in the state of Mato Grosso, followed by Amazonas (15.3%) and Rondônia (15%).
“Around 20 years ago, we feared that the forest would be devastated in the so-called ‘deforestation arch’ and the movement would migrate from the peripheral areas toward the central region of the Amazon,” said Marco Lentini, senior project coordinator of Imaflora, a sustainable development NGO involved in the mapping project. “Our map shows this is happening now: logging is going toward the Amazon core.”
He said the logging pattern was that of “frontier migration,” adding, “This is something that terrifies us. We have to stabilize this frontier.”

The largest seizure of illegal timber in Brazil’s history saw police recover 226,000 cubic meters (8 million cubic feet) of wood on the border between the states of Amazonas and Pará in March 2021. Image courtesy of the Federal Police in Amazonas state.
The research, released last week, was developed by the Simex network formed by four Brazilian environmental nonprofits: Imazon, Imaflora, Idesam, and Instituto Centro de Vida (ICV). The institutions say they set up the alliance to map, for the first time, logging in almost all of the Amazon. They managed to map seven of the nine states that make up the Brazilian Amazon — Acre, Amazonas, Amapá, Mato Grosso, Pará, Rondônia and Roraima — which together account for almost 100% of timber production from the rainforest.
Although the mapping was unable to specify the exact amount of trees illegally extracted from untouched forests, mostly of the illegalities were concentrated at the triple border between Mato Grosso, Amazonas and Rondônia, where intense logging activity was detected in an Indigenous reserve and a conservation unit, according to Vinicius Silgueiro, territorial intelligence coordinator at ICV, a nonprofit based in Mato Grosso. “Protected areas in this region show a large presence of logging and low level of fiscalization, with a lot of signs of illegality.”
The Sismex map covers areas where the Federal Police made the largest seizure of illegal timber in Brazil’s history earlier this year, recovering 226,000 cubic meters (8 million cubic feet) of wood on the border between Amazonas and Pará states. This operation triggered the ouster of the controversial minister of environment, Ricardo Salles, in June, after he reportedly asked for the release of the wood.
Ten municipalities accounted for almost 200,000 hectares (494,000 acres) of logging, five of them in Mato Grosso, two in Amazonas and the remaining in Roraima, Acre and Pará. Most logging activity, 78%, reportedly occurred on privately owned properties. Legal permits are often used to mask logging in restricted areas through a process known as tree laundering, according to the findings.
A more detailed study developed by Imazon focused on Pará shows that over half of the logging in the state has not received any governmental authorization. From August 2019 to July 2020, 50,139 hectares (123,896 acres) of forest were reportedly devastated, with 55% without authorization from environmental bodies. This represented a 20% growth over the 12 months before, when non-authorized logging totaled 38%, according to Imazon.

The map developed by the Simex network shows concentrations of logging activity in the state of Mato Grosso, followed by Amazonas and Pará. Image courtesy of Simex.Before the advent of the Simex project, only Pará and Mato Grosso had satellite-based maps identifying areas where logging has occurred. Imazon started monitoring Pará in 2008 and ICV joined the iniciative in 2013 by monitoring Mato Grosso. The institutions say that these states were their initial focus for data transparency due to high logging activities.
Logging for timber doesn’t clear forest area as extensively as deforestation does, and vegetation growth over logging sites can make visualization via satellite harder, according to Vinicius Silgueiro, territorial intelligence coordinator at ICV.
“With logging, different than deforestation, there is still some coverage by vegetation. We can identify scars in the forest made by the roads used to move the logs, as well as clear areas for storage. There is a whole infrastructure around logging that helps us find these areas,” Silgueiro told Mongabay in a phone interview.
In most states, however, he said it’s nearly impossible to verify when the logging activity is illegal, due to lack of transparency or technological barriers. Many times, he added, certificates for legal forestry activities are filed on paper, making it hard to cross-reference the database of certificates with the images. The only two states with digitized databases are Pará and Mato Grosso.

Logging activity in the Brazilian state of Rondônia, with trees already tagged and awaiting transportation. Image courtesy of Vicente Sampaio/Imaflora.
Another challenge is that the certificates allowing forest management give the location coordinates, but not the shape file — the digital map — of the area, which hampers efforts to identify through satellite imagery where illegal logging occurs, according to Lentini.
Despite these challenges, there are cases where it is very clear that the logging taking place is illegal, Lentini said: when it happens in protected areas like Indigenous reserves and conservation units. The study found that 6% of logging in the Amazon, or 28,112 hectares (69,466 acres), was in conservation units during the study period; 5% was in Indigenous reserves, at 24,866 hectares (61,445 acres). “These areas don’t have any kind of authorization for legal logging,” Silgueiro said.
A 2018 report by the Greenpeace, titled “Imaginary trees, real destruction,” highlighted the unreliability of Brazil’s forestry licensing and control systems, which it said makes it harder to tackle fraud.
“A critical flaw in the Amazon states’ forestry governance lies in the weakness of the licensing process for sustainable forest management plans,” the report said. For the most part, no field inspections are conducted before management plans are drawn up, or these inspections are of low quality, according to the report.
“This allows the forest engineers … to overestimate volumes or fraudulently add trees of high commercial value to the area’s forest inventory. State agencies subsequently issue credits for the harvesting and movement of this non-existent timber,” which will be logged from forests on Indigenous lands, protected areas or public lands, according to Greenpeace’s investigation.

Pará state environmental authorities seize illegal timber in an inspection operation in 2021. Image courtesy of Agência Pará.
Silgueiro, from ICV, said legal and illegal logging persist in proportions of around 60:40. “The more legal documentation there is for exploring the forest, the more illegal timber there is,” he said. He added that logging fraud will only stop once the whole process becomes traceable through technologies that help estimate the real volume of timber production and track each tree individually. “Traceability of production is essential,” Silgueiro said. “This technology already exists, but producing states are slow at adopting it.”
The environmental impact of illegal logging is immense. Recent studies show the Brazilian Amazon is now a net CO2 source, instead of being a carbon dioxide sink as would be expected, due to factors that include logging.
Banner image: A truck carries logs cut from the Amazon Rainforest in the state of Rondônia. Image courtesy of Vicente Sampaio/Imaflora.
An extension to a previous timeline covering April 2020–March 2021. The new timeline covers the period from April 2021 to June 2021.
Read the timeline by going to the source link.
The final discussion and conclusion is copied below.
Topics:
WHO's role and its funding, Gavi, COVAX, Trusted News Initiative, International Fact-Checking Network, the role of private philanthropy, Frontiers issue, comparison to the H1N1 pandemic, new treatment protocols, causal modeling.
Introduction
Ivermectin is a multifaceted medication invented in collaboration between Japanese professor emeritus Satoshi ¯ Omura from Kitasato University and US researcher William Campbell from Merck & Co/MSD between 1973 and 1979 [1];[2]. Each of them received one quarter of the 2015 Nobel Prize in physiology or medicine for their discoveries [3]. Ivermectin is best known as an antiparasitic agent, with approximately four billion doses having been administered since 1981, predominantly in Africa. Merck &Co/MSD’s patent expired in most countries in 1996, and ivermectin preparations are currently available internationally from many sources, with the production cost of a single dose estimated to be less than0.1 US dollars [4].
This article extends the timeline of ivermectin related-events described in a previous preprint available in two versions, March 30, 2021 and April 3, 2021 [5];[6]. The latter preprint covered the period from April 1, 2020 to March 31, 2021. This preprint extends the timeline to cover April–June 2021, as well as adding a few earlier events. Some caveats of the review are described in the previous preprint. Due to resource limitations, details of many developments are not covered in detail but only mentioned briefly,and omissions have been unavoidable. The focus of this review entails the social, organizational, financial and legal aspects of the situation with ivermectin, with less emphasis placed on presenting clinical trial results and biomedical research.Some of the main events in the previously covered period from April 2020 to March 2021 were an Australian in vitro study which initiated the interest in ivermectin [7]. This was followed by adoption of ivermectin in several South and Central American countries, the state of Uttar Pradesh in India, and Bangladesh in the second and third quarter of 2020. In late October 2020, the Front Line COVID-19Critical Care Alliance (FLCCC) published its ivermectin-based outpatient protocol called I-MASK+ [8];[9];[10].
A month later, another group called CovidAnalysis begun publishing a meta-analysis of ivermectin trials [11] and a list of ivermectin studies [12]. A main event in December 2020 was the US Senate hearing of Pierre Kory of the FLCCC [13]. The hearing raised interest of Lawrie et al. and Bryant et al. who produced additional meta-analyses [14];[15]. In conjunction, another group called British Ivermectin Recommendation Development (BIRD) was founded.
Another main event was the introduction of a preprint of a Unitaid/WHO-funded meta-analysis by Hillet al. [16]. Yet another notable event was the publication of an extensive review by a Japanese group including the discoverer of avermectins, the Nobel prize winner Satoshi ¯ Omura [2];[17].
In the first quarter of 2021, ivermectin had been adopted in several additional countries including Slovakia as the first European Union member country. However, in March 2021 both the European Medicine Agency (EMA) and the World Health Organization (WHO) advised against the use of ivermectin except in clinical trials, ignoring the various meta-analyses and the results of 26 existing randomized clinical trials, in addition to a similar amount of observational trials and other studies.
The majority of indications and the safety of ivermectin have been described in the previous preprint [6].In addition, in April 2021 ivermectin was found to effectively inhibit hepatitis E virus replication [18]. There is also a relatively large amount of research about the treatment of cancers with ivermectin [19][20][21][22][23][24][25], including breast cancer [26][27][28][29][30][31][32], ovarian cancer [33][34][35][36][37][38][39], cervical cancer [40], oesophageal squamous cell carcinoma [41], renal cancer [42], glioma [43][44][45], nasopharyngeal carcinoma [46], melanoma [47][48], gastric cancer [49][50], liver cancer [51] and leukemia [52][53] (list from [54]).
Recently, mass distribution of ivermectin has been studied for prophylaxis of malaria [55];[56];[57]. Ivermectin has also been found to promote wound healing partly through modulation of the inflammatory process and the levels of transforming growth factor beta 1 (TGF-β1) and vascular endothelial growth factor (VEGF) [58]. Ivermectin has also been proposed for the treatment of autoimmune disorders [59].
Omura has characterized ivermectin as “a panacea for resource-poor communities” [60]. Ivermectin has also been said to “continue to surprise and excite scientists, offering more and more promise to help improve global public health by treating a diverse range of diseases, with its unexpected potential as an antibacterial, antiviral and anti-cancer agent being particularly extraordinary” [61]. Possible issues include environmental toxicity [62];[63] and the emergence of ivermectin resistance [64].
April 2021...
Read the timeline by going to the source link. The final discussion and conclusion is copied below.
Discussion
In the United States and the European Union, most of the year 2020 appeared to have been characterized by an attempt to collect ivermectin-related data. The period from the beginning of November 2020 tothe end of March 2021 appeared to be characterized by disputes about interpretation of this data. The change of administration in the United States did not appear to significantly change its ivermectin-related health policy, likely to the disappointment of ivermectin proponents. Beginning from the March 30 guideline decision by the WHO against ivermectin, a period of a kind of trench warfare appeared to emerge. Ivermectin proponents, especially the FLCCC, announced they had resigned their attempts to influence the US National Institutes of Health, the Food and Drugs Agency, the European Medicines Agency and the World Health Organization. Similarly, the BIRD group turned directly to clinicians and the public. Changes to existing treatment protocols were mostly minor. Fluvoxamine emerged as an option and was added to many protocols including the FLCCC’s. The FLCCC introduced two new protocols: the I-MASS protocol for mass prophylaxis and the I-RECOVER for long haul COVID-19syndrome (LHCS). An interesting new development was the recognition of the role of mast cell activation and histamine release in LHCS [456].
The US NIH announced a new trial, ACTIV-6, for repurposed medicines, estimated to finish in March2023, almost two years in the future, rendering the trial practically irrelevant for the purposes of handling the pandemic. Simultaneously, pharmaceutical companies continued their attempts to finish their trials of new outpatient treatment pharmaceuticals as swiftly as possible, and new projects for the development of such treatments were initiated in the US and the UK.
A third concurrent process was the slower-than-expected progress of vaccination programs. A fourth concurrent process was the adoption of ivermectin in countries outside the US and EU. The countries who had adopted ivermectin previously, including Slovakia, implicitly disregarded the March 2021 guideline set by the WHO [171];[457]. India adopted ivermectin nationally after the announcement of the WHO guideline, then mostly dropped it, with the current situation being somewhat unclear. Legal action against the WHO was initiated in India. At the end of the period, Indonesia adopted ivermectin.With regard to researchers and clinicians, medical professionals whose practices appeared to be predominantly based on following existing regulations and protocols appeared to feel criticism against them unjustified and unfair. Similarly, medical professionals whose interest was in the further development of the protocols felt criticism against them unjustified and unfair. The first group may have perceived the latter group as deviants, whereas the latter group may have perceived the first group as anti-innovative.Presumably, both groups saw each others’ practices as somewhat unethical and antisocial. The difference was possibly due to different perspectives on collegiality and the perception of the role of patients. The first group appeared to put more weight on collegial cohesion and rule-adherence, with less weight put on individual patient outcomes, assumedly perceiving that patient outcomes were predominantly the product of the inflexible regulations which lay beyond their responsibility. The second group appeared to put less weight on collegial cohesion and regulations, placing more weight on individual patient outcomes, assumedly perceiving that patient outcomes superseded the rules and that validation of rules was the responsibility of individual clinicians.
With regard to COVID-19, knowledge about the mechanisms and treatments was somewhat scarce especially in the early phase of the pandemic. A recent study described that in such a situation, it would be adaptive to seek further information to resolve uncertainty and obtain a more accurate worldview but biases in such information-seeking behavior could contribute to the maintenance of inaccurate views [458].
The study indicated that more dogmatic individuals were less likely to seek out new information to refine an initial perceptual decision, leading to a reduction in overall belief accuracy despite similar initial decision performance. In addition, dogmatic participants placed less reliance on internal signals of uncertainty, rendering them less likely to seek additional information to update beliefs derived from weak or uncertain initial evidence. Dogmatism is often defined as a viewpoint or system of ideas based on insufficiently examined premises. Thus, differences in openness to research evidence may have been due to differences in personalities and habits which, in turn, may be seen as products of the life experiences(environments) of the individuals, including their medical education.
At times, the views appeared to differ up to a point in which the existence of a shared reality could be questioned, and the practice of presenting opposite conclusions on the same, existing data was in effect making further research irrelevant.
Validity of statistics-based research
In the context of clinical trials, the fundamental validity of the statistics-based research in general is rarely discussed. In 2011, Penston said that the extent and depth of the criticisms of statistics-based research usually comes as a surprise to investigators, doctors and other health care professionals who use the data from large-scale RCTs and epidemiological studies, as they rarely have the time, inclination and skill to read the related literature [459]. He questioned the large size of a study as a sign of strength,saying that as the number of patients recruited to a study increases, statistical significance may be achieved but causal inference is weakened, adding that the source of the problem was the belief that causal relationships of value can be derived from extremely heterogeneous samples. He also said that the methodology of statistics-based research cannot be tested independently of statistics; therefore it is unknown whether the causal inferences drawn from the data of large-scale RCTs and epidemiological studies are valid. According to him, lack of understanding of diseases and the properties of drugs, i.e.ignorance, were driving up the size of studies, and we had witnessed “an inexorable increase in the size of epidemiological studies and RCTs over the past 50 years without any concern for the consequences”.
Saint-Mont discussed the effect of randomization, detailing various false assumptions related to it, concluding that randomization does not lift experimental procedures in the medical and social sciences to the level of classical experiments in the natural sciences but may lull researchers into a false sense of security instead [460]. Both Saint-Mont and Penston stressed the importance of the existence of sound background theory as crucial for the success of science. Theory allows for stricter definitions of concepts and the identification of homogeneous reference classes that ensure regularity and, hence, reliable causal inference. In the context of COVID-19, the FLCCC appeared to present their conclusions more in the context of background theory (especially the MATH+ protocol [77]), while most others appeared to relymore on statistics.
An alternative or adjunct to RCTs to investigate could be causal modeling [461];[462];[463];[464]. According to Sgaier et al., causal modeling allows testing for causality in individuals and population groups faster and more efficiently, along with the ability to unravel the underlying complexity, and allows researchers and program designers to simulate an intervention and infer causality by relying on already available data [461]. Karvanen has provided examples of causal models for a case-control study,a nested case-control study, a clinical trial and a two-stage case-cohort study [463].
Journalistic ethics
With regard to journalistic ethics, the censorship discussion of April 11 appeared to indicate that journalistic principles that should have been self-evident no longer were, such as the responsibility of the media “to tell the truth” [165]. As described already for the period preceding April 2021, the financial press (e.g. the Wall Street Journal [163] and the Financial Express [171]) seemed to be more in favor of repurposed medicines, whereas the generalist press mostly continued to ignore or oppose them [217]. MacLeod has written about practices of the mass media in the United States, stating that corporate shareholders have no interest in the veracity of the news, only in short-term profits, and that reporting that challenges corporate profits is strongly discouraged [465]. A key factor shaping the content of the media is its reliance on advertising from large businesses for revenue. Advertisers wish to appeal to the groups and individuals with a greater spending power and to avoid controversial and critical content. Also, the collapse in advertising revenue in the traditional media has led to an increasing dependence on official sources, government and corporations which effectively subsidize the media by providing free content but expect something in return. In addition, in many cases, journalists are preselected based on their obedience to authority and their credulousness, and they increasingly come from the elite themselves [466]. The media houses also depend on social media for visibility which may be easily denied of them. Yet another factor are ideologies which in the United States were traditionally anti-communist but more recently anti-Trump and anti-Russian, for example. In the US media, ivermectin was often associated with hydroxychloroquine, and hydroxychloroquine with president Trump [467].
The dismissal of ivermectin in the press appeared to be related to the Trusted News Initiative (TNI) founded by Associated Press (AP), Agence France-Presse (AFP), British Broadcasting Corporation(BBC), Canadian Broadcasting Corporation (CBC), European Broadcast Union (EBU), Facebook, Financial Times, First Draft, Google, YouTube, The Hindu, Microsoft, Reuters, Twitter and Washington Post [321]. TNI appeared to function as some kind of peer-to-peer structured censorship mechanism.
Social media fact-checkers
In its COVID-19 medical misinformation policy, YouTube explicitly forbade treatment misinformation including “content that recommends use of ivermectin or hydroxychloroquine for the treatment of COVID-19” and “claims that ivermectin or hydroxychloroquine are effective treatments for COVID-19” [468]. The policy forbade also a large amount of peer-reviewed medical publications, in effect making YouTube an anti-science organization.
In a similar manner the policy forbade “prevention misinformation”, explicitly defined as “content that promotes prevention methods that contradict local health authorities or WHO”, specifically mentioning“content that recommends use of ivermectin or hydroxychloroquine for the prevention of COVID-19”. It also explicitly disallowed discussions of efficacy and possible adverse effects of vaccines which “contradict expert consensus from local health authorities or WHO”. Also diagnostic, transmission, social distancing and self-isolation information contradicting local health authorities or WHO were banned. The definitions of “expert” and “consensus” remained undefined, making the policy arbitrary, subsequently making YouTube an unpredictable promoter and enforcer of possibly arbitrary or authoritarian practices. In addition, technically, where local health authorities and WHO disagreed, application of the “or” operator banned content contradicting with either of them. Therefore in countries such as Slovakia and India,YouTube could not be used for content that recommended either for or against ivermectin for prophylaxis of COVID-19.
Clarke mentioned that YouTube and Facebook were relying on third party fact checkers funded partly by Charles Koch Institute [373];[374];[372]. Koch was listed as one of the 18 major funders of Poynter Institute, each with an undisclosed sum of at least USD 50,000, making it impossible to compare funders’ contributions [469];[470]. The International Fact-Checking Network (IFCN) is a unit of the Poynter Institute [471]. In May 2020, Facebook stated that all of its fact-checking partners were certified byIFCN [472]. IFCN stated it led an alliance of over 100 fact-checkers [473]. Poynter Institute described that the alliance was launched in January in response to “rampant misinformation globally” which the WHO classified as an “infodemic”, with the alliance “on the front lines in the fight against it”.
IFCN and the alliance also maintained a database of checked facts [474]. The database was updated daily, with members collaborating on the “massive crowdsourcing project” by using a shared spreadsheet and instant messaging apps. Poynter said the international collaboration had allowed the members to respond faster and reach larger audiences. All of the over 80 items found in the database with search term “ivermectin” dated between April 2020 and May 2021 were labeled either as no evidence, unproven, exaggerated, misleading, missing context, partly false, or false (the most common label), with two items labeled as explanatory [474]. Most of the items originated from South American partners such as Estadão Verifica in Brazil.
Some of the other major funders of Poynter included Facebook, Google News Initiative [475], Foundationto Promote Open Society (FPOS) of George Soros, a primarily US government funded agency National Endowment for Democracy (NED) [476], Democracy Fund created by eBay founder Pierre Omidyar, funding especially PolitiFact [477], and the Omidyar Network/Luminate also of Omidyar, Craig New-mark Foundation of Craigslist founder Craig Newmark, with at least USD 6 million donated to PoynterInstitute [478], and Rita Allen foundation involved in medical research, with its stated goal of “investing in transformative ideas in their earliest stages to promote breakthrough solutions to significant problems” [479].
It was of note that the major funders of Poynter included several individuals who were billionaires. Assumedly, they may have possessed influence over guidelines for what qualified as “facts”. While there was not enough information to ascertain whether the observed patterns of social media censorship were related to the values and previously observed practices of the any of the funders specifically, it was also not possible to rule out such influences.
An example may illustrate what kind of issues may arise from the use of donations as a tool for gaining political influence. With regard to funding by Koch, a report by Mayer in the New Yorker described the Koch brothers as “longtime libertarians who believe in drastically lower personal and corporate taxes,minimal social services for the needy, and much less oversight of industry .. . their combined fortune of thirty-five billion dollars is exceeded only by those of Bill Gates and Warren Buffett . . . many of the organizations funded by the Kochs employ specialists who write position papers that are subsequently quoted by politicians and pundits. David Koch has acknowledged that the family exerts tight ideological control. ‘If we’re going to give a lot of money, we’ll make darn sure they spend it in a way that goes along with our intent .. . and if they make a wrong turn and start doing things we don’t agree with, we withdraw funding’ ” [480];[481].
A republican political consultant commenting Kochs’ strategies for opposing climate change related oil industry reforms said that “the key .. . was to question the science – a public-relations strategy that the tobacco industry used effectively for years to forestall regulation”. As an example of health related interests, David Koch had served on the US National Cancer Advisory Board without disclosing his conflicts of interests as a major producer of formaldehyde, while simultaneously lobbying to prevent theUS Environmental Protection Agency (EPA) from classifying formaldehyde as a carcinogen, and funding members of Congress who had stymied the EPA, requiring it to defer new regulations until more studies would be completed.
Mayer’s article described Kochs’ operations as “covert”, referring to David Koch’s description of their businesses as “the largest company that you’ve never heard of”. According to Source Watch, in addition to denying climate change, other issues on the Kochs’ agenda included repealing health reform Obamacare), dismantling collective bargaining rights, fighting reductions in carbon emissions, keeping corporate money in elections and fighting internet neutrality [482];[483]. With regard to COVID-19, Koch Industries were producing test kit materials, sanitizers, alerting systems, healthcare IT systems related to COVID-19diagnostic testing, ventilators, and personal protective equipment [484].
Poynter’s largest custom training partners in 2019-2021 included Facebook, Huffington Post, Market-place, MRC Media, Middle East Broadcasting Networks, National Public Radio (NPR), Newsweek, New York Times, Southern Newspapers Publishers Association, Washington Post, TikTok, USA Today Network, Vice and Voice of America [469].
Academic journals
Regarding the academic journal publisher Frontiers Media SA’s, one of the members of its board of directors responsible for the financial and governance oversight of the company was Steve Koltes, founder and co-chairman of CVC Capital Partners Ltd [485]. In 2019, CVC Capital Partners, one of the world’s largest private equity and investment advisory firms, was said to have USD 75 billion of assets under management [486]. CVC announced that a group of its executives had helped fund University of Oxford’s vaccine research [487];[488]. CVC had also invested in System C, a company providing key software being used for planning and managing the UK’s COVID-19 vaccination programme [489]. The Times described CVC as “powerful, successful and extremely low profile” [490].
In 2015, Frontiers had removed 31 editors after the editors had complained that company staff were interfering with editorial decisions and violating core principles of medical publishing [491].
The WHO
During the period, an intensifying critique of the WHO emerged as a result of the March 2021 ivermectin guideline lacking transparency and breaking established practices of meta-analysis and research.Presenting criticism towards the feasibility of the vaccines-only approach and its possible relationship to financial interests of the pharmaceutical industry, or possible failures of entities such as WHO, FDA,NIH and EMA, has been difficult during the pandemic. Regardless, it is necessary to consider whether funding-related biases might exist with regard to the current practices of these agencies, especially the WHO.
First we may note that the main funders of the WHO for the 2018/2019 biennium were United States(USD 893 million), Bill and Melinda Gates Foundation (USD 531 million), United Kingdom (USD435 million), Gavi The Vaccine Alliance (USD 371 million), Germany (USD 292 million), Japan (USD214 million), UN Office for the Coordination of Humanitarian Affairs (UNOCHA) (USD 192 million),Rotary International (USD 143 million), World Bank (USD 133 million), European Commission (USD131 million), National Philanthropic Trust (USD 108 million), Canada (USD 101 million), China (USD86 million), Norway (USD 86 million), UN Central Emergency Response (USD 86 million), Sweden (USD77 million), France (USD 76 million), Kuwait (USD 70 million), Republic of Korea (USD 70 million) and Australia (USD 67 million) [492];[493];[494].
The Bill and Melinda Gates Foundation stated that its focus was on vaccine equity [307]. Also Gavi The Vaccine Alliance had been founded by the Bill and Melinda Gates Foundation in 1999, and the Gates foundation had invested a total of USD 4 billion in Gavi [495]. Gavi described the Gates foundation as“a key Gavi partner in vaccine market shaping”. The Gates Foundation also had long-term partnerships with Rotary International (polio vaccinations), National Philanthropic Trust, and the World Bank. Together, the USD 902 million contributions of the Gates Foundation and Gavi exceeded the United States contributions of USD 893 million, making the Gates-Gavi cluster the largest funder of the WHO in the2018/2019 biennium (in April 2020, president Trump announced that US halted funding to the WHO; the effects of this remained unclear [496];[497]). In addition, the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) contributed 33 million. Co-founded by the Bill and Melinda Gates Foundation in 2002, the foundation has contributed a total of USD 2.49 billion to GFATM [498]. Considering the recent USD 4 billion donation by the United States government to Gavi [89], one interpretation of the situation might be that the US outsourced a large part of its public health policy setting to Gavi and, subsequently, to Gates.
Yet another member of the Gates cluster was the Seattle-based PATH (Program for Appropriate Tech-nology in Health), one of the largest nonprofit organizations in global health [499]. In 2021, its website presented with a banner saying “600 million people are vaccinated. 7 billion haven’t had a shot. Help PATH today”. PATH’s CEO Nikolaj Gilbert, previously the global partnerships director for the United Nations Office for Project Services (UNOPS) and an employee of Novo Nordisk, described PATH’s priorities: “the partnership with the Bill and Melinda Gates Foundation and the U.S. government has shaped what this organization is all about today .. . so one of my key priorities will be to see: how can we sustain and grow those relationships that we have, how can we continue to be the preferred partner for those donors, and how can we also help them with their priorities?” [499].
A 2017 Politico article described Gates as “the world’s most powerful doctor”, saying his sway over the WHO spurred criticism about misplaced priorities and undue influence [500];[501]. The article quoted Gates’ critics saying that “Gates’ priorities have become the WHO’s . .. he is treated liked a head of state,not only at the WHO, but also at the G20”. Top WHO officials were said to have raised concerns that the foundation was distorting research priorities. Over three quarters of the WHO’s budget was coming from voluntary contributions which were usually earmarked for specific projects or diseases so that the WHO could not freely decide how to use them. The article stated that the Gates foundation’s focus on delivering vaccines and medicines, rather than on building resilient health systems, had drawn criticism.Changes had been made to the WHO’s budget approval process to in order to decrease the foundation’s influence. Yet a senior fellow for global health at the Council on Foreign Relations commented that “the foundation’s impact on the WHO is enormous . . . if they weren’t there, if they walked away with their money, the deleterious impact would be profound, and everyone is all too aware of that”.
Importantly, it should also be noted that the other top 20 funders predominantly represent high-income countries of the North America and Europe. None of the countries that had officially adopted ivermectin country-wide for COVID-19 up to April 2021 were represented [502]. Similarly, Coalition for Epidemic Preparedness Innovations (CEPI), an organization aiming to accelerate the development of vaccines against emerging infectious diseases and enable equitable access to these vaccines for people during outbreaks was founded by the governments of Norway and India, Bill and Melinda Gates Foundation, UK Wellcome Trust, and the World Economic Forum [503]. It had later secured financial support from Australia, Austria, Belgium, the Bill and Melinda Gates Foundation, Canada, Denmark, the European Commission, Ethiopia, Finland, Germany, Hungary, Iceland, Indonesia, Italy, Japan, Kuwait, Lithuania, Luxembourg, Malaysia, Mexico, Netherlands, New Zealand, Norway, Panama, Romania, Saudi Arabia,Serbia, Singapore, Switzerland, The Republic of Korea, United Kingdom, USAID, and UK Wellcome Trust. Of these countries, as of June 2021, ivermectin had been officially adopted in Mexico, Panama and Indonesia, as well as mixed use or occasional off-label use in some other countries [502].
Additionally, CEPI had received support from undeclared private sector entities as well as public contributions through the UN Foundation COVID-19 Solidarity Response Fund [503]. Each investor was to get one representative to an Investors Council providing guidance and oversight of CEPI activities, with four members serving on the CEPI board. Another entity, a Joint Coordination Group, was intended to discuss how to best enhance CEPI’s efforts to deliver and deploy vaccines, and had a role in planning for rapid response to a priority pathogen or an unknown pathogen. The Joint Coordination Group included the WHO, Gavi, European Medicine Agency (EMA), United States Food and Drug Administration Agency (FDA), Médecins Sans Frontières (MSF), UNICEF, International Federation of Red Cross and Red Crescent Societies (IFRC), African Vaccine Regulatory Forum (AVAREF), UK National Institute for Biological Standards and Control (NIBSC) and UK Wellcome Trust.
The Wellcome trust had been previously found out to secretly invest in companies that contributed to the same problems the trust said it wanted to solve [504]. The trust’s known investments through offshore companies in the Cayman Islands amounted to USD 891 million in 2018.
In 2010, the Bill and Melinda Gates Foundation, Gavi, WHO, US NIH/NIAID, CDC, UNICEF, PAHO and several research organizations launched a Decade of Vaccines collaboration, initiated by the Gates Foundation [505]. The intention was to enable greater coordination across all stakeholder groups – national governments, multilateral organizations, civil society, the private sector and philanthropic organizations. The five-member leadership council included the director general of WHO, Anthony S. Fauci of the National Institute of Allergy and Infectious Diseases (NIAID), executive director of UNICEF, an representative of African Leaders Malaria Alliance, and the president of global health at the Bill and Melinda Gates Foundation. All the relevant organizations had thus intimately and for the long term participated in the vaccine-centric collaboration initiated by Gates.
According to a recent study, in 2020, governments had spent a total of EUR 93 billion on COVID-19 vaccine and therapeutics development projects, with 95% allocated to vaccines and 5% on therapeutics [506]. 32% of the funds came from the US, 24% from the EU, and 13% from Japan and SouthKorea (a total of 69%). Only 7% of funds were preferred loans or conventional grants. 93% were advance market commitments (AMCs), i.e. binding agreements to subsidize purchases of vaccine doses prior to availability. Interestingly, 71% of the vaccine funding was allocated to Small and Medium Enterprises(SMEs) and MidCaps, with only 18% allocated to large pharmaceutical manufacturers. The figures did not include private sector investments.
The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public-private partnership program initiated by the US National Institutes of Health aimed at developing a coordinated research strategy for prioritizing and speeding development of the most promising treatments and vaccines [228]. Its public partners included Biomedical Advanced Research and Development Authority (BARPA), Centers for Disease Control and Prevention (CDC), Department of Defense, Department of Veterans Affairs,European Medicines Agency (EMA), National Institutes of Health (NIH), The Operation (formerly known as Operation Warp Speed), and US Food and Drug Administration (FDA). Industry partners included AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Dewpoint Therapeutics, Eisai, Eli Lillyand Company, Gilead, GlaxoSmithKline, Johnson & Johnson, Merck & Co/MSD, Moderna, Novartis,Novavax, Pfizer, Rhythm Therapeutics, Roche-Genentech, Sanofi, Takeda, and Vir Biotechnology. Nonprofit partners included Bill and Melinda Gates Foundation, Fred Hutchinson Cancer Research Center,Foundation for the National Institutes of Health, and RTI International.
According to the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA), as of February 2021, there were approximately 382 vaccine candidates in development, of which 24 in Phase I, 34 in Phase II and 23 in Phase III [507]. In addition to vaccines, there were over 1,000 clinical trials for therapeutics, of which 190 in Phase III. For example, Eli Lilly and Company and the Bill and Melinda Gates Foundation had entered into an agreement to facilitate access to future Lilly therapeutic antibodies under development, to benefit low- and middle-income countries.
Bill and Melinda Gates Foundation
According to Schwab, in five years up to 2020 the Gates Foundation had invested at least USD 250 million in companies that were currently working on COVID-19 vaccines, therapeutics, diagnostics or manufacturing [508];[509]. He also noted that Wellcome Trust had invested at least USD 1.25 billion to COVID-19 related industries [510]. Both funders were thus positioned to potentially gain from the pandemic financially. Wellcome’s director had a position on the Scientific Advisory Group for Emergencies advising the UK government on COVID-19, as well as a board seat on the Coalition for Epidemic Preparedness Innovations (CEPI). Earlier, the UK’s Scientific Advisory Group for Emergencies had failed to publicly disclose competing interests related to COVID-19. A Canadian professor emeritus of health policy and management commented that the funders were assumedly “acting the way they always have .. . looking after their own financial interests [and] pursuing their own privately developed objectives without being responsible to anybody but their own boards of directors”. Schwab said that despite the outsize role of the private charities in the pandemic response their financial interests had been little scrutinized, likely because foundations were not subject to the same oversight mechanisms as public institutions. A professor of sociology in the UK commented that the foundations were giving a false ideological impression that they are solving the problem even when they’re not.
The Gates foundation had also donated almost USD 2 billion to for-profit businesses, including USD 89 million to Novavax Inc., USD 65 million to GlaxoSmithKline Biologicals, USD 63 million to Evotec and Just Biotherapeutics, USD 61 million to Biologial E. Limited, USD 53 million to LG Chem Ltd., USD43 million to Dimagi Inc, USD 40 million to Inventprise, USD 38 million to Bharat Biotech International Ltd., USD 37 million to Janssen Vaccines and Prevention BV, and USD 35 million to AJ VaccinesAS [510]. Schwab claimed the foundation was subsidizing private companies’ research costs, opening up markets for their products, and bankrolling their bottom lines. He also claimed the foundation had funded groups pushing for industry-friendly government policies and regulation, including the Drug Information Association. He was also said to have funded nonprofit think tanks and advocacy groups that wanted to limit the role of government or direct its resources toward helping business interests. Schwab also noted that despite having given away USD 23.5 billion in the last five years up to 2020, Bill and Melinda Gates Foundation’s income from its investments had exceeded USD 28.5 billion in the same period [510].
Other commentators asked whether the Gates Foundation was addressing or reinforcing systemic problems raised by COVID-19, citing lack of transparency, dogmatic defence of intellectual property rights and monopolies, and intimate involvement with large pharmaceutical corporations as the main issues [511]. A 2016 report by Curtis gave details about Microsoft’s tax avoidance practices and its monopolistic nature, the foundation’s excessive global influence and support to various questionable practices including industrial agriculture with patented genetically modified seeds, Gates family’s “considerable personal access to senior levels of the WHO”, Gavi’s alleged overpaying for vaccines leading to excessive increases in vaccine prices, Gates’ dismissal of the issue, and the foundation’s agenda skewing health priorities and distorting health programmes [512]. Curtis wrote that one problem with the foundation’s heavy focus on developing new vaccines was that it detracted from other, more vital health priorities such as building resilient public health systems. As a rationale, Gates was said to have provided the following: “Vaccines are an extremely elegant technology. They are inexpensive, they are easy to deliver, and they are proven to protect children from disease. At Microsoft, we dreamed about technologies that were so powerful and yet so simple.. . all 193 member states, you must make vaccines a central focus of your health systems”. Curtis commented that Gates had “a fixation on vaccines”. He also claimed the foundation was stifling criticism through its media and NGO influence built on donations. An US professor of media, culture and communications was quoted saying the foundation “wielded enormous propaganda power”. A 2009 editorial in the Lancet, describing the foundation’s governance principle of being “driven by the interests and passions of the Gates family” as “whimsical”, proposed that the foundation should be more transparent and accountable and listen to opinions of external parties [513];[514].
In April 2020, the Bill and Melinda Gates Foundation awarded a five-year grant of USD 50 million to Unitaid to fight against HIV, tuberculosis and malaria, in addition to previous contributions of USD 100 million since 2006. Unitaid’s budget for the year 2021 was approximately USD 32 million [515]. In late 2020, Unitaid partially funded the ivermectin meta-analysis by Hill et al. published as a preprint [16].This meta-analysis was later ignored by the WHO in its March 2021 decision against the use of ivermectin except in clinical trials [6]. On April 22, the chief of Unitaid stressed the need to increase commercialresearch and development of new pharmaceuticals for the treatment of COVID-19 [242]. A core function of Unitaid is Medicines Patent Pool, a tool or practice to negotiate patents for low-income countries; this emphasis may have made unpatentable products seem foreign to the organization [516];[517]. Gates foundation was the chair of Unitaid’s Finance and accountability committee and a member of its policy and strategy committee [518].
Comparing the countries most heavily involved in the development and funding of vaccines to the countries with interest in ivermectin it can be noted that the two sets of countries have little overlap. Also, it can be noted that if influence is related to the amount of funding given, the first set of countries likely had more influence in the WHO in comparison to the rest of the countries.
The WHO, the philanthropic entity Bill and Melinda Gates Foundation, the public-private partnership Gavi, The Vaccine Alliance, and the philanthropic-commercial entity CEPI appeared to be strongly interconnected with each other and with high-income nation states. Major financial investments and commitments likely created propensities for various biases and a vulnerability to the sunk cost fallacy [519]. A haphazard or ideological commitment solely to vaccines (95% of government spending) may have overlooked considerations of cost-effectiveness and feasibility, such as vaccines likely being more expensive and more vulnerable to viral variants than repurposed medicines, their long-term safety being unclear, and vaccines likely requiring constant redevelopment and revaccinations, in addition to not being suitable for self-administration and requiring refrigerated delivery systems. With regard to the sunk cost fallacy, it would be more economical for the governments to reconsider the vaccine and investigative pharmaceuticals dominated pandemic policy and at least adjunct it with broad-spectrum repurposed medicines.
Comparisons to the H1N1 pandemic
After the H1N1 ‘swine flu’ pandemic of 2009-2010, the WHO was accused of malpractice when conflicts of interests of key WHO scientists led to unfeasible WHO recommendations which in turn led to billions of public money spent on inefficacious antivirals for H1N1 influenza [520];[521];[522];[523]. In her book, Abeysinghe has written about the role of the WHO [524]. A review by Andres summarizes keypoints, including the monopoly of the WHO to declare a pandemic [525]. In the case of H1N1, WHO was retrospectively criticized for unnecessarily declaring a pandemic, as for example the European Centre for Disease Control (ECDC) did not agree that the disease should be qualified as severe (measured by mortality), which at the time was considered a requirement for a pandemic but is no longer mentioned. At the time, an epidemiologist commented that the WHO, public health officials, virologists and pharmaceutical companies had “built this machine around the impending pandemic . . . there’s a lot of money involved, and influence, and careers, and entire institutions .. . all it took was one of these influenza viruses to mutate to start the machine grinding” [526].
WHO was later criticized by the Council of Europe for giving too much importance to vaccination and for not sufficiently emphasizing other measures such as the use of antivirals even though some arguments suggested that other measures, such as taking antivirals preventively, could be at least as efficacious as vaccines [525];[521];[522]. WHO emphasized mass vaccination as the most effective strategy against H1N1 [524]. According to Abeysinghe, this emphasis was a result of the path-dependent institutional reaction of the organization, where prior experience with infectious disease (including notable victories using mass vaccination strategies) resulted in the favoring of this reaction, whereas other potential actions were disregarded or underemphasized.
In June 2010, the rapporteur of Council of Europe Parliamentary Assembly described the acts of the WHO as foolish, saying “this is not going to go away” [524]. The rapporteur assumedly meant the criticism was not going to go away; yet it appears instead that the organizational patterns did not go away, leading the WHO and the national governments to repeat the same issues a decade later in theCOVID-19 pandemic.
Legal responsibility of public-private partnerships and the WHO
Clarke has noted that the regulation of global health has partially shifted from the hands of states and international organizations into the hands of public-private partnerships such as Gavi, The Vaccine Alliance and the Global Fund [527];[528]. These partnerships then become capable of also adversely impacting the rights of individuals, leading to concerns of responsibility under international law. However, the private entities in public-private partnerships typically fall outside the framework of responsibility under international law, and thus cannot be held responsible under it. In addition, in certain instances the partnerships have been granted immunity from the jurisdiction of domestic courts. This immunity applies to the staff, funds, properties and assets of these partnerships. The situation regarding Gavi andthe Global Fund appeared especially complicated and the legal details were therefore considered out of the scope of this review.
With regard to the WHO, Gostin has described WHO’s regulatory powers as extraordinary, noting that it may set regulations on a broad range of health topics including the safety, potency, and advertising of biologicals and pharmaceuticals, and a nomenclature for diseases, causes of death, and public health practices [529];[530]. These regulations, unlike most international law, are binding on member states unless they proactively “opt out”. In addition, also the WHO enjoys several privileges and legal immunities. Regardless of the original purpose of these privileges, the possibility of abuse of these privileges by the WHO also exists. Also here the details were considered out of the scope of this review.
Private philanthropy, society and science
In his recent book, Callahan discussed the role of private philanthropy, noting the rising influence and political significance of elite philanthropy, asking who is making choices over public life and who actually benefits from those choices [531]. Callahan described “today’s era of austerity” as a result of an orchestration of the upper class to reduce its taxes and the size of government, even so that in some US states, cuts to higher education specifically helped finance tax reductions for the wealthy and corporations. He noted that in a decade, Bill Gates and Warren Buffett, the main funders of the Bill and Melinda Gates Foundation, had added USD 25 billion and USD 80 billion, respectively, to their wealth, and that the Koch brothers had increased their wealth from USD 9 billion in 2005 to USD 85 billion in 2015.In a book review, Saunders-Hastings asked whether elite philanthropists are a counterweight to other, self-interested elites or to democracy itself, and noted that the distance between elite “charity” and elite political influence is small and shrinking, and that donors’ motivations matter less than the results of their actions [532].
Broad wrote that due to cuts to public funding and increase in private donations, “American science, long a source of national power and pride, is increasingly becoming a private enterprise” and quoted a policy analyst commenting that “the practice of science in the 21st century is becoming shaped less by national priorities or by peer-review groups and more by the particular preferences of individuals with huge amounts of money” [533].
Callahan proposed putting some curbs in place against the private philanthropy, yet noted that foundations and nonprofit trade groups are strongly against any new restrictions, partly due to their dependency on philanthropy. He noted that “rethinking philanthropic freedom is a Pandora’s box that almost nobody wants to open”, saying the current situation was a result of “yesterday’s mantras about philanthropic freedom and the dated regulation upholding it”.
Vaccines vs repurposed medicines
In Finland, a team led by two leading Finnish professors, Kari Alitalo and Seppo Ylä-Herttuala, had a patent and intellectual property free adenovirus-based nasal spray COVID-19 vaccine ready in May 2020. Despite taking approximately EUR 18 billion of public debt to mitigate damages caused by societal lockdowns and using hundreds of millions of Euros on diagnostic tests only, the Finnish government refused the approximately EUR 50 million needed to fund a phase III patient trial for the vaccine [534];[535].
The above case illustrates that the issue at hand is fundamentally not even about vaccines versus repurposed medicines or new pharmaceuticals versus repurposed medicines. Based on this data it is difficult to say whether it is about excessive adherence to inflexible regulations, subconscious biases present in corporate cultures and individuals, intellectual property enforcement, or intentional misleading for profit; likely, it is a mixture of all these factors. Personal biases, organizational cultures and commercial incentives of the vaccine cluster may have lead to attempts to build near-monopolies mass-producing proprietary but inferior products that outcompete more feasible alternatives. In Finland, significantly less interest has been present for any repurposed medicine than for the patent-free vaccine, with the sole exception of the company which developed the ivermectin-containing nasal spray not yet on the market [356].
More generally, the situation may partly be a result of the unprepared and rushed way in which the pandemic has been handled by the governments. Assumedly, from the perspective of governments with 95% of their funding committed to vaccines and international co-operation led by the WHO, paradigm change inducing innovations from outsiders may be perceived as unwanted disturbances. Considering these paradigms, the dismissal of ivermectin might be perceived as cultural discrimination, an instinctive reaction to avoid unfamiliar ideas. As a result of the chosen policy of vaccines and new pharmaceuticals only, in order to avoid losing the sunk costs and credibility, the interests of the governments and the pharmaceutical industry appeared to align with each other but likely not with the public health interest.
The concept of “regulatory capture” may be described as the agencies tasked with protecting the public interest coming to identify with the regulated industry and protecting its interests against those of the public, with the result of government failing to protect the public [536]. Whether rejection of ivermectin may be seen as an example of “regulatory capture” depends on how the vaccines-only policy was selected: primarily to align with the interests of the pharmaceutical industry, or because a better option could not be imagined. Curiously, options could be imagined early on in many low-income countries, but not in the high-income countries, possibly as a result of “technological capture”: when access to advanced technology exists, every problem looks like a problem to be solved with advanced technology, even though such solutions would be suboptimal due to being overly complex and unnecessarily expensive. For example, the idea of spending tens of billions of dollars per year for testing 20 percent of the global population every week assumedly for a single pathogen (SARS-CoV-2) appeared irrational at best [89]. Gates’s speeches repeated terms such as “war and “battle plan” [537]; these talks may easily be interpreted as priming fear in the public. Gates is also famous for regularly predicting the next pandemics [538].
Since the beginning of 2021 at the latest it should have been obvious that the continuing denial of early treatments could not be characterized either as accidental or as a rational choice with respect to public health interest. During the pandemic, a large part of the medical community seemed incapacitated like an old-fashioned military unit lacking leadership. The model based on the fear of losing medical license and an inflexible hierarchical chain of command appeared unsuitable for ensuring proper care of populations.While denial of treatments for certain illnesses such as drug addictions, post-traumatic stress disorder or “treatment-resistant” depression for years or decades for example by denying funding for the research of psychedelic therapies has become normalized, it was unexpected that in the case of COVID-19 this antisocial behavior on behalf of governments and the pharmaceutical industry would be extended to literally everyone in the world. In a comment suggesting adoption of ivermectin, a patent attorney and a former director of a pharmaceutical company referred to “potential civil/criminal liability for censorship, scientific misconduct for misrepresenting ivermectin and other generics” [387].
The exact causes of the situation remained unclear. Regardless, the consequences remain to be seenand felt. One way forward might entail the majority of governments halting their funding to the WHOin order to dissolve the whole organization which appeared beyond repair. Another necessary changemight be the eviction of the so-called philanthropic entities from healthcare contexts. In the long term,another beneficial action might be a worldwide conversion of the pharmaceutical industry into a nonprofit operation. Continuing on the current path may result in a further polarization or destabilization of societies.
Near-future objections to adoption of ivermectin will undoubtedly include the possible environmental impacts. In the mid-to-long term, due to the need to reduce water usage and enable better retention of nitrogen, phosphorus and ammonia [539], transition from water based sewer systems to toilet systems not using water and not requiring wastewater processing but utilizing for example composting and new kind of treatments to degrade pharmaceuticals will become inevitable in many areas in any case.
Conclusions
During this period, ivermectin was officially adopted in South Africa but not widely used, adopted but later dropped in most of India, and adopted in Indonesia. In the United States and the United Kingdom, projects with involvement of both the governments and commercial companies were announced for development of new pharmaceuticals for early outpatient treatment of COVID-19, indicating unclear boundaries between these entities. The dismissal of repurposed medicines including ivermectin continued in high-income countries due to very differing views on what constituted evidence of efficacy. The divide between ivermectin proponents and opposers remained mostly unchanged during the period, indicating a stagnated situation.
There was a noticeable centralization of power, with pandemic response and public discussions largely directed by a few organizations that were largely funded by a few billionaires which, in turn, were affectedby their own personal preferences and biases such as obsessive-compulsive attachment to testing and new technologies, primarily vaccines. Legal responsibilities of these organizations appeared, in the words of one researcher, “obscure”.
Commercial interests appeared to override public health interests during this period. As a result, several low-and-middle-income countries and regions either implicitly or explicitly disregarded the WHO guidance, accelerating an erosion of WHO’s credibility.

(Traduction en français disponible ici)
Following their “Open Letter to the Unvaccinated”, an expanding group of Canadian scholars has now written a letter addressing “the vaccinated”. The writers expose the divisiveness of vaccination status and denounce the resulting rift in society.
Giving up civil liberties in exchange for a false sense of safety is futile. We must not accept a descent into medical apartheid in Canada and around the world.
The letter appeals both to those who chose to take the vaccine and those who were coerced. It reflects on the broader implications of our actions in an effort to collaborate on a constructive path forward.
Open Letter to the Vaccinated
Prime Minister Trudeau recently warned that “there will be consequences” if federal employees do not comply with vaccine mandates. This is a voice of tyranny that has reverberated fear and heightened agitation across our country. It has launched our nation into deep division around mass vaccination and brought our collective recovery from this pandemic to a critical head. In fact, it forces us, as a country, to finally ask: indeed, what are those consequences?
What are the societal consequences of being divided along the lines of vaccination status? What are the consequences of mandating such an insufficiently tested medical intervention? How is this all supposed to end well?
The consequences will be dire, to be certain. And the consequences will affect all of us, the vaccinated and the unvaccinated alike.
Over the last six months, many of us made our decision to accept the vaccine in good faith – doing the right thing in order to work, travel and visit the people we love. Sadly, some of us have been pressured or coerced. And now, mounting evidence worldwide shows that these vaccines cannot stop the transmission of the virus and variants, yet vaccination mandates continue.
Meanwhile, the pharma corporations are earning billions of dollars of public money, and pushing to fast-track the vaccines towards full approval, without due process or public discussion. It is abundantly clear that when money and politics intertwine, science and ethics take a back seat.
Maybe you once resented those who hesitated to get the vaccine, as people who were not doing their part; but maybe it is time to consider that we have all become passengers on the same runaway train. The meaning of “fully vaccinated” is rapidly changing as leaders demand the next booster upgrade and threaten ousting us from public spaces if we don’t comply. So, if you are among the “fully vaccinated” today, by tomorrow you may become one of the “insufficiently vaccinated” and be coerced into taking another shot.
If history is any indication, this will not stop with barring admission to concerts or bars. When you can no longer buy food, access banking, vote in person or cross a provincial border, it will be crystal clear that the same discriminatory practices that you hope to abolish will be ever more firmly established. The real consequences await all of us.
Perhaps you’ve had your full round of doses and are now having doubts about whether to continue based on the alarming number of infections among the vaccinated. Or maybe you know someone who has been vaccine-injured or are concerned about the mounting death reports in conjunction with vaccinations.
We keep asking ourselves, “Why is the data not allowed to be scrutinized and why are independent experts being censored if they attempt to do just that?” It is incomprehensible, and decidedly un-Canadian, to see the silencing of highly regarded doctors and health scientists in our country and around the globe.
History has taught us that one-sided arguments and outlawed dissent are signs of totalitarianism lurking at the doorstep. Soon, asking questions will make you an enemy of the State. Mandating vaccines is a breaking point. “My body, my choice” has been one of the hallmarks of a free and democratic society, but this is changing. Canadians are being robbed of personal decision making.
With lockdowns already scheduled for the fall, and boosters at the ready, we are entering a watershed moment. Are we all willing to continue being injected indefinitely? In Canadian provinces and around the world vaccine passports are demonstrating our new, long-term relationship with medical coercion in exchange for basic freedoms. Thus far, each treatment has been promised to be the last, but it couldn’t be clearer that there is no end in sight.
And now they’re coming for our children.
With extremely low risk of becoming ill and practically no risk of dying from COVID-19, the mass vaccination of children and adolescents remains unwarranted. Lining up our healthy children for medical treatment was never part of the deal. Most disturbingly of all, we are being primed for mass vaccination campaigns in our schools that do not require parental consent. Does the government decide what is best for our children? Without question, the family ties that bind us are being undone. Justifiably, parents are appalled by this unprecedented overreach and are debating pulling their children out of schools.
Despite our best intentions, families are scarred, friends are divided, and partners are at odds with each other. We have been weakened by our division and manipulated through fear.
Just how far will we allow this to go? “All the way!” some of us declare. But “all the way” is a place we will never reach. We need to stop this medical catastrophe and face the truth: this isn’t about our health; it is about politics and it is about control.
The consequences of following Prime Minister Trudeau’s current orders are greater than his threatened consequences. We entered into this for one another, not for our politicians. We have done what we felt we had to do, and now we must say, ‘This is far enough, no more!’
Angela Durante, PhD
Denis Rancourt, PhD
Jan Vrbik, PhD
Laurent Leduc, PhD
Valentina Capurri, PhD
Amanda Euringer, Journalist
Claus Rinner, PhD
Maximilian C. Forte, PhD
Julie Ponesse, PhD
Michael Owen, PhD
Donald G. Welsh, PhD

“I’m not going to arm wrestle with the administration about where to put you,” Dr. C., a highly skilled gastroenterologist, said gently to my friend who was in bed in a triage room in the ER. “We just want to get you into a bed so we can figure out what’s wrong and get you treated.”
We were at our small town’s hospital. No one was sure why, but my friend had not been able to keep anything more than a handful of raspberries down since a complicated surgery for a chronic health condition three weeks before. Dehydrated and unable to eat, my friend had been violently vomiting after taking just a sip of water or sucking on an ice chip, and had lost nearly twenty-five pounds.
I was by my husband’s side when he had a gallbladder attack so severe that it left his hands shaking. I’ve had three unmedicated childbirths and attended many more, both as a journalist and a patient advocate. Still, I’ve never seen a human in so much pain.
Diagnosed with a Pancreas Disorder, Admitted as a COVID Patient
After a battery of testing, my friend was diagnosed with pancreatitis. But it was easier for the hospital bureaucracy to register the admission as a COVID case.
Let me explain. This patient had none of the classic symptoms of COVID: No shortness of breath, no fever, no chills, no congestion, no loss of sense of smell or taste, no neurological issues. The only COVID symptoms my friend had were nausea and fatigue, which could also be explained by the surgery. However, nearly three weeks earlier, a COVID test had come back positive.
The mainstream media is reporting that severe COVID cases are mainly among unvaccinated people. An Associated Press headline from June 29 reads: “Nearly all COVID deaths in US are now among unvaccinated.” Another, from the same date: “Vast majority of ICU patients with COVID-19 are unvaccinated, ABC News survey finds.”
Is that what’s really going on? It’s certainly not the case in Israel, the first country to fully vaccinate a majority of its citizens against the virus. Now it has one of the highest daily infection rates and the majority of people catching the virus (77 percent to 83 percent, depending on age) are already vaccinated, according to data collected by the Israeli government.
After carefully reviewing the available data, including the safety and efficacy profiles of the mRNA vaccines, my friend had taken a cautious approach. Though a medical doctor who gives vaccines in the office every day, my friend opted to wait and see. According to WebMD, a “huge number” of frontline hospital workers have also chosen not to get the vaccine. Indeed, various news reports, from California to New York, confirm that up to 40 percent of health care workers have decided the risks of the vaccines do not outweigh the benefits.
After admission, I spoke to the nurse on the COVID ward. She was suited up in a plastic yellow disposable gown, teal gloves, and two masks underneath a recirculating personal respiratory system that buzzed so loudly she could barely hear. The nurse told me that she had gotten both vaccines but she was feeling worried: “Two thirds of my patients are fully vaccinated,” she said.
[
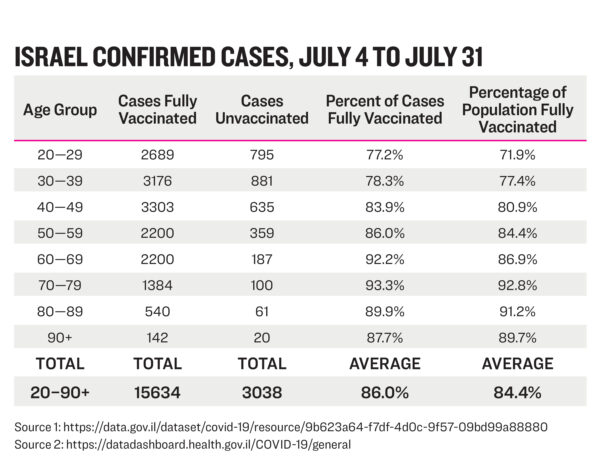
](https://img.theepochtimes.com/assets/uploads/2021/08/01/Israel-confirmed-cases-table.jpg)
Data Limitations
How can there be such a disconnect between what the COVID ward nurse told me and the mainstream media reports? For one thing, it is very hard to get any kind of accuracy when it comes to actual numbers. In fact, the Centers for Disease Control and Prevention (CDC) have publicly acknowledged that they do not have accurate data.
As reported by the Associated Press, “The CDC itself has not estimated what percentage of hospitalizations and deaths are in fully vaccinated people, citing limitations in the data.”
At the same time, data collection is done on a state by state basis. In most states, a person is only considered fully vaccinated fourteen days after they have had the full series of the vaccine.
This means that anyone coming into an American hospital who has only had one dose, or who has had both vaccines but had the second one less than two weeks prior, will likely be counted as “unvaccinated.”
So when the South Carolina’s Department of Health and Environmental Control released a report about COVID severity on July 23, 2021, they reported higher morbidity and mortality rates in the “not fully vaccinated.” Are these people who have had one vaccine and gotten sick, two vaccines and gotten sick, or no vaccines at all? Without more details, it is impossible to know what is really going on.
“We don’t have accurate numbers,” insists Dr. James Neuenschwander, an expert on vaccine safety based in Ann Arbor, Michigan.
But what we do know, Neuenschwander says, is that the vaccines are not as effective as public health officials told us they would be. “This is a product that’s not doing what it’s supposed to do. It’s supposed to stop transmission of this virus and it’s not doing that.”
Overcounting COVID
Then there is the problem of attributing severe illness and deaths from other causes to COVID, like in my friend’s case. Health authorities around the world have been doing this since the beginning of the COVID crisis. For example, a young man in Orange County, Florida who died in a motorcycle crash last summer was originally considered a COVID death by state health officials (after Fox News investigation the classification was changed.) And a middle-aged construction worker fell off a ladder in Croatia and was also counted as a death from COVID (whether having COVID played a role in his death is still unclear.)
To muddy the waters further, even people who test negative for COVID are sometimes counted as COVID deaths.
Consider the case of 26-year-old Matthew Irvin, a father of three from Yamhill County, Oregon. As reported by KGW8 News, Irvin went to the ER with stomach pain, nausea, and diarrhea on July 5, 2020. But instead of admitting him to the hospital, the doctors sent him home.
Five days later, on July 10, 2020, Irvin died. Though his COVID test came back negative two days after his death and his family told reporters and public health officials that no one Irvin had been around had any COVID symptoms, the medical examiner allegedly told the family that an autopsy was not necessary, listing his death as a coronavirus case. It took the Oregon Health Authority two and a half months to correct the mistake.
In an even more striking example of overcounting COVID deaths, a nursing home in New Jersey that only has 90 beds was wrongly reported as having 753 deaths from COVID. According to a spokesman, they had fewer than twenty deaths. In other words, the number of deaths was over-reported by 3,700 percent.
Who’s Suffering from Severe COVID, Vaccinated or Unvaccinated?
In countries with the highest numbers of vaccinated individuals, we are also seeing high numbers of infections. Iceland has one of the most vaccinated populations in the world (over 82 percent) and is reporting that 77 percent of new COVID cases are in fully vaccinated Icelanders, according to Ásthildur Knútsdóttir, Director General of the Ministry of Health.
According to news reports, over 85 percent of the Israeli adult population has been vaccinated. But a July report from Israel’s Ministry of Health found that Pfizer’s vaccine is only 39 percent effective. Though Israeli health officials are telling the public that the cases are more mild in vaccinated individuals, this upsurge in COVID cases and deaths is leading Israel’s prime minister to issue new restrictions.
Dr. Peter McCullough, an academic internist and cardiologist in practice in Dallas, Texas, says that a large number of people in the hospitals right now have, indeed, been fully vaccinated. “Fully vaccinated people are being hospitalized, and … 19 percent of them have died,” McCullough says. “This is not a crisis of the unvaccinated. That’s just a talking point. The vaccinated are participating in this.”
Other physicians are seeing the same thing. “In my practice multiple patients who are fully vaccinated have been admitted to local hospitals,” says Dr. Jeffrey I. Barke, a board-certified primary care physician based in Newport Beach, California. Barke believes part of the problem is exaggeration of the efficacy: “If the vaccine works so well, why are we now pushing a booster?”

Jennifer Margulis
Jennifer Margulis, Ph.D., is an award-winning journalist and author of Your Baby, Your Way: Taking Charge of Your Pregnancy, Childbirth, and Parenting Decisions for a Happier, Healthier Family. A Fulbright awardee and mother of four, she has worked on a child survival campaign in West Africa, advocated for an end to child slavery in Pakistan on prime-time TV in France, and taught post-colonial literature to non-traditional students in inner-city Atlanta. Learn more about her at JenniferMargulis.net
Secretary Antony Blinken @SecBlinken - 1:34 UTC · Aug 31, 2021
I want to drive home today that America’s work in Afghanistan continues. We have a plan for what’s next, and we’re putting it into action.
The codename for the plan which Secretary Blinken is putting into action has not been officially released. It will likely be called "Eternal Revenge" or something similar.
The U.S. is not a good loser. Nor are President Biden and Blinken. They will take revenge for the public outcry their chaotic evacuation of troops and civilians from Afghanistan has caused. The Taliban will be blamed for it even as they, following U.S. requests, had escorted groups of U.S. citizens to the gates of Kabul's airport.
One can anticipate what their plan entails by looking at the process that led to yesterdays UN Security Council resolution about Afghanistan. The full resolution has not been published yet but the UN reporting on it gives the gist:
Security Council urges Taliban to provide safe passage out of Afghanistan
Thirteen of the 15 ambassadors voted in favour of the resolution, which further demands that Afghanistan not be used as a shelter for terrorism.
Permanent members China and Russia abstained.
As the resolution only 'urges' it is obviously minimal and not binding. It is not what the U.S. had set out to achieve. It wanted a much stronger one with possible penalties (see 'holding ... accountable' below) should the Taliban not follow it.
Prior to the UNSC meeting France and Great Britain had proposed to create a 'safe zone' in Kabul. That request has been silently dropped - likely over Chinese and Russian concerns about Afghanistan's sovereignty.
On August 29 Blinken had talked with China's Foreign Minister Wang Yi about a binding resolution. The State Department readout of the call was minimal:
Secretary of State Antony J. Blinken spoke today with PRC State Councilor and Foreign Minister Wang Yi about the importance of the international community holding the Taliban accountable for the public commitments they have made regarding the safe passage and freedom to travel for Afghans and foreign nationals.
The readout by China reveals that much more than that was discussed:
Wang said that the situation in Afghanistan has undergone fundamental changes, and it is necessary for all parties to make contact with the Taliban and guide it actively.
The United States, in particular, needs to work with the international community to provide Afghanistan with urgently-needed economic, livelihood and humanitarian assistance, help the new Afghan political structure maintain normal operation of government institutions, maintain social security and stability, curb currency depreciation and inflation, and embark on the journey of peaceful reconstruction at an early date, he said.
The U.S. has blocked Afghanistan's Central Bank reserves, has stopped any budgeted payments to Afghanistan and ordered the International Monetary Fund and the World Bank to block their Afghanistan programs.
This will paralyze all functions of the Afghan state. The World Bank is for example currently responsible for paying Afghan teachers and medical personnel. Afghanistan is experiencing a drought and will need to import large amounts of food. With its foreign assets blocked it has no way to do that.
China is clearly aware that Afghanistan will experience a human catastrophe should the U.S. continue its economic blockade.
There is also the danger of terrorism which the U.S. failed to address:
Wang urged the United States, on the premise of respecting Afghanistan's sovereignty and independence, to take concrete actions to help Afghanistan combat terrorism and violence, instead of practicing double standards or fighting terrorism selectively.
The U.S. side clearly knows the causes of the current chaotic situation in Afghanistan, Wang noted, adding that any action to be taken by the UNSC should contribute to easing tensions instead of intensifying them, and contribute to a smooth transition of the situation in Afghanistan rather than a return to turmoil.
China is specifically concerned about the "East Turkestan Islamic Movement" (ETIM) in east Afghanistan which the Trump administration had last year taken off its terrorist list even though the organization continues to target China. The Biden administration has made no attempt to revive the terrorist designation of ETIM.
Russia has similar concerns as its Permanent Representative Vassily Nebenzia explained after abstaining from the resolution:
We had to do this because the authors of the draft had ignored our principled concerns.
Firstly, despite the fact that the draft resolution was proposed against the backdrop of a heinous terrorist attack, the sponsors refused to mention ISIL and “Eastern Turkistan Islamic Movement” – the organizations that are internationally recognized as terrorist – in the paragraph on counter-terrorism. We interpret it as unwillingness to recognize the obvious and an inclination to divide terrorists into “ours” and “theirs”. Attempts to "downplay” threats emanating from these groups are unacceptable.
Secondly, during the negotiations we emphasized the unacceptability and negative impacts of evacuation of Afghan highly qualified personnel for Afghanistan’s socio-economic situation. If experiencing a “brain drain”, the country will not be able to achieve Sustainable Development Goals. These elements that are vital for the Afghan people were nor reflected in the text of the resolution.
Thirdly, the authors ignored our proposal to have the document state the adverse effects that freezing of Afghan financial assets had on the economic and humanitarian situation in the country, and mention the fact that humanitarian assistance to Afghanistan must imperatively comply with the UN guiding principles, stipulated in UNGA resolution 46/182.
The first concern Nebenzia mentions is a node to the Chinese concerns. The second one is based on a concern the Taliban had raised when they declined to prolong the U.S. evacuation of educated Afghan people. The third one is the most important.
Russia had proposed to lift the block on Afghan assets. The U.S. has rejected that. That makes it quite obvious that the U.S. intends to keep these in place. It will use them to make demands which the Taliban will be unable to fulfill.
At the same time the U.S. will uses its ISPK (ISIS-K) and 'Northern Alliance' assets in Afghanistan to continue the war and to make successful efforts to govern Afghanistan impossible.
It will then blame the Taliban for the inevitable results.
Dr. Jessica Rose has a BSc in Applied Mathematics and completed her MSc in Immunology at Memorial University of Newfoundland in Canada. She completed her PhD in Computational Biology at Bar Ilan University and then did her first Post Doctorate at the Hebrew University of Jerusalem in Molecular Biology.
Estimating the number of COVID vaccine deaths in America
by Jessica Rose, Mathew Crawford
Abstract: Analysis of the Vaccine Adverse Event Reporting System (VAERS) database can be used to estimate the number of excess deaths caused by the COVID vaccines. A simple analysis shows that it is likely that over 150,000 Americans have been killed by the current COVID vaccines as of Aug 28, 2021.
The Vaccine Adverse Event Reporting System (VAERS) database is the only pharmacovigilance database used by FDA and CDC that is accessible to the public. It is the only database to which the public can voluntarily report injuries or deaths following vaccinations. Medical professionals and pharmaceutical manufacturers are mandated to report serious injuries or deaths to VAERS following vaccinations when they are made aware of them. It is a “passive” system with uncertain reporting rates. VAERS is called the “early warning system” because it is intended to reveal early signals of problems, which can then be evaluated carefully by using an “active” surveillance system.
The VAERS database can be used to estimate the number of deaths caused by the COVID vaccines using the following method:
1. Determine the significant adverse event under-reporting multiplier by using a known significant adverse event rate
2. Determine the number of US deaths reported into VAERS
3. Determine the propensity to report significant adverse events this year
4. Estimate the number of excess deaths using these numbers
5. Validate the result using independent methods
Determining the VAERS under-reporting multiplier
One method to discover the VAERS underreporting analysis can be done using a specific serious adverse event that should always be reported, data from the CDC, and a study published in JAMA. Anaphylaxis after COVID-19 vaccination is rare and occurs in approximately 2 to 5 people per million vaccinated in the United States based on events reported to VAERS according to the CDC report on Selected Adverse Events Reported after COVID-19 Vaccination. Anaphylaxis is a well known side effect and doctors are required to report it. It occurs right after the shot. You can’t miss it. It should always be reported.
A study at Mass General Brigham (MGM) that assessed anaphylaxis in a clinical setting after the administration of COVID-19 vaccines published in JAMA on March 8, 2021, found “severe reactions consistent with anaphylaxis occurred at a rate of 2.47 per 10,000” people fully
vaccinated. This rate is based on reactions occurring within 2 hours of vaccination, the mean time was 17 minutes after vaccination. This study used “active” surveillance and tried not to miss any cases.
When asked about this, both the CDC and FDA sidestepped answering the question. Here’s the proof at the CDC (see page 1 which incorporates the CDC response to the original letter on pages 2 and 3).
As noted in the letter, this implies that VAERS is underreporting anaphylaxis by 50X to 123X. The CDC chose not to respond to the letter.
Is the anaphylaxis under reporting rate a good proxy for reporting fatalities? Since anaphylaxis is such an obvious association, one could argue that the rate would be a lower bound. Others would argue that deaths are more important and would be more reported than anaphylaxis.
We don’t know, but it doesn’t matter because this is just an approximation to get to a ballpark figure. In general, most of us think It is therefore entirely reasonable to assert that deaths are reported even less frequently than anaphylaxis since deaths are not as proxmate to the injection event.
The MGH study used practically identical criteria as CDC used in its study to define a case of anaphylaxis. We ran the numbers ourselves and confirmed this.Therefore, a conservative estimate (giving the government the greatest benefit of the doubt) would use 50X as the underreporting rate.
However, after the MGH study was published, one doctor pointed out that doctors were more careful to avoid anaphylaxis; there was more careful screening of people likely to have anaphylaxis, and they were advised to see their allergist and take more precautions prior to
vaccination. This sort of thing would overstate the numbers above.
So we ran the numbers BEFORE the JAMA study appeared and got a more conservative estimate.
Here’s the data from Google (which uses World In Data):
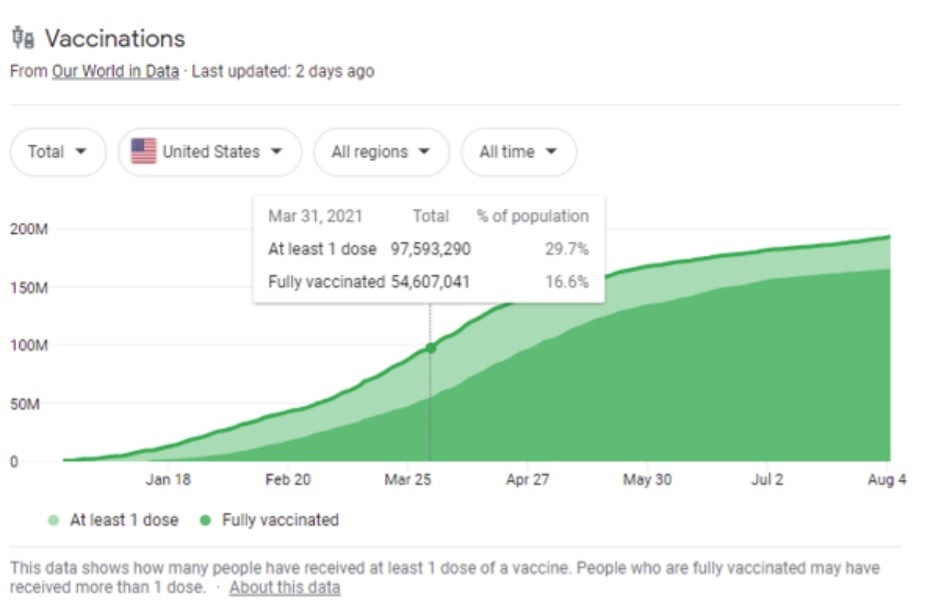
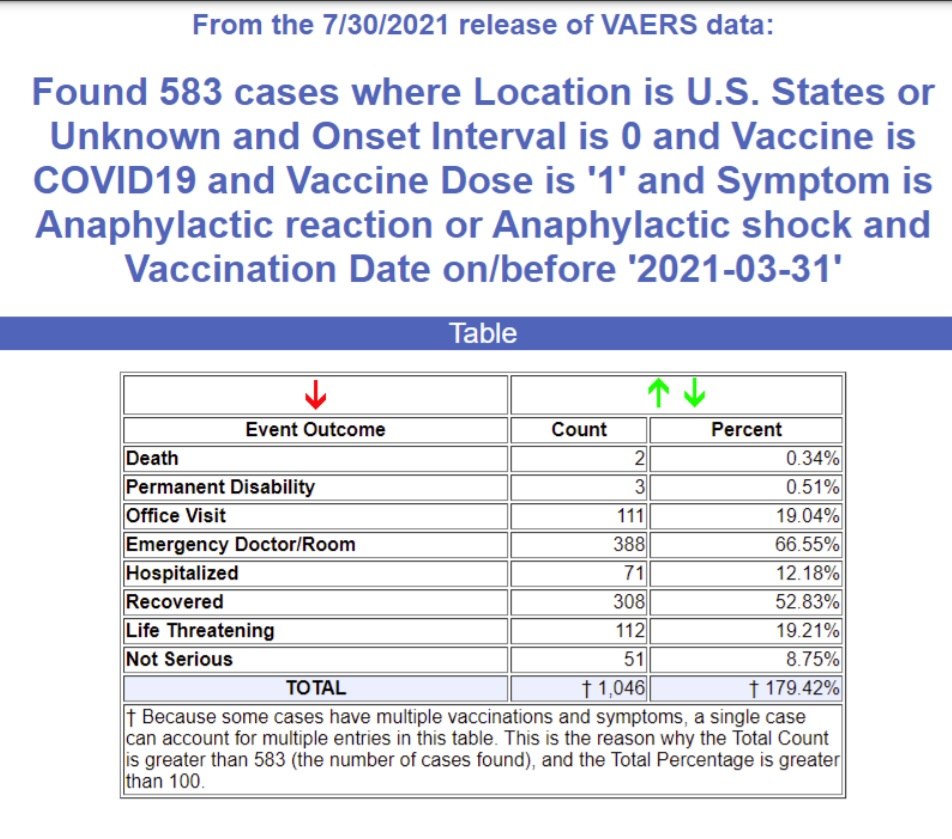
We’ve vaccinated 97.5M people from the start thru March 2021 and there were 583 reports in VAERS who had an anaphylaxis reaction on their first dose. This suggests that the underreporting rate is 41X.
Other estimates such as How Underreported Are Post-Vaccination Serious Injuries and Deaths in VAERS? suggests a 30X factor based on VAERS.
However, this used a serious adverse event rate from the Pfizer Phase 3 study which we believe under-reported these events for three reasons:
1) the patients were much healthier than average with a 10X lower rate of cardiac arrest than the general public (for example),
2) it was hard to report adverse events if you were in the trial (the evidence of this was unfortunately deleted when Facebook removed the vaccine side effect groups), and
3) there was known malfeasance in the reporting of adverse events in the 12-15 year old trial where the paralysis of 12-year-old Maddie de Garay was never included in the trial results and the FDA and CDC refused to investigate and the mainstream media would not report on it.
The point of this paper is not to find the exact number of deaths, but merely to find the most credible estimate for deaths. We think that anaphylaxis is an excellent proxy for a serious adverse event that, like a death, should always be reported so we think 41X is the most accurate number.
Our hypothesis is that this number will be applicable to deaths as well. In order to confirm our hypothesis, we must derive the death count in different ways and see if we come up with the same answer.
When used for less serious events, such as a headache, it’s likely that 41X is going to be low since such events are less likely to be reported. So our hypothesis is that 41X is a safe, conservative factor useful for both serious and less serious adverse events.
Determining the number of US deaths
As of August 27th, 2021, a search of the VAERS database shows that there are 7,149 domestic deaths in the VAERS database (US/Territories/Unknown).
Estimate the propensity to report for 2021
Healthcare providers have been required by law to report serious adverse events in VAERS with passage of the National Childhood Vaccine Injury Act (NCVIA) in 1986.
Therefore, nothing has changed this year vs. previous years:
1. no new legal requirements,
2. no noticeable promotion or incentives to report into VAERS.
Even when there are strong promotions to report adverse events as there was with H1N1 in 2009 where there were serious campaigns to raise the visibility of reporting, this didn’t impact the background fatality event reporting: it didn’t go up at all in 2009 and 2010 as can be seen from the graph below.
In short, it is extremely difficult to materially change the propensity to report serious adverse events into the VAERS system; it is remarkably consistent from year to year. This makes sense: old habits die hard… behaviors are hard to change. And there was nothing “new” this year to incentivize a massive change in behavior.
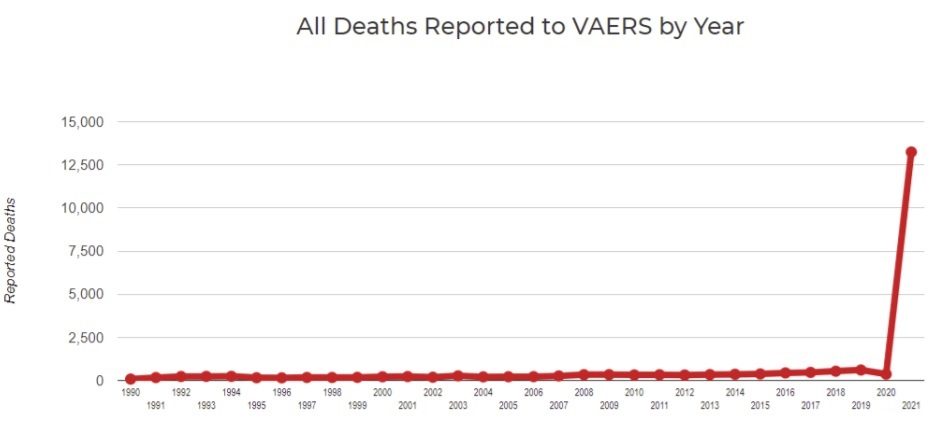
Look at the weekly data below. The massive increase in reporting pretty much happened almost instantaneously as soon as the vaccines started rolling out. And it was proportional to the rollout. That is not how behavioral change works… behavioral change would happen very lowly over time; especially if you are trying to get doctors to change their long term behaviors. The reporting basically followed the rollout of the vaccine. Doctors were more likely to report to VAERS this year because there were simply more events to report. We have verified that by talking directly to the doctors as the reason they are reporting more for these vaccines.
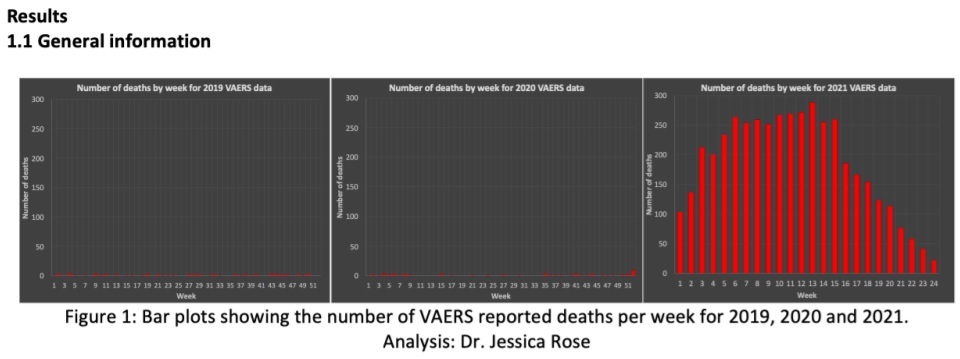
To double check our hypothesis that the propensity to report is unchanged this year, we ran VAERS queries using symptoms unrelated to those impacted by the vaccines. We ruled out any known comorbidities like diabetes and obesity since these would likely be elevated since there are more adverse events.
We found that the reporting rates for these unrelated events (listed in the table below) are no different this year than in previous years and for some of these events, the reporting rate is dramatically lower. Note that the number in the 2015-2019 column is the total for the 5 years, not an average annual amount. The Rate Increase is an X factor (i.e., A/B*5)
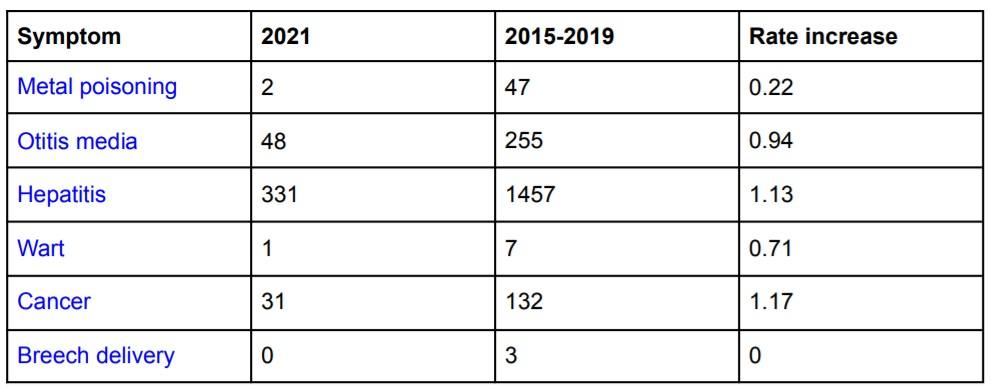
A third way to see that 2021 isn’t simply over-reporting normal background adverse events is to look at the “adverse event (AE) footprint” of the vaccine. You do that by listing adverse events on the X-axis and AE counts on the Y-axis. If there is over-reporting this year, the overall outline of the boxes will be exactly the same as previous years, and they will just be higher due to the higher propensity to report the same types of events. As you can see, that is not the case here.
This vaccine is definitely causing a completely different “shape” of severe adverse events. Here we show 2018, 2019, 2020, and 2021.
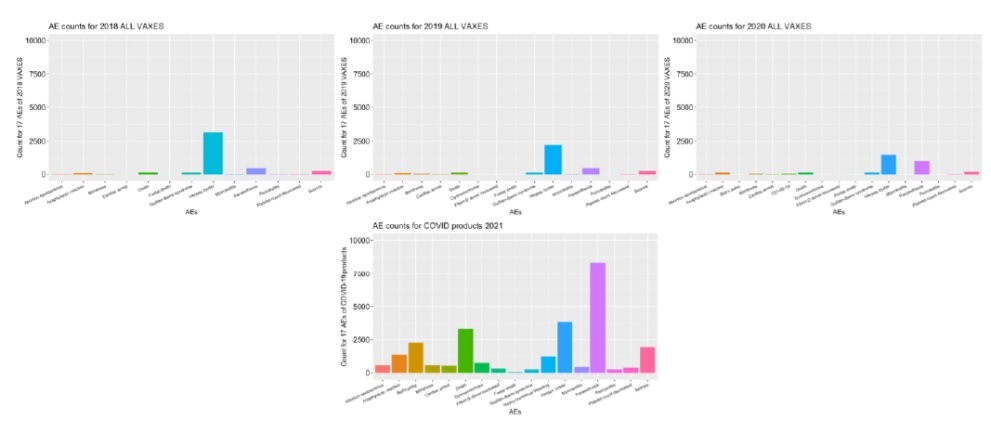
For a more detailed set of vaccine fingerprints (COVID vs. other vaccines), see these charts from Jessica Rose.
A fourth way to confirm there wasn’t over-reporting is through informal physician surveys.
In our informal physician surveys we saw a bias to under-report serious adverse events in order to make the vaccines look as safe as possible to the American public since most physicians believe they are hurting society if they do anything to create vaccine hesitancy.
Secondly, we’d estimate that at least 95% of physicians have completely bought into the “safe and effective” narrative and thus any event that they observe they deem as simply anecdotal and don’t bother to report it since it couldn’t have been caused by such a safe vaccine that appeared to do so well in the Phase 3 trials.
Determining the number of excess deaths caused by the COVID vaccines
There are three ways to estimate the number of excess deaths caused by the vaccine. Using these three methods we can estimate the low and high likely bounds for the number of excess deaths caused by the vaccine:
1. Subtract the average number of background deaths in previous years
2. Use 86% based on the analysis in the Mclachlan study
3. Use 40% based on the estimate of Dr. Peter Schirmacher one of the world’s top pathologists
Here is the result we get from the three methods:
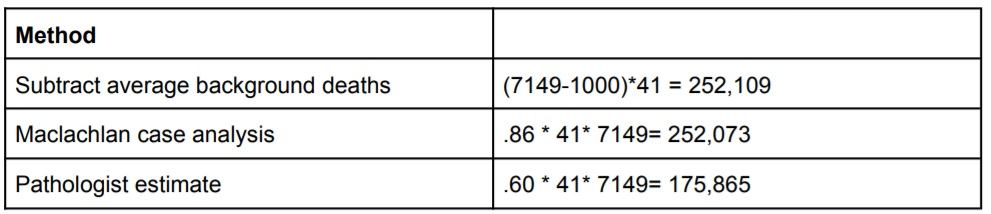
In the first method, we used 500 background deaths as normal for a year since the propensity to report is the same this year as in previous years as shown earlier. However, we should assume that the age cohort is older this year than previous years. For example, here are the vaccination rates shown in a CDC report for influenza:
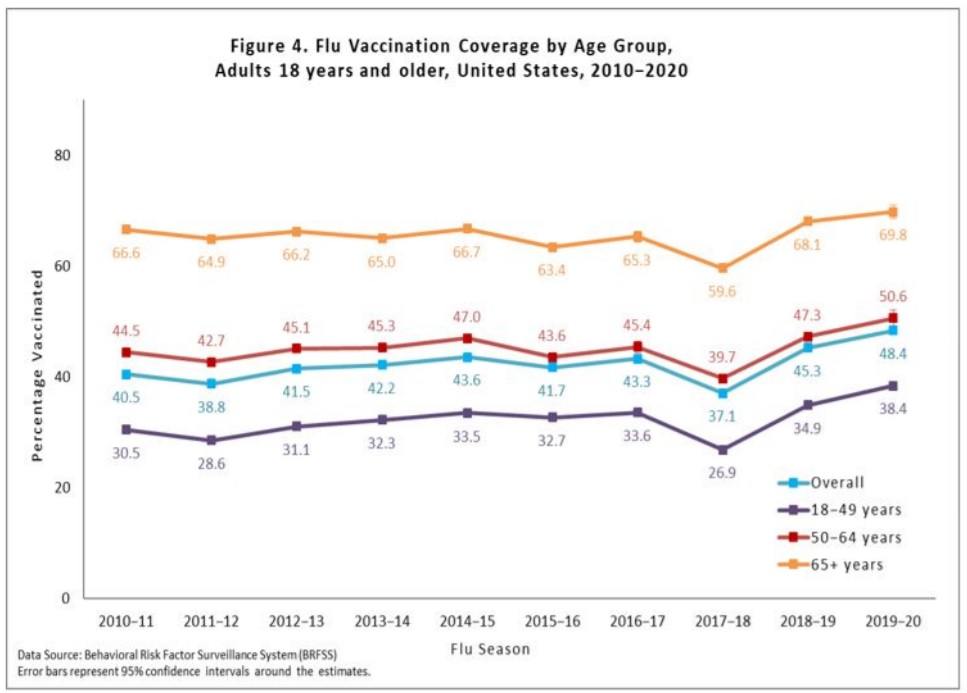
So a conservative estimate is to take the <500 deaths per year and increase it by 50% to more than account for a shift to higher ages so subtract 750 background deaths.
In the second method, McLachlan examined 250 VAERS reports in detail and concluded that up to 86% of the deaths were consistent with the vaccine being causal for the death. We use the higher number, because using a lower number makes no sense since it leads to a background death rate that would be excessive compared to previous years (.14*7149 = 1,000 which is already higher than the 500/yr background death rate).
The third method uses estimates made by Dr. Peter Schirmacher, one of the world’s top pathologists, for the % of deaths examined by autopsy within 2 weeks of the vaccine that were clearly caused by the vaccine.
The range was from 30% to 40% and we used the high end of the range since we believed that in making a potentially career-ending revelation such as this that Dr. Schirmacher was being extremely conservative and only estimating what he was 100% certain of proving.
40% is likely very conservative since Norway was under no such reputational pressure and in the the first 13 bodies they assessed, 100% of the deaths were found to be caused by the vaccine (see Norwegian Medicines Agency links 13 deaths to vaccine side effects). Therefore using a 60% number seems relatively conservative (less than the 65% average of 30 and 100).
Therefore we have a range of death estimates from 148,000 to 216,000 deaths which averages to 182,000 deaths.
Validation using other methods
In order to validate that our estimates are reasonable (or simply that the evidence was more likely consistent with the hypothesis that the vaccine does more harm than good), we looked at four different quantitative methods from very small to very large and summarized their estimates in the table:
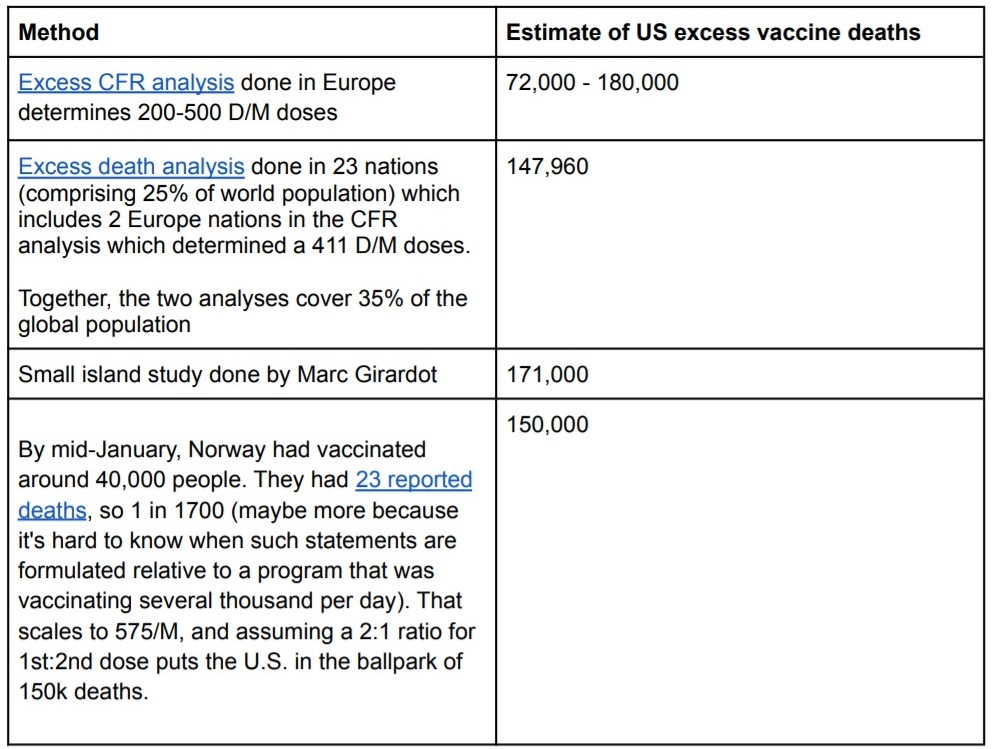
There are additional qualitative methods that show a large number of deaths. The point of these method is to show that the FDA assumption that “the vaccines are safe and all of the reports in VAERS are background events” is not even close to being true.
Example 5: The pericarditis data below shows that the number of events for these vaccines are anything but safe: they generate myocarditis/pericarditis at 860 times the rate of the typical flu vaccine in a year.
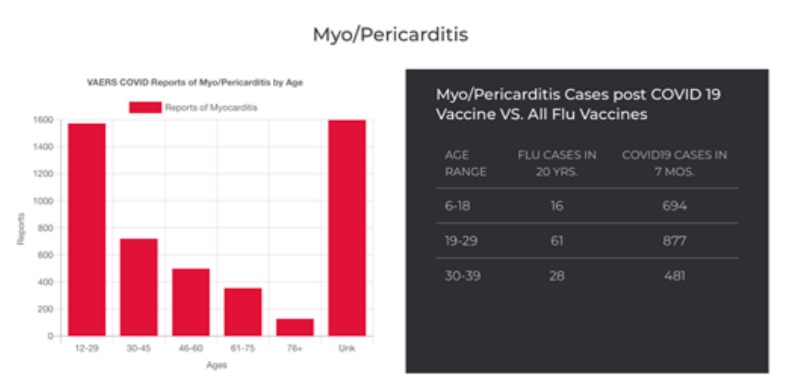
A friend of ours got pericarditis right after getting the influenza vaccine when she was 30 years old. It took her two years to recover. The heart muscle never really regenerates like other organs unfortunately.
Example 6: A total of 23 deaths have been reported in connection with the corona vaccination to the Norwegian Medicines Agency. Of those, 13 deaths were linked to the vaccine’s side effects. The other 10 haven’t been evaluated yet. Thus, 100% of the reported deaths have been deemed to be caused by the vaccine. If the vaccine is perfectly safe and has killed no one, then this is statistically impossible. Someone is lying. The fact that there are no autopsies being done in the US in public view suggests that it is more likely that the CDC is lying than the Norwegian Medicines Agency.
Example #7: An analysis of excess deaths in Israel, especially among young people, that was done by Dr. Steven Ohana, clearly shows a huge rise in excess deaths that have no explanation other than the rollout of a mass vaccination program.
Example #8: A published analysis of VAERS data by Dr. Jessica Rose and a more recent analysis of VAERS data done by Christine Cotton show massive numbers of cardiovascular and neurological adverse events occurring within temporal proximity to the injection date.
Example #9: Causality of these adverse events is confirmed using Dose 1 and Dose 2 studies done by Dr. Jessica Rose.
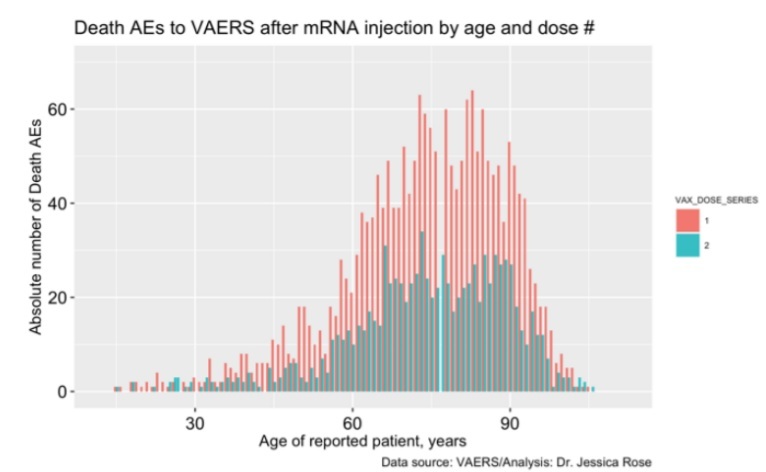
Example #10: If the vaccine is perfectly safe, the number of deaths would be equally likely after the first dose vs. the second dose since both are effectively “non-events.”
Because there are 15% fewer people who get the second dose than the first dose, we should expect the blue bars to be uniformly 15% lower than the red bars. This is not the case here. If the vaccine kills 50% of the 1% most vulnerable people each time it is administered, this can explain the dramatic drop off in events.
Another explanation is that the vulnerable population experienced severe adverse events following Dose 1 and thus chose not to get a second Dose despite the societal pressure (vaccine mandates, peer pressure, etc) to do so.
It is likely a combination of both effects. Here is an example of this from a comment posted to TrialSiteNews on A New Low For the FDA:
Whatever the cause, evidence to support the arisal and reporting of multiple severe adverse events that are dose-related is a very strong safety signal that requires investigation.
Example #11: The same commentary as before applies for cardiac arrest; a safe vaccine should have blue bars on average 15% below the red bars.
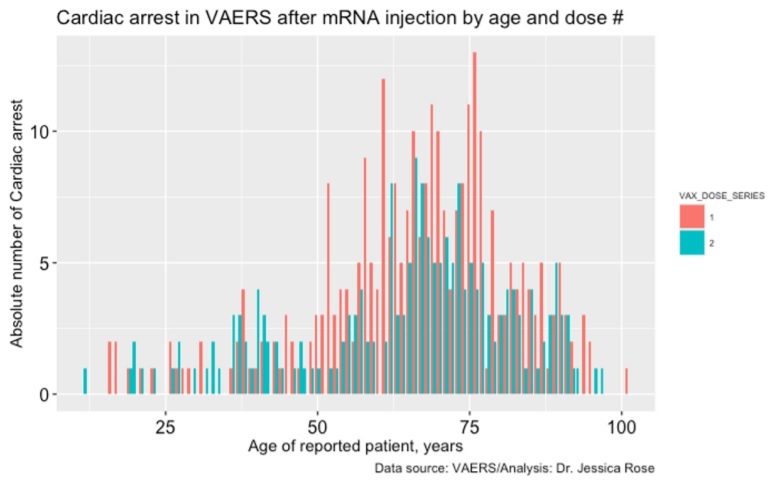
Example 12: Absolute numbers of VAERS reports plotted according to “time to death” is very revealing. We don’t know what the exact distribution of timing looks like because this was never measured. But we speculate that maximum accumulation of spike protein is achieved around 24 hours or so after injection and then it plateaus after that point as the mRNA disintegrates. Therefore, we would expect to see a death peak more than 24 hours after injection, i.e., on Day 1 and not on Day 0 This is exactly what happens in practice:
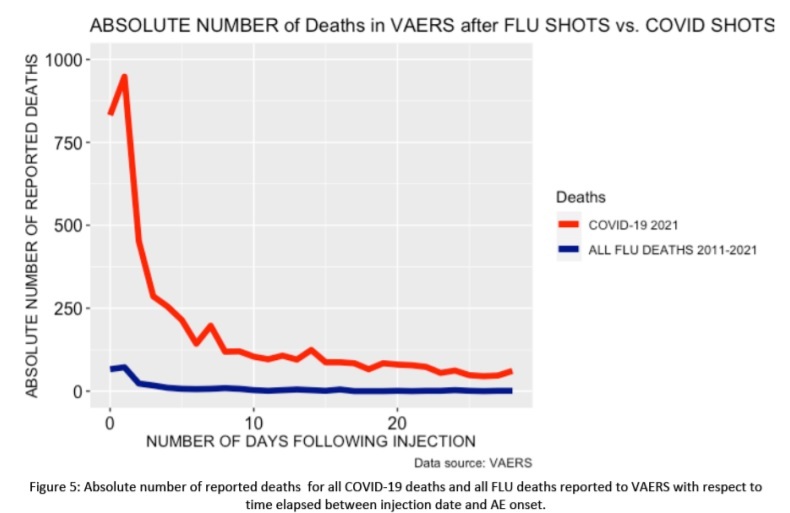
If these were simply random background deaths, we would expect to see a peak on the first day since that has the highest propensity to report, and it would drop from there; it would never peak on Day 1. In the graph above, we plot 8 months of the COVID19 vaccine reports compared to all death reports from all influenza vaccines for the past 10 years combined. So the blue line at 0 is 20 years of death reports, it is not an annual average. In short, the killing power of this vaccine is at least 200X greater than the influenza vaccine and probably a lot more than that since background deaths are included in both red and blue bars.
Furthermore, the shape of the two curves is completely different. The combined flu deaths are relatively flat with a slight rise in the first few days. The COVID vaccine generally kills people very quickly, and then gradually over time from there.
Example 13: A visual way to show that excess deaths are likely caused by the vaccine is to plot vaccinations and deaths on the same axis using data from the COVID-19 data explorer. For Israel we get this chart which shows a correlation between vaccine booster doses given
(cumulative booster doses per 100 people) and average daily deaths per million: they track almost in lock step.
This is hard to explain any other way.
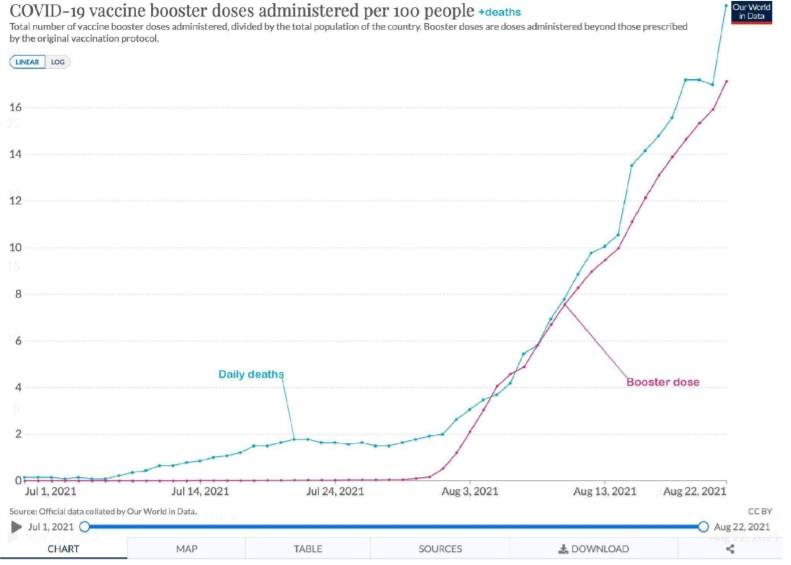
In summary, the qualitative and quantitative confirmation techniques we used were all independent of each other and of our main method, yet all were consistent with the hypothesis that the vaccines cause large numbers of serious adverse events and excess deaths and are inconsistent with the null hypothesis that the vaccines have no effect on mortality and have a safety profile comparable to that of other vaccines.
We were not able to find a single piece of evidence that supported the FDA and CDC position that all the excess deaths were simply over-reporting of natural cause deaths.
Serious adverse events elevated by the COVID vaccines
We made a table comparing the rate of adverse events this year relative to the annual VAERS incidence rate reported for all vaccines over the period from 2015-2019 for ages 20 to 60.
We limited the age range to show that these events are affecting young people and not just the elderly. Also, the signal to noise ratio is much stronger in this younger age group since they are less likely to suffer “background” adverse events. A value of 473 means the rate reported in VAERS for the COVID19 vaccines in 2021 was 473 times higher than what is typical for all vaccines combined in the typical average year.
Nearly all serious adverse events we looked at were strongly elevated compared to the expected normal baseline event rate. This table is useful when assessing whether the vaccine may have been involved in causing death in cases.
The symptoms listed here are consistent with the presumed mechanism of action for how these vaccines kill people (producing spike protein throughout the body that cause inflammation, scarring, and blood clots).
Surprisingly, only a few of these symptoms appear in the labeling of the recently approved Pfizer vaccine. Thus, this table is important and timely.
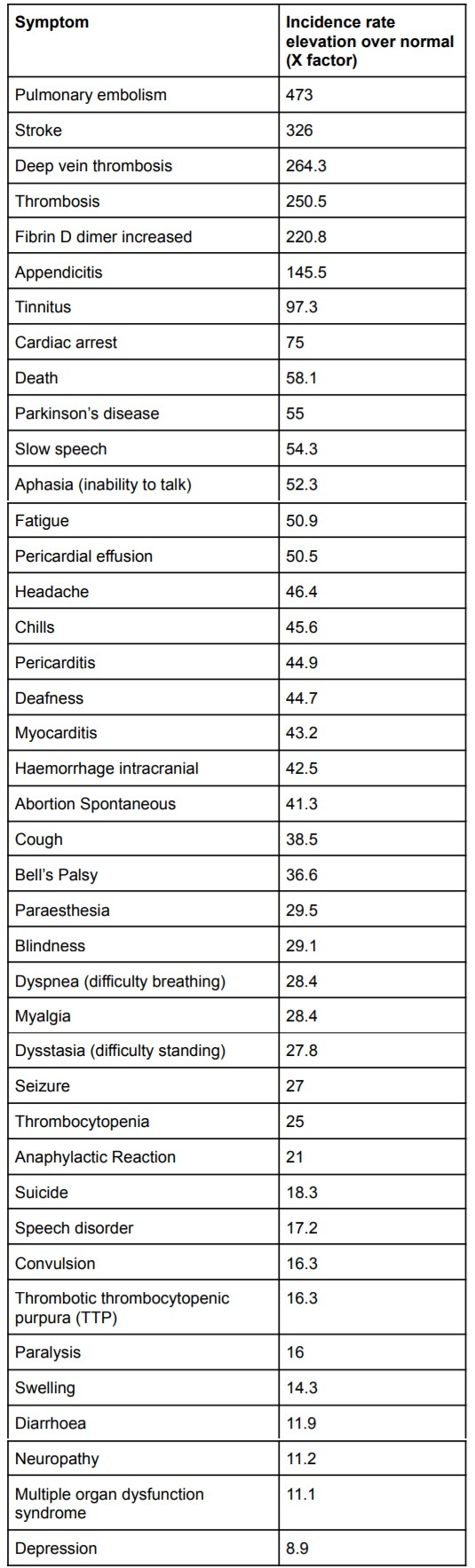
Child deaths are consistent with symptoms elevated by the COVID vaccines
Perhaps most troubling of all is child deaths.
The CDC VAERS review of the 12-17 year old data released on July 30, 2021 showed there were 345 cases of myocarditis and 14 deaths. Unlike old people, kids don’t spontaneously die every day at anywhere near the same rate.
Using the table above and investigating each death, all of these deaths where there was sufficient detail in the death report showed that it involved one or more of the symptoms listed in the elevated adverse event table.
14*41 = 574 deaths
There are fewer total child deaths for 17 and under (which is a much wider age range than above) in the entire pandemic.
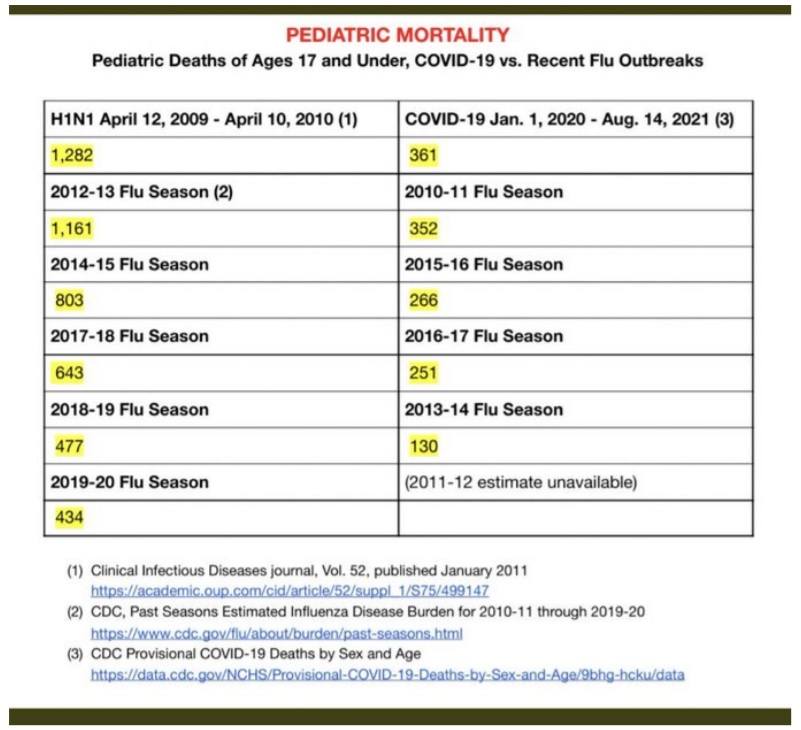
Therefore, the cost benefit case for children isn’t there.
Lack of a stopping condition
In 1976, they halted the H1N1 vaccine after 500 GBS cases and 32 people died.
However, there is no stopping mortality condition for these vaccines. We are likely at 150,000 deaths and counting and nobody in the mainstream medical establishment, mainstream media, or Congress is raising any concerns.
No member of the medical community is calling for any stopping condition nor autopsies. We find this troubling.
Negative efficacy
This paper shows that the vaccines we received may well shortly become completely useless to protect us and, to make matters worse, might enhance the ability of future variants to infect us due to vaccine enhanced infectivity/replication, rather than “classical” ADE.
In short, even if the vaccine were perfectly safe and killed no one, it’s rapidly becoming a net negative based on efficacy alone.
We are starting to see evidence of this today. UK data destroys entire premise for vaccine push. August 21. 2021. “Again, 402 deaths out of 47,008 cases or 0.855% CFR in fully vaccinated, and; 253 deaths out of 151,054 cases or 0.17% CFR in unvaccinated. If you get Covid having been fully vaccinated, according to this UK data, you are five (5) times more likely to die than if you were not vaccinated!”
All-cause mortality is the single most important thing to focus on and it’s not there
Today, most people focus on the relative risk reduction of the vaccines against infection, hospitalization death from COVID. They pay less attention to the absolute risk reduction from COVID. And they pay no attention at all to the absolute all-cause mortality benefit.
The funny thing is that we should be paying attention to these in the opposite order that we listed them.
All-cause mortality is key. If there is no improvement in all-cause mortality, nothing else matters.
In short, say our vaccine reduces the risk of dying from COVID by 2X. But it came at a cost, e.g., increasing your risk of dying from a heart attack by 4X. And let’s say both events are equally likely (which they aren’t). Then you’ve made a bad decision… you’re more likely to die if
you took the vaccine.
Here are the results from the Pfizer 6-month study:
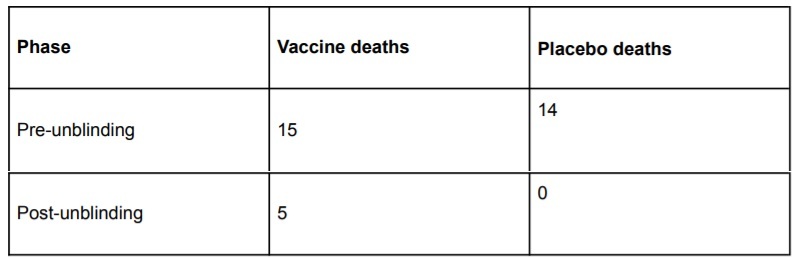
Discussion of these results is quite a bit more complex than we have space to go into here, but these are the basic stats. For more information, see the 10-page discussion of the Pfizer 6 month trial at Why so many Americans are refusing to get vaccinated.
All the all cause mortality numbers are negative from the 6 month Pfizer study. This is not a surprise: it is caused by the high rates of adverse events we’ve already discussed.
There is no evidence of statistically significant mortality improvement.
If there was the CDC, FDA, and NIH would certainly let us know. But just the opposite happened: when the Pfizer 6 month study came out, the mainstream media and mainstream medical scientists were silent on the lack of all-cause mortality evidence. It didn’t even make it into the abstract. The fact that 4 times as many people were killed by cardiac arrest wasn’t even mentioned.
When you combine (1) the negative efficacy of the vaccine with (2) the negative all-cause mortality benefit, it’s impossible to justify vaccination. Either alone is sufficient to kill the benefit; both of them together makes things even more difficult for recommending vaccination.
The bottom line is clear: If you got the vaccine you were simply more likely to die. The younger you are, the greater the disparity.
Early treatment using repurposed drugs has always been the safer and easier way to treat COVID infections
Early treatment protocols such as those used by Fareed and Tyson have been shown to provide more than a 99% relative risk reduction, work for all variants, and the drugs don’t maim or harm the recipients. It is baffling that we are ignoring these treatments and waiting for more evidence when we have a vaccine which appears to kill more people than it saves, soon will be completely useless against future variants, and is likely going to make things worse for the recipient by enhancing replication and/or infectivity.
There are also a variety of prophylaxis techniques that are simple, safe, and highly effective including. The precautionary principle suggests that if there is evidence from a credible source of the benefits of these treatments (which there are), that doctors.
Because early treatments using repurposed drugs don’t create a measurable risk of death, the all-cause mortality for early treatments is always positive.
Many people assume that vaccination is the only path forward. It isn’t. Allowing people to be infected and develop recovered immunity leads to immunity which is broader against variants and lasts longer. See “Recovered immunity is broader and longer lasting” in this document.
It is instructive to compare Israel with India.
Israel is one of the most vaccinated countries on Earth with 80 percent of citizens above the age of 12 fully inoculated. As of Aug 24, 2021, Israel reported 9,831 new diagnosed cases on Tuesday, a hairbreadth away from the worst daily figure ever recorded in the country—10,000—at the peak of the third wave.
At the same time, India recorded 354 deaths in a day, Israel was reporting 26 deaths and record high cases. Here’s how they stack up:
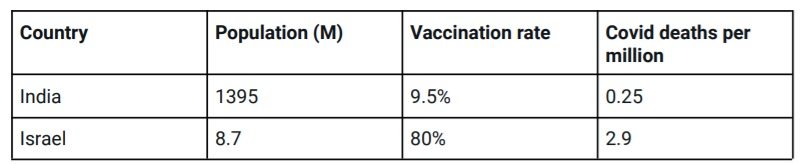
Obviously, India has 11.6X lower deaths per capita than Israel.
The conclusion is clear, vaccination is not the only solution nor the best solution.
Summary
Using the VAERS database and independent rates of anaphylaxis events from a Mass General study, we computed a 41X under-reporting factor for serious adverse events in VAERS, leading to an estimate of over 150,000 excess deaths caused by the vaccine.
The estimates were validated multiple independent ways.
There is no evidence that these vaccines save more lives than they cost. Pfizer’s own study showed that adverse events consistent with the vaccine were greater than the lives saved by the vaccine to yield a net negative benefit. Without an overall statistically significant all-cause mortality benefit, and evidence of an optional medical intervention that has likely killed over 150,000 Americans so far, vaccination mandates are not justifiable and should be opposed by all members of the medical community.
Early treatments using a cocktail of repurposed drugs with proven safety profiles are a safer, more effective alternative which always improves all-cause mortality in the event of infection and there are also safe, simple, and effective protocols for prophylaxis.
This is — without a doubt — the best articulation as to the ethical problem posed by mandatory vaccines or vaccine passports.
Dr. Julie Ponesse explains the dilemma in a persuasive manner.
Watch the whole 4 minute video, split across 3 segments in this thread

As the pandemic rolled into its second year, I became concerned that the psychosocial fallout of the pandemic, and especially the response at the global and local levels, could represent an existential threat to permaculture and kindred movements. At one level, this threat is the same as that to families, workplaces, networks and organisations more generally, where a sense of urgency to implement the official response, especially lockdowns and mass vaccination, is producing a huge gulf between an ever more certain majority and a smaller minority questioning or challenging the official response.
My aim in this essay is to focus on the critical importance of using all our physical, emotional and intellectual resources towards maintaining connections across what could be a widening gulf of frustration and distrust within our movement, reflecting society at large. I want to explore how permaculture ethics and design principles can help us empathetically bridge that gulf without needing to censor our truth or simply avoid the issues.
While the pandemic and the responses to it will pass in time, I believe the future will be characterised by similar issues that test our ability to tolerate uncertainty and diversity and to thus exercise solidarity within kin, collegiate and network communities of practise.


International Permaculture Day May 2013 Daylesford Community Garden
Future Scenarios and the Brown Tech future
The positive grounded thinking that characterises permaculture has always been informed by a dark view of the state of the world and long-term emerging threats. Future Scenarios is my 2008 exploration of four near-future ‘energy descent’ scenarios driven by the variable rates of oil and resource depletion on the one hand and rate of onset of serious climate change on the other. Six years later, I wrote the essay ‘Crash on Demand: Welcome to the Brown Tech Future’ where I ‘called’ Brown Tech as being the already emergent scenario.
In the longer version of this ‘Pandemic brooding’ essay, I review and reinterpret this work in light of the pandemic and responses to it.
Permaculture pluralism
Anyone involved in permaculture knows that permies can come to quite different conclusions about what is the most ethical and practical solution to the same problem. For example faced with marauding wildlife, some will go to considerable expense (and resource consumption) building elaborate fences, anti-aviaries and other deterrents to separate wildlife from food. Others will treat the wildlife as another abundance of the system to be harvested. Various permaculture principles, as well as the fundamental ethic of Care of Earth, might be invoked to support both approaches.
Likewise, many permies believe taxation is essential to redistribute resources from places of abundance to those of scarcity and as an expression of solidarity essential to any functioning, let alone ethical, society. Others see almost all the expenditure by governments of tax revenues as representing rape of Mother Earth’s abundance and theft from Indigenous peoples, and further as either downright evil or at best a bandaid covering festering wounds. An ethical response is to minimise taxpaying (by reducing income and consumption). Again, design principles and ethics can be invoked to support either position.
From my perspective, grappling with the ethical and systemic issue is more important than the notion that there might be a correct answer, and therefore a wrong answer, to the challenge. In the past, there have been heated debates, and agreements to disagree, but rarely would participants in permaculture design courses, convergences or networks see the answers of others as reasons to reject permaculture. Many celebrate personal actions as small-scale experiments with their good, bad and interesting outcomes informing other experiments, especially the next generation’s, as we muddle through energy descent to hopefully more benign, or at least less-bad, futures.


Pandemic flavoured Brown Tech
I believe the pandemic and the responses to it represent a major turning point in crystalising the Brown Tech future. It ticks so many boxes:
- a nature-driven crisis which has been long predicted, and to some extent, planned for
- rolling uncertainty that progressively breaks down past expectations
- a crisis which, like a war, requires the suspension of normal economic activity, personal rights and governance processes
- a demand for strong action by government for the common good informed by science
- a revival of Keynesian policies including a massive increase in government debt
- an enemy (the virus) that can be easily demonised without there being too many defenders to ignore or silence
- strong censorship of broadcast media and novel efforts to censor social media to sideline debate that could undermine the rapidly emergent and evolving program.
If the crisis is not solved, then demonisation progressively shifts to those resisting the plan.
This situation is creating the fork in the road where some permies will find themselves (perhaps surprisingly) following the program, while others will have become certain that they will at least quietly resist complying to some degree or other, right up to a radicalised public resistance, whether that be through resigning from work, street protest or satirical art.
We can learn and gain, individually and collectively, from these increasingly divergent paths – but the learnings could be painful. Let’s consider the benefits that might have led permies down one or another path, perhaps unwittingly, to increasingly polarised positions.
The mainstream plan
Although there are differences of emphasis and policies around the government responses to the pandemic, these debates are around the margins, even if they are at times heated. Most fundamentally, the mainstream plan, informed by the scientific and medical establishment, takes the following as self-evident:
- The virus is an existential threat to society that must be contained and disarmed if not eliminated before an establishment of some hoped-for, tolerable new normal.
- Social distancing, disinfectant cleaning, testing, contact tracing, masks and various levels of quarantine, border controls and lockdowns are the only mechanisms available to prevent collapse of the health system and deaths escalating to horrific levels in the short term.
- Novel vaccine technology is the only real hope for a tolerable new normal.
- To achieve effective herd immunity and minimise death, some great majority of the adult population and probably children need to get vaccinated as soon as possible.
- The adverse effects of these provisionally approved vaccines are minor and/or rare and much less than the risk of the disease.
- Preventative and early treatments are at best of marginal value, or more likely based on false hope and fraud.
- The suspension of normal civil liberties is a necessary, albeit temporary, measure to achieve the plan in a timely fashion and reduce the suffering both from the virus and the plan itself.
- People who actively resist the plan need stronger social, economic and, where necessary, legal sanctions to ensure their actions don’t prevent the plan from working for the common good.
- Apart from debate around the margins about how best to respond to these givens, debate and questioning at the level of science, logistics, economics, law, politics, media and social media is not just unnecessary, but an existential threat to the plan and society at large, so must be prevented by unprecedented means.
- It is the responsibility of every citizen to play a part in the plan, be bold in convincing those who are hesitant, and challenging those not following the plan, especially those actively resisting it.
Permies following the plan are likely to see themselves as being part of a society-wide collective effort to minimise pain and suffering in the aged, the disadvantaged and those in poor health; a choice in favour of collective and longer-term gain at the cost of individual and short-term sacrifice. For many of us, this is a perfect metaphor for what is needed to address the climate emergency. By accepting what appears to be a broad consensus of global, national and local medical and scientific experts, we avoid the protracted debate and lack of a technical consensus that has stymied governments in initiating strong action to address the climate emergency.
For permies in despair about the waste and dysfunction of the consumer economy, the closure, albeit temporary, of many discretionary services and businesses is a taste for how we might need to decide what is important; maximum consumer choice for the affluent versus the provision of basic needs for all. The personal sacrifice and adaptation to difficulties, including stay-at-home lockdown, have been opportunities to focus more on the important things in life and get a taste of what social solidarity feels like.
Reports of contrarian views seem to mostly come from sources contaminated by association with climate denial and other views we categorically reject. The resisters’ outrage looks to many like just more selfish, science denying and ignorant right-wing rednecks, trying to prevent collective wisdom and social solidarity from working. Familiar powerful bad players in global corporations or nation states have been replaced by much more immediate angry undesirables, who without much power or vision, could wreck the hard work of the collective to create a workable new normal.
The dissident view
It is more difficult to generalise about those who question or reject the program. A great diversity of views, explanations, feelings and actions flourish in an environment of unprecedented censorship. While there is great sensitivity about the term ‘censorship’, let alone ‘propaganda’ by those supporting the plan, for those on the other side, it is astonishing how rapidly the axe has fallen on enquiry, and debate, in the mainstream media, social media, workplaces and families, let alone in defence of what – until very recently – most of us took as our inalienable rights.
For many permies, the pandemic seems another example of hyped threat like the ‘war on weeds’, ‘war on drugs’, ‘war on terror’ used to manipulate the population to comply with some version of disaster capitalist1Disaster capitalism feeds off natural (climate change) and other disasters to provide recovery and reconstruction services funded by the public that typically benefit the corporate providers and contribute to ongoing dependencies. The term was used by Naomi Klein to describe the evolution of late stage capitalism over recent decades. solutions. Most sceptics acknowledge the virus as real, but not as dangerous as the cure in lockdowns and other draconian measures. The ‘war on the virus’ seems just as futile or misguided as all the other wars on nature, substances and concepts. So much for trying to have nuanced discussions about viruses as an essential and largely symbiotic mechanism for the exchange of genetic material and mediation of evolution!
While the closure and loss of cafés, gyms and hairdressers might not be a great loss, except to those directly affected, many of us have noticed that the official response to the pandemic tends to follow a pattern of support and strengthening of dominant corporations while leading to the weakening and likely collapse of small business and community self-organised activities.
During the first lockdown, ‘stay at home in your household’ was celebrated as a great plus for people getting the RetroSuburbia message. More recently, the messaging about the problem of shared and multi-generation households being suspect has been building, especially in the working-class western suburbs of Sydney and Melbourne where many of essential and less well paid workers live. We have shifted from a joke about ‘which permie created the pandemic?’ to a gritted teeth recognition that the response to the pandemic is working to vacuum people into another level of dependence on techno-industrial systems.
Many permies have taken advantage of the shift online to network more effectively around the country and the world, but we are deeply troubled by our increasing dependence on mediated experiences and what seems like draconian regulation of informal engagement with people and nature. The concerns for what this is doing to children are far more serious than the loss of the regulated version of social interaction that children get at school.
For many of us, it is completely natural to be sceptical about one big fast answer provided by the giants of the pharma industry, while they have been granted legal immunity for the consequences of their novel products. Many have made the rational assessment that the very low risks of the virus (for most of us at least) seem better than the unknown of a novel technology approved and pushed on a frustrated and frightened population in record time. Some in this camp were sceptical about vaccines in general but most have been influenced by the largely censored views from some leading global experts, that these vaccines are in a totally different risk category to all previous vaccines.
While waiting and seeing what happens next may look selfish to the majority, the difficulty in getting access to data and unbiased interpretation drives many to rely on their gut feelings. One or more examples of spin and manipulation of data by officials, and especially the media, leads to a general collapse in trust about any, and even all, aspects of the official story. For instance:
- Many of us have seen evidence that existing low cost and low risk treatments are available and used effectively in some countries resisting the ‘no available treatment’ orthodoxy.
- Most understand that while the vaccines seemed to give some protection from more severe effects at least in the early stages, they do not appear to stop transmission, at least of the latest variant.
- Many wonder why the build-up of natural immunity from prior exposure to the virus is not considered as part of the solution that should at least be discussed before vaccine passports are implemented.
Concerns about more serious adverse effects of the vaccines, as predicted by some experts, have developed into alarm, anger and resistance as both the evidence increases and efforts at cover up and spin become worse. Extreme consequences that many of us dismissed early on as highly unlikely are now showing up in hard-to-read scientific papers, clinical reports and official records and databases.
A similar process has happened with the official responses. For example vaccine passports are now widely discussed and debated as part of the attempt to get as many people vaccinated as possible, as the efficacy of vaccines falls and concerns about adverse effects lock in resistance by a minority. At the start of the pandemic this possibility was decried as paranoid conspiracy theory.
France has been leading the charge to impose vaccine passports for many public and work spaces including hospitals. It’s hard to assess how large the resistance will be in different countries and circumstances but there are already signs that whole industries will lose a significant part of their workforce as some substantial minority of the population withdraw their work, consumption and investment in the system rather than getting the vaccine. Whether by design, policy stupidity or the unexplained viral power of censored scientists and vaccine doubters to overcome the largest public health education/public relations/propaganda effort in history, it is conceivable that the result could be economic contraction on a much larger scale than has occurred as a result of lockdowns so far.2 I can’t help but see what is unfolding as a bizarre version of my ‘Crash on Demand’ scenario
Economic contraction could mostly be in the discretionary economy, but how would the health system cope with a loss of staff, especially if some combination of ineffective vaccines against new strains and antibody-enhanced disease lead to medically informed people losing faith before the general public? Part of the solution might be doctors and nurses from overseas,3In the week since I wrote this sentence, doctors from overseas are now part of the plan for Australia or the adoption of treatment options for Covid currently being used with success in countries like Mexico and India.
Australia and New Zealand seem to be something of a test bed for the most authoritarian regulations in an attempt to keep Covid as close to zero as possible (and failing). Large numbers of people in other countries see us as a police state and wonder why there hasn’t been more resistance Down Under.
Some of us have noted plans promoted by the World Economic Forum for a Global Reset that will require a command economy to respond to the climate emergency, and that the pandemic is an opportunity to implement some of the structures and processes needed to create what some fear is a global new world order.
For many people, the trajectory from trust to mistrust often leads to either deep depression or an energised anger, mostly focused on the authorities but often expressed to friends and family at great cost to all concerned.
Although I have some of those thoughts and feelings, I mostly feel a great tension between a deep and somewhat detached fascination with the big picture and the sense of urgency I habitually feel in spring to get fully cranking with the seasonal garden and generally keeping our home at Melliodora shipshape. I feel like I finally have a box seat to watch the train of techno-industrial civilization hitting the Limits to Growth stone wall and breaking apart, all in slow motion.
The rapidly evolving situation and all its psychological, sociological and economic dimensions suggest an expanding field of possibilities. These could include:
- a cyber pandemic that crashes the global financial system,
- a short war between China and the USA4Part of my ‘A History from the Future’ story happening in 2022
- rapid reduction in consumption of oil and other critical resources and consequently greenhouse gas emissions as a result of the virus,
- plus of course accelerating climate disasters.
In different scenarios, concern about the virus and the ability to implement the plan could become ever more intense, or alternatively, be shunted offstage or metastasised into dealing with the next crisis. Consequently, the details of what worked, what didn’t, who takes the credit and who gets the blame, would probably all be lost in the swirling muddy waters of compounding crises.
A personal view of the pandemic
Up until this point, I have not indicated my personal interpretation of either the virus or the response because I wanted to focus on the bigger systemic drivers without getting muddied in the good/bad, right/wrong, us/them polarities. However we all have to face what life throws in our path with whatever internal and collective resources we have at hand. As is my lifelong habit, I have done my own ‘due diligence’ to understand and guide my personal decisions. In the past I have always been open about my conclusions and decisions, whether around the campfire or on the most public of forums. I have often joked about the comfort I feel in being a dissident about most things including being beaten up at primary school in the early days of the Vietnam war for being a ‘commie traitor’ to being ostracised in the 1990s for opposing the ‘war on weeds’ orthodoxy of the environmental mainstream. But today being a dissident is no joking matter. Unfortunately the psychosocial environment has now become so toxic that the pressures to self-censor have become much more complex and powerful. Much more is at stake than personal emotions, ego, reputation or opportunities and penalties.
Following my instinct for transparency, I will state my position, which has been evolving since I first started to consider whether the novel virus in Wuhan might lead to a repeat of the 1919 flu pandemic or even something on the scale of the Black Death. I can summarise my current position and beliefs as follows:
- The virus is real, novel and kills mostly aged, ill and obese people with symptoms both similar to and different from related corona viruses.
- It most likely is a result of ‘Gain of Function’ research at Wuhan Institute of Virology in China supported by funding from the US government.
- Escape rather than release was the more likely start of the pandemic.
- Vaccines in use in western world countries are based on novel technology developed over many years, but without resulting in effective or safe vaccines previously.
- The fear about the virus generated by the official response and media propaganda is out of proportion to the impact of the disease.
- Effective treatment protocols for Covid-19 exist and if those are implemented early in the disease, then hospitalisation and deaths can be greatly reduced, as achieved in some countries that faced severe impacts (especially Mexico and India).
- The socioeconomic and psychosocial impacts of the response will cause more deaths than the virus has so far, especially in poor countries.
- The efficacy of vaccines is falling while reported adverse effects are now much greater proportionally than for previous vaccines.
- The under-reporting of adverse events is also much higher than for previous vaccines, although this is still an open question.
- The possibility of antibody dependent enhancement (ADE) leading to higher morbidity and death in the future is a serious concern and could be unfolding already in countries such as Israel where early and high rates of vaccination have occurred.
Given the toxic nature of views already expressed about (and by) people I know and respect, I am not going to engage in an extensive collating of evidence, referencing who I think are reliable experts and intermediaries who can interpret the virus, the vaccine or any of the related parts of the puzzle. Outsourcing personal responsibility for due diligence to authorities is a risky strategy at the best of times; in times of challenge and rapid change the risks escalate. I do not want to convince anyone to not have the vaccine, but I do want to provide solidarity with those struggling (often alone and isolated) to find answers, so the following are two starting points that I think could be helpful:
- For those trying to understand the vaccines, their efficacy and risks, ‘This interview could save your life: a conversation with Dr Peter McCulloch’ provides a good overview with full reference to official data, scientific papers and clinical experience.
- For those focused on treatment options, the Front Line COVID-19 Critical Care Alliance (FLCCA) physicians are a good source on this rapidly emerging field of clinical practise.
As a healthy 66-year-old I am not personally afraid of the virus, but if greater virulence and death rate do emerge with new variants, I might consider the preventative regimen recommended by the FLCCA doctors. There is no way I will be getting any of the current vaccines in the foreseeable future, no matter what the sanctions and demonisation of my position on this matter.
At this point there may be readers who decide to ignore anything and everything I have written as obviously deluded. These are the costs of transparency.
Valuing the Marginal
Tolerance, let alone celebration of diversity, is not the easy permaculture principle many of us assume. Valuing the marginal can be even harder, especially if we study the darker periods of human history.
Over most of history, minority ethnicities and subcultures lived in ambiguous complementarity with dominant majorities. For hundreds, if not a thousand, years my Jewish ancestors made valuable contributions to European culture while managing to maintain their own culture to an extraordinary extent. They lived in ghettos not just for protection from the eruptions of intolerance in the dominant Christian communities but to ensure their language and culture wasn’t swamped by that of the majority. While the Jews carried the elitist belief that they were God’s Chosen People, they didn’t attempt to gain converts and were naturally respectful to the majority Christians. They survived through all but the worst of antisemitic pogroms by not antagonising the majority, largely accepting the restrictions placed on them by society. What else could they do?
Similar dynamics could emerge from the virus and the vaccine, where a subculture of home birth, home education, home food production and alternative health brings together people of previously diverse subcultures, including permies, who are excluded from society. That exclusion will seem self-inflicted to the majority, but for those excluded it will feel critical to both survival and identity.
Is it sensible to plead for tolerance in line with sensitivities to the rights of other minorities? Or is that just an invitation to be stoned to death, if not literally then virtually, on social media?
Unfortunately one of the weaknesses of western culture, which shows up in both Christian and Muslim traditions, is the idea that if a particular path is the correct one, then everyone should follow it. From the perspective of east Asian philosophy and many Indigenous traditions, harmonious balance is more important than the right way. The yin yang symbol showing each polarity containing the seed of its opposite encapsulates this critically important antidote to the recurring western theme about the triumph of good over evil. In The Patterning Instinct Jeremy Lent explores how these different world views have shaped history and that any emergent ecological world view will foreground the importance of harmonious balance.
The wisdom of the collective
I want to lead by example in trying to understand and articulate why it is good that the majority of the population appears to be strongly behind the official plan and that maybe it is even good that a majority of my permaculture colleagues might be lining up to get vaccinated, when I have no intention of doing so.
Firstly, I acknowledge the obvious reason that if the official story is right, the majority getting vaccinated will combine with naturally acquired immunity and control the worst effects of the virus without the need to get every last dissenter vaccinated.
Secondly, given the pressure to push the vaccination rate in every way possible, encouraging some extra hesitators to resist will only increase the pressure and possibly lead to harsher sanctions as well as more broken family relationships, reputations, pain and suffering, which could be worse than potential adverse effects of the virus, or the vaccine, on those people.
Thirdly, because so many people I respect as intelligent and ethical are following the plan, I won’t fall into the trap of losing respect for who they are, what they have done and what else they might do in the future. And if it turns out this is the start of a more permanent hard fascist command state, then we need people of good values on the inside to keep open whatever channels of communication remain possible.
As systems unravel, the stories that make sense of the world also fall apart and in the desperate search for mental lifeboats, different stories come to the fore. The mainstream story around the pandemic is one such mental lifeboat that allows people to maintain faith and function. Without the renewed source of faith and order from rational science guiding technological wizardry, the psychosocial shock from a pandemic could be enough to create social, economic and political chaos on a historically unprecedented scale, at least in long-affluent countries like Australia.
Whatever the nature of the next crisis, I think it will require citizens to by and large accept that the behaviours, rights and freedoms we took for granted are artifacts of a vanishing world. Further, it will provide a harsh reality check on how dependent most of us are on systems we have no control over, so most will find they have little choice but to accept the new state of affairs.
While I might resent what I see as unnecessary sanctions on those resisting, I accept than in the early stage of Brown Tech energy descent, harsh and by some perspectives, arbitrary, controls on behaviour will be part of our reality and are arguably necessary to maintain some sort of social order (even if short-sighted or not sustainable in the long run). My aim is to focus on how we ameliorate the adverse effects of a predicament that humanity cannot escape.
More philosophically, the virus and the response to it could be seen as a meditation practise showing us how no one is an island separated from the whole of life. To break down the toxic notion that we are free agents to do as we choose without consideration of consequences, especially for future generations and the wider community of life, is something permaculture teaching has tried to bring to daily life. How we do this in meaningful ways is a constant challenge.
Sympathy for the devil
Having at least had a go at seeing the good in the mainstream plan, I now want to articulate quite passionately why the majority should at least tolerate and not seek to further punish the minority for their resistance. To advocate for this within the permaculture movement, I appeal to our pluralism in celebrating the diversity of action. This is especially where permies take the risk of being the unvaccinated guinea pigs, who can at least be a control group in this grand experiment on the human family. Beyond that, I hope our colleagues inside the tent will see the need to express solidarity with our right to chart our own course and not feel they have to be silent for fear of being cast out of the tent.
While I respect the younger permaculture folk following the plan for the common good, I still believe the most creative deep adaptations to the Brown Tech world will be crafted at the geographic and conceptual fringes by younger risk takers coming together in new communities of hope. While the paths to the armoured centre and the feral fringes both have their risks, those on the inside, especially older people, should accept that the young risk takers on the fringes might create pathways though the evolutionary bottleneck of energy descent more effectively than the best resourced and rationally devised plans from within the system of thinking that has created the civilisation crises.
Whether or not the pandemic will lead to the flowering of creative light-footed models for adaptation, the larger energy descent crisis for which permaculture was originally designed (that most permies recognise as the ‘Climate Emergency’) needs these responses at the margins. If the permaculture movement cannot digest this basic truth and at least defend the right of people to craft their own pathways in response to collapse of all certainties, then our movement will have failed the first great test of its relevance in a world of energy descent.
Some permie dissidents will double down in their focus on preparation to survive and thrive in spite of the sanctions, while others will be energised by non-violent direct action to resist what they see as draconian and counterproductive collective punishment. In doing so they may draw on past experience, or inspiration, from the frontlines of anti-war, environmental defence and free communication resistance.
In the past, more apolitical permies trying to introduce permaculture to socially conservative punters could still acknowledge, at least privately, the element of truth in the quip ‘permaculture is revolution disguised as gardening’. In today’s climate, can permies inside the tent accept and appreciate their colleagues on the frontlines of a new resistance movement that might moderate the extremes of how society navigates the larger climate emergency? Or will they flip and decide permaculture was, after all, mostly hippy nonsense now further contaminated with toxic right wing conspiracy madness, so must be dumped as unfit for purpose in our new world?
In saying this, I’m not suggesting we should all follow suit, let alone belittle or demonise those who don’t take the walk on the wild side. That would also be a contradiction of permaculture ethics and design principles. As we have always taught, ethics and design principles are universal but rarely lead to clear and conclusive solutions. Strategies and techniques vary with the context; wonderful elegant design solutions for one context can be hopeless white elephants, or worse, in another. Context is everything and as colleague Dan Palmer has so effectively applied in his Living Design Process, the people context is as complex, subtle and diverse as that of the land and nature.
The sovereignty of persons to choose freely how they grapple with the tension between autonomy and the needs of the commonwealth is not just an ideal from western Enlightenment civilisation working out how to apply the gift of fossil fuel wealth. It is a fundamental expression of how the ecology of context is constantly shifting, and that all systems simultaneously express life through bottom-up autonomy of action and top-down guidance of collective wisdom.
In times of great stability, the distilled wisdom of the collective, embodied in institutions, carries human culture for the long run. Sometimes the sanctions on the individuals who rejected the rules of the collective were harsh and, according to modern thinking, arbitrary but over long periods of relative stability, those rules kept society working. In times of challenge and change it is, ironically, dissidents at the fringes who salvage and conserve some of the truths of the dying culture into the unknown future to craft new patterns of recombinant culture.
What we call ‘science’ had its origins in what Pythagoras salvaged, almost single handedly, from the decadent and corrupt theocracies of ancient Egypt of which he was an initiate, before he walked away from the centre to the margins of civilisation. Major failures in the application of so-called trusted science have been a feature of our lived experience. Tragically, science could be one of the casualties as humanity passes through the cultural evolution bottleneck of climate chaos and energy descent. Permaculture was one attempt to craft a holistic applied design science grounded in observation and interaction, taking personal responsibility and accepting (negative) feedback, designing from patterns to details, and creatively using and responding to change. I still believe that salvaged and retrofitted versions of practical science crafted at the margins will serve humanity better than rigid faith in the priests of arcane specialised knowledge maintained by an empire of extraction and exploitation. Can we be sure what the father of science and mathematics would do in this time of turmoil?
Whatever the historical significance of these times, maintaining connections across differences of understanding and action within permaculture and kindred networks will strengthen us all in dealing with the unfolding challenges and opportunities of the energy descent future.
David Holmgren
Melliodora
September 2021

Vincent van Gogh The red tree house 1890
The FDA. the U.S. Food and Drug Administration, announced on Monday that it gave full approval to a vaccine. But it didn’t. Or rather, it did, but the approval is for a vaccine that doesn’t exist. Or rather, it exists, but it’s not being produced. Or rather, it’s being produced, but under different names and with different legal statuses.
The FDA is playing a game with Americans, in order to get them to submit to being vaccinated. And this has to stop. No more. The role of the FDA is to protect people, not cajole them into politically desired but illegal actions. Below are 3 -bullet points of- articles about the (non-) approval. One from Peter Doshi, senior editor at The BMJ, and a powerful foe to the FDA, one from Robert Kennedy jr, and one from Jill Malone, wife of Dr. Robert Malone.
But first, yet another lie -BIG, not noble- from Anthony Fauci, as told to Anderson Cooper. There is no approval for “the Pfizer product”, and Fauci knows that very well. Or rather, there is approval for a Pfizer product that is not available to anyone. And that should never have been approved the way it was in the first place, but that’s another story. Still, Fauci said it.
In theory, if he were called on it (but of course he won’t be by any reporter he talks to), he could say that the products are the same anyway. But he won’t say that, because he realizes full well that they have different legal statuses; they are “legally distinct” in the words of the FDA. So Fauci can’t say they are the same. Even if it’s just a matter of a different label on a vial.
Yes, it sounds crazy, but that’s the legal labyrinth the FDA and Pfizer have negotiated themselves into. Why? Kennedy says it best: Pfizer is unlikely to allow any American to take a Comirnaty vaccine until it can somehow arrange immunity for this product..
And: “If it says “Comirnaty,” it’s a licensed product. If it says “Pfizer-BioNTech,” it’s an experimental product, and under 21 U.S. Code 360bbb, you have the right to refuse. If it comes from Moderna or Johnson & Johnson (marketed as Janssen), you have the right to refuse. [..] If it doesn’t say Comirnaty, you have not been offered an approved vaccine.”
Jill Malone: The vaccine that is likely to be supplied for some time, WILL BE THE Pfizer – EUA vaccine. So any mandates based on full approval are meaningless.
Fauci Dismisses “Freedom” In Call For Vaccine Mandates: “The Time Has Come. Enough Is Enough.”
“There was some poll that showed about 30% of people who are not anti-vax, they were just waiting to get what they felt was the real final stamp of approval, which we just got today with the Pfizer product.” He continued, “And those 30% are saying when that occurs, they will feel very, very comfortable about getting vaccinated. So right away, you’re talking about 30%. I hope they come through with what the survey said.”
[..] “They’re going to give a lot of incentive and backing for a lot of institutions and organizations and places of employment to mandate, and that could be colleges, university, the military, organizations that employ a lot of people, some of the big corporations are going to say if you want to work for us in person, you’ve got to be there and get vaccinated.”
[..] “I know I respect people’s freedom, but when you’re talking about a public health crisis that we’ve been going through for well over a year and a half, the time has come. Enough is enough. We’ve just got to get people vaccinated.” “If we keep lingering without getting those people vaccinated that should be vaccinated, this thing could linger on, leading to the development of another variant which could complicate things.”
Here’s Peter Doshi, senior editor at The BMJ.
Does The FDA Think These Data Justify The First Full Approval Of A Covid-19 Vaccine?
On 28 July 2021, Pfizer and BioNTech posted updated results for their ongoing phase 3 covid-19 vaccine trial. The preprint came almost a year to the day after the historical trial commenced, and nearly four months since the companies announced vaccine efficacy estimates “up to six months.” But you won’t find 10 month follow-up data here.
While the preprint is new, the results it contains aren’t particularly up to date. In fact, the paper is based on the same data cut-off date (13 March 2021) as the 1 April press release, and its topline efficacy result is identical: 91.3% (95% CI 89.0 to 93.2) vaccine efficacy against symptomatic covid-19 through “up to six months of follow-up.”
[..] the recent reports from Israel’s Ministry of Health caught my eye. In early July, they reported that efficacy against infection and symptomatic disease “fell to 64%.” By late July it had fallen to 39% where Delta is the dominant strain. This is very low. For context, the FDA’s expectation is of “at least 50%” efficacy for any approvable vaccine.
_
[..] evidence of waning immunity was already visible in the data by the 13 March 2021 data cut-off… And it’s hard to imagine how the Delta variant could play a real role here, for 77% of trial participants were from the United States, where Delta was not established until months after data cut-off.
[..] Despite the reference to “six month safety and efficacy” in the preprint’s title, the paper only reports on vaccine efficacy “up to six months,” but not from six months. This is not semantics, as it turns out only 7% of trial participants actually reached six months of blinded follow-up (“8% of BNT162b2 recipients and 6% of placebo recipients had ≥6 months follow-up post-dose 2.”) So despite this preprint appearing a year after the trial began, it provides no data on vaccine efficacy past six months, which is the period Israel says vaccine efficacy has dropped to 39%.
[..] —a total of three covid-19 related deaths (one on vaccine, two on placebo). There were 29 total deaths during blinded follow-up (15 in the vaccine arm; 14 in placebo). The crucial question, however, is whether the waning efficacy seen in the primary endpoint data also applies to the vaccine’s efficacy against severe disease.
_
[..] here we are, with FDA reportedly on the verge of granting a marketing license 13 months into the still ongoing, two year pivotal trial, with no reported data past 13 March 2021, unclear efficacy after six months due to unblinding, evidence of waning protection irrespective of the Delta variant, and limited reporting of safety data.
Robert F. Kennedy, Jr. and Meryl Nass, M.D. at childrenshealthdefense.org.
2 Things Mainstream Media Didn’t Tell You About FDA’s Approval of Pfizer Vaccine
Monday, the U.S. Food and Drug Administration (FDA) approved a biologics license application for the Pfizer Comirnaty vaccine. The press reported that vaccine mandates are now legal for military, healthcare workers, college students and employees in many industries. New York City Mayor Bill de Blasio has now required the vaccine for all teachers and school staff. The Pentagon is proceeding with its mandate for all military service members.
[..] First, the FDA acknowledges that while Pfizer has “insufficient stocks” of the newly licensed Comirnaty vaccine available, there is “a significant amount” of the Pfizer-BioNTech COVID vaccine — produced under Emergency Use Authorization (EUA) — still available for use. The FDA decrees that the Pfizer-BioNTech vaccine under the EUA should remain unlicensed but can be used “interchangeably” (page 2, footnote 8) with the newly licensed Comirnaty product. Second, the FDA pointed out that the licensed Pfizer Comirnaty vaccine and the existing, EUA Pfizer vaccine are “legally distinct,” but proclaims that their differences do not “impact safety or effectiveness.”
[..] EUA products are experimental under U.S. law. Both the Nuremberg Code and federal regulations provide that no one can force a human being to participate in this experiment. Under 21 U.S. Code Sec.360bbb-3(e)(1)(A)(ii)(III), “authorization for medical products for use in emergencies,” it is unlawful to deny someone a job or an education because they refuse to be an experimental subject. Instead, potential recipients have an absolute right to refuse EUA vaccines.
_
U.S. laws, however, permit employers and schools to require students and workers to take licensed vaccines. EUA-approved COVID vaccines have an extraordinary liability shield under the 2005 Public Readiness and Preparedness Act. [..] At least for the moment, the Pfizer Comirnaty vaccine has no liability shield. Vials of the branded product, which say “Comirnaty” on the label, are subject to the same product liability laws as other U.S. products.
When the Centers for Disease Control and Prevention’s (CDC) Advisory Committee for Immunization Practices places a vaccine on the mandatory schedule, a childhood vaccine benefits from a generous retinue of liability protections. But licensed adult vaccines, including the new Comirnaty, do not enjoy any liability shield. Just as with Ford’s exploding Pinto, or Monsanto’s herbicide Roundup, people injured by the Comirnaty vaccine could potentially sue for damages. And because adults injured by the vaccine will be able to show that the manufacturer knew of the problems with the product, jury awards could be astronomical.
Pfizer is therefore unlikely to allow any American to take a Comirnaty vaccine until it can somehow arrange immunity for this product.
[..] the FDA’s acknowledgement in its approval letter that there are insufficient stocks of the licensed Comirnaty, but an abundant supply of the EUA Pfizer BioNTech jab, exposes the “approval” as a cynical scheme to encourage businesses and schools to impose illegal jab mandates. The FDA’s clear motivation is to enable Pfizer to quickly unload inventories of a vaccine that science and the Vaccine Adverse Events Reporting System have exposed as unreasonably dangerous, and that the Delta variant has rendered obsolete.
Americans, told that the Pfizer COVID vaccine is now licensed, will understandably assume COVID vaccine mandates are lawful. But only EUA-authorized vaccines, for which no one has any real liability, will be available during the next few weeks when many school mandate deadlines occur. [..] While the media has trumpeted that the FDA has approved COVID vaccines, the FDA has not approved the Pfizer BioNTech vaccines, nor any COVID vaccines for the 12- to 15-year age group, nor any booster doses for anyone.
And the FDA has not licensed any Moderna vaccine, nor any vaccine from Johnson & Johnson — so the vast majority, if not all, of vaccines available in the U.S. remain unlicensed EUA products.
_
Here’s what you need to know when somebody orders you to get the vaccine: Ask to see the vial. If it says “Comirnaty,” it’s a licensed product. If it says “Pfizer-BioNTech,” it’s an experimental product, and under 21 U.S. Code 360bbb, you have the right to refuse. If it comes from Moderna or Johnson & Johnson (marketed as Janssen), you have the right to refuse. The FDA is playing bait and switch with the American public — but we don’t have to play along. If it doesn’t say Comirnaty, you have not been offered an approved vaccine..
And Jill Malone.
FDA Pfizer Authorization (Comirnaty): Key Points To Consider And Discuss
FDA Pfizer authorization (Comirnaty): Key points to consider and discuss.
These points are an aggregate of many minds, including Dr. Robert Malone. 23 Aug 2021
General talking points
• Why mandates if herd immunity isn’t possible?
• What happens 8 months after boosters?
• What’s the plan for the next variant?
• Why we’re messing with vaccine injury liability if the vaccines are safe and effective?There are now TWO LEGALLY distinct (Pfizer vs. BionTech), but otherwise identical products, based on two FDA letters, as well as a press release. The analysis of these FDA products below is preliminary and subject to change.
Letter to Pfizer
https://www.fda.gov/media/150386/download
• DOES NOT GIVE FULL APPROVAL
• Extends EUA to allow supply of current Pfizer under EUA because limited supply of BioNTech version.
• “The products are legally distinct with certain differences that do not impact safety or effectiveness. (page 2, Pfizer letter) [..] here FDA quietly admits that the licensed Pfizer vaccine and the authorized Pfizer vaccine are identical with regard to safety/efficacy, but they are “legally distinct.” That’s code for one has manufacturer liability, while the other doesn’t. It is also code for “we don’t want to impose a mandate on the EUA product cause it is illegal, but we can probably get away with a mandate on the licensed product.”_
[..] yes, we licensed the vaccine, but…there is a lot of the old vaccine out there, actually “a significant amount” and this amount will be considered an EUA and will continue to be used. Now, why would they do that? Why specify that identical versions of the product will be legally different? Because they need the license to impose the mandates. But they need the EUA to evade liability.
Along with the license comes liability for the manufacturer. (While all EUA products were given a liability shield.) the feds want us to THINK the vaccine we are receiving is licensed, which will make people submit because they think it can now be mandated , but instead we are almost certain to receive the EUA vials instead, to save Pfizer’s behind.
Press release
https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine“On August 23, 2021, FDA approved the biologics license application (BLA) submitted by BioNTech Manufacturing GmbH for COMIRNATY (COVID-19 Vaccine, mRNA) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older.” The efficacy claims are based on outdated data. The press release indicates that the basis of the efficacy claims was as quoted below. However, those data are outdated, and captured with strains of virus (Alpha, Beta) that are no longer predominant. The efficacy claims are therefore invalid – it is quite clear that the vaccine is much less effective in preventing infection by the currently circulating strain (Delta)
In its letter to BioNTech, the FDA states “” We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis. Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.” The first sentence says that VAERS will be incapable of assessing known serious risk The second sentence says that the other pharmacovigilance systems that by law FDA employs (supposedly about 20 different databases when they were bragging about them last October) are similarly incapable of assessing known serious risk.
• The risks in pregnancy remain unknown. “although not FDA requirements, the company has committed to additional post-marketing safety studies, including conducting a pregnancy registry study to evaluate pregnancy and infant outcomes after receipt of Comirnaty during pregnancy.” The prescribing info says: “There is a pregnancy exposure registry for COMIRNATY. Encourage individuals exposed to COMIRNATY around the time of conception or during pregnancy to register by visiting https://mothertobaby.org/ongoingstudy/covid19-vaccines/ .” WHY ARE THEY DOING A PREGNANCY STUDY?
FDA has licensed the BioNTech vaccine for 16 and up
• All of the authorized vaccine on shelves and in freezers will remain only authorized, until the new product with Cominaty labelling arrives.
• 3d or booster doses and vaccine for 12-15 year olds remains under EUA
• Why not also approve the Pfizer version? Why leave it under EUA?
• When the press says the “Pfizer vaccine is fully approved.” It is not. The vaccine that is likely to be supplied for some time, WILL BE THE Pfizer – EUA vaccine. So any mandates based on full approval are meaningless.THE BLA acknowledges LONG term myocardial issues with a 5 year follow up consistent with the lower range for LTFU for Gene Therapy Products. Is FDA quietly acknowledging the Gene Therapy classification? These products have been classified by FDA as Gene Therapy Products which require UP to 15 years long term follow up in studies. This was acknowledged by Moderna in their 2Q 2020 filing.
_
Using superior CDC published methods, normalizing for people vaccinated, Children’s Health Defense estimates 176x reports of VAERS deaths associated with C19 vaccines compared with flu vaccines. 35x the number for H1N1 (where stimulated reporting is speculated) Using CDC published methods we estimate under-reporting of VAERS deaths to be 5- 15x. for a total of 30,000-90,000 deaths, mostly non-C19. Underreporting for lifethreatening events may be 24-64x. IN ADDITION – (Israel MOH, combined with Dagan study), we have estimated between 35-86,000 EXCESS USA deaths due to Covid in those vaccinated (>=1 dose)

Background Reports of waning vaccine-induced immunity against COVID-19 have begun to surface. With that, the comparable long-term protection conferred by previous infection with SARS-CoV-2 remains unclear.
Methods
We conducted a retrospective observational study comparing three groups:
(1) SARS-CoV-2-naïve individuals who received a two-dose regimen of the BioNTech/Pfizer mRNA BNT162b2 vaccine,
(2) previously infected individuals who have not been vaccinated, and (3)previously infected and single dose vaccinated individuals. Three multivariate logistic regression models were applied. In all models we evaluated four outcomes: SARS-CoV-2 infection, symptomatic disease, COVID-19-related hospitalization and death. The follow-up period of June 1 to August 14, 2021, when the Delta variant was dominant in Israel.
Results
SARS-CoV-2-naïve vaccinees had a 13.06-fold (95% CI, 8.08 to 21.11) increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021. The increased risk was significant ( P <0.001) for symptomatic disease as well. When allowing the infection to occur at any time before vaccination (from March 2020 to February 2021), evidence of waning natural immunity was demonstrated, though SARS-CoV-2 naïve vaccinees had a 5.96-fold (95% CI, 4.85 to 7.33) increased risk for breakthrough infection and a 7.13-fold (95% CI, 5.51 to 9.21) increased risk for symptomatic disease. SARS-CoV-2-naïve vaccinees were also at a greater risk for COVID-19-related-hospitalizations compared to those that were previously infected.
Conclusions
This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.

The World Economic Forum estimates that the Covid response has cost the globe $11 trillion thus far and counting and AIER’s seminal analysis of the costs (mental health costs, hunger and poverty costs, direct economic costs, unemployment costs, educational costs, healthcare costs, and crime costs etc.), places the Covid ‘emergency’ in a sobering light. It reveals the devastating and crushing collateral damage from the unnecessary lockdowns, school closures, and masking and mask mandates that will impact the rest of the 21st century by some estimates. These harms have damaged the poorer class among us in a perverse and brutal manner. They destroyed businesses, destroyed employees who were sent home, destroyed lives, and destroyed the lives of children who committed suicide.
Yet the elites are far removed from the ramifications of their nonsensical, illogical, specious policies and edicts. Dictates that do not apply to them or their families or friends. The ‘laptop’ affluent class could vacate, work remotely, walk their dogs and pets, catch up on reading their books, and do tasks they could not do had they been in the workplace daily. They could hire extra teachers for their children etc. Remote working was a boon. The actions of our governments however, devastated and long-term hurt the poor in societies and terribly and perversely so, and many could not hold on and committed suicide. AIER’s Ethan Yang’s analysis showed that deaths of despair skyrocketed. Poor children, especially in richer western nations such as the US and Canada, self-harmed and ended their lives, not due to the pandemic virus, but due to the lockdowns and school closures. Many children took their own lives out of despair, depression, and hopelessness due to the lockdowns and school closures.
Our core position since the start of the Covid-19 response in February 2020 (and which remains fixed for how the US, Canada, UK, Australia, Caribbean nations, European nations, and all other global nations must presently respond to the Delta variant/mutation) is that we do not lock the society down or close schools or impose mask mandates, etc. These policies did not apply to this emergency and certainly not after the first 3 to 4 weeks or so. This applies just as much for the initial Wuhan variant and now for the Covid-19 Delta variant or any other variant to come, if the variant is not one with an extremely high level of lethality, as was presumed erroneously for the initial Wuhan variant. In fact, even with respect to the initial variant it became clear very early on in the pandemic that it was probably no more lethal than annual influenza, yet we persisted with draconian devastating lockdown policies that only served to harm the people. These restrictive policies worked to ruin and kill (direct and indirect) more persons than SARS-CoV-2 itself.
It is why leading infectious diseases experts especially with regards to pandemics (such as Dr. Donald Henderson of Johns Hopkins) never supported the non-pharmacological measures noted above, as they knew that such policies would be catastrophic; even for more lethal pathogens (see AIER).
“As experience shows, there is no basis for recommending quarantine either of groups or individuals. The problems in implementing such measures are formidable, and secondary effects of absenteeism and community disruption as well as possible adverse consequences, such as loss of public trust in government and stigmatization of quarantined people and groups, are likely to be considerable.”
None of these restrictive policy measures such as lockdowns and school closures have worked in the past for Covid-19 and they will not work now with this media-driven hysteria over the Delta variant. If reimposed, they will once again cause crushing harms and deaths due to the collateral effects.
The leaders in public health and government spokespersons as well as the corrupted media are quickly progressing towards endorsing and implementing and registering of individuals under the guise of a public health emergency. That our Governments are even considering the issuance of what have become known as Covid-19 ‘vaccine passports’ is very troubling on many levels. The very idea is anathema to our democratic principles and rights that are enshrined in the US Constitution.
The vaccine passports are being considered and/or introduced by various government bodies which will constrain the rights of citizens under the questionable guise of safety. These passports are simply unjustifiable on any grounds, not the least of which is the fact that SARS-CoV-2 is no more deadly on a population level than influenza. Ostensibly, the passports are designed to allow individuals to partake in everyday commerce and “life” with freedom.
There is even talk of immunity passports also known as ‘antibody passports’ with the concept of antibodies as a “declaration of immunity” or “golden passport” so as to return to routine work and travel. Yet, it is well known that insofar as immunity passports are concerned, antibody levels in people who’ve either had Covid-19, or have been vaccinated, wane after weeks to months.
Hence even someone who should be completely eligible not only for a vaccine passport but in fact an ‘immunity’ passport would easily fail the tests required to obtain such a passport. We and others argue that such will drive the development of a heretofore unheard of (in the USA and Canada) caste system of the haves (have vaccine passports) and the have nots (don’t have vaccine passports). Liew stated “the introduction of immunity passports is beset with challenges, not least of which is the potential erosion of civil liberties, as travelers are stratified into the ‘immunoprivileged’ and the ‘immuno-deprived.’
Experts have argued that the introduction of vaccine and/or immunization (antibody) passports must entail extensive debate that considers all of the moral, ethical and constitutional issues, including “a comprehensive assessment of benefits and harms, and what would least restrict individual liberties without significantly heightening the threat of Covid-19.”
The ACLU has weighed in, sounding warnings that there are many harms that can arise with the introduction of vaccine passports, particularly the digitization of relevant information associated with the granting of those passports. The ACLU stated, “Given the enormous difficulty of creating a digital passport system, and the compromises and failures that are likely to happen along the way, we are wary about the side effects and long-term consequences it could have.”
Now our concerns look to the future for more variants that will most assuredly emerge more efficiently than the Delta variant. Refocusing on the lockdowns, these restrictions are options of last resort as mentioned above (see Henderson, 2006, Disease Mitigation Measures in the Control of Pandemic Influenza). This basic principle applied to the first variant of SARS-CoV-2 and even more so to the Delta variant which appears to be the weakest, most nonconsequential of all the variants as can be computed based on data obtained in the UK and Israel (and other data). The emergence of the Delta variant is quite simply not a new Covid-19, nor was the Alpha (original) variant and sadly as a consequence of the draconian measures we’ve discussed, societies were decimated needlessly. There is now evidence out of Israel that the booster shot (3rd shot) is also met with emergent infections.
We were fantastically misled by the media and experts who doled out misinformation related to Covid-19 and the lockdowns and we were driven into a life of fear. This really is and was a pandemic of fear, of ignorance, and of hysteria. It continues to be so, underpinned by a corrupted biased media. This is ‘panic porn’ driven by a craven inept media, and the corrupt public health officials who are using the Delta variant (soon another e.g. Lambda or Epsilon), to drive further fear. We wonder if it is pure incompetence or unabashed unbridled bias and corruption?
The fact is that we knew very early on that Covid-19 was amenable to risk stratification that predicted outcome, especially with regard to severity and mortality. We know that an age-risk ‘focused’ (Great Barrington Declaration) and ‘targeted’ approach was the critical and only meaningful approach that should have been used. Then and now.
We argue and hold that these lockdown strategies have devastated the most vulnerable among us – the poor – who are now worse off. Lockdowns have hit the African-American, Latino, and South Asian communities devastatingly and have decimated developing nations. Lockdowns have made poor persons even poorer. Lockdowns and especially the extended ones have been deeply destructive and there was absolutely no reason to ever quarantine those up to 70 years old. There was no reason to test or quarantine asymptomatic individuals. And in relation to the testing of ‘asymptomatic’ people we can point to the subtle nature of the creation of an environment of fear. The mere use of the word ‘asymptomatic’ implies that everyone being tested is sick! They are not! They are healthy people! Why would we ever do mass testing for viral or other pathogens in healthy people? Readily accessible data showed consistently that there was near 100% probability of survival from Covid for those 70 and under (99.95%). Therefore, we strongly secure and safeguard the elderly as our core approach, while the young and healthiest among us should be ‘allowed’ to live their lives without fear. This was and is our position as we argued and continue to argue for a ‘focused’ and ‘targeted’ approach based on risk. We continue to suggest a similar approach for the Delta variant, based on the UK and Israel data (and other emerging data) and all other nonlethal variants yet to emerge.
This is not heresy. It is classic biology and modern public health medicine! As mentioned, those in the low to no risk categories must live reasonably normal lives with sensible common-sense precautions (while providing strong safeguards to the high-risk persons and vulnerable elderly). With strong protections of the high-risk among us and the use of early treatment as needed (for those infected will be in a better position to clear the virus and be then ‘naturally immune post early treatment), we can close off this pandemic emergency.
So, what do we know about Delta?
The good news is that Delta is so far proving to be the mildest form of Covid-19 as the mutations have focused on the Spike protein and in and around the gain-of-function furin cleavage joint, which causes the virus to be less dangerous.
This is great news, as those who have natural immunity will be immune to Delta, though we are seeing some breakthrough cases in those vaccinated.
Unfortunately, across the last 17 to 18 months, we chose to ignore the signals from the pandemic and instead we chose to focus on the noise to address Covid-19. We instead harmed our societies and especially our children!
We knew early on and ignored it, that Covid-19 was amenable to risk stratification and that your baseline risk was prognostic on your subsequent outcome, e.g. mortality. We had strong early evidence that a focused approach based on age and risk stratification was more optimal but disregarded this. The fact remains that age and excess body weight/obesity, have accounted for almost 80 to 85% of the hospitalizations, intubations/ventilation, severe sequelae, and deaths in Covid-19. Many persons who have died in nations such as the US have been overweight with some level of obesity. The importance of educating the public on the risk factors and the need for such protective efforts can be enhanced by the people themselves. Had public health leaders used their platforms optimally, the geared messaging would have helped reduce the damage significantly. We could have cut deaths significantly had the options described above been used, especially early outpatient treatment.
Understanding Covid-19 must therefore not involve the traditional unidimensional, dogmatic orthodoxy whereby we simply wish to control the spread of the virus or eradicate it. It remains an impossibility to eradicate a viral pathogen, especially if it is highly mutable like the flu virus. We as humanity have learned to live with such viruses. It is likely that Covid-19 will become the 5th ‘common cold’ coronavirus (if it isn’t already) and be with us for decades, in a mild, mainly nonlethal form, and will exhibit a seasonal pattern. Indeed, we have almost zero concerns about the common cold, and yet, the common cold is responsible for many deaths in the elderly or those with compromised immune systems. We will learn to live with it as we have for other pathogens, e.g. common cold, seasonal influenza etc., and we argue that this latest Delta variant is the step toward this largely ‘benign’ relationship with humans. At the same time, whenever there is a pathogen that is causing some level of illness, there is usually a greater severity and adverse sequelae in the lower SES populations (socioeconomically disadvantaged populations). We must therefore look at this consequence and consider a more nuanced and finessed approach to pathology, as we address targeting the pathogen. We can learn from this public health debacle created through wilful ignorance and the near criminal merging politics with medicine and not repeat the mistakes.
Where did we go so wrong with these lockdowns and school closures? The stark reality is that the Covid-inspired forced lockdowns on business and school closures are and have been counterproductive, were not sustainable and were, quite frankly, meritless, unscientific and may have caused more harm through forcing individuals into enclosed spaces. These unparalleled public health actions were enacted for a virus with an infection mortality rate (IFR) roughly similar to seasonal influenza. Stanford’s John P.A. Ioannidis identified 36 studies (43 estimates) along with an additional 7 preliminary national estimates (50 pieces of data) and concluded that among people <70 years old across the world, infection fatality rates ranged from 0.00% to 0.57% with a median of 0.05% across the different global locations (with a corrected median of 0.04%).
What is the conclusion after 17 to 18 months of Covid-19 (February 2020 to July 2021) in terms of the utility of societal lockdowns and school closures? What does the new evidence across the past year and a half add? What can we say based on the sum of the evidence to date? Have our positions changed on lockdowns and school closures as to the merits? We can state conclusively, after 17 months, that lockdowns and school closures were a catastrophic failure in every sense of the word! With careful examination of all available studies, reports, and documents that are judged of quality enough to inform this thesis, we can find not one instance, (not one!) across the entire globe whereby societal or setting lockdowns or school closures conferred any benefit in curbing the spread of Covid virus or reducing deaths. In fact, we find the contrary, whereby lockdowns and school closures were devastating and particularly on the poorer in society, benefitting the laptop ‘café latte’ class and decimating the underprivileged class.
What was incredible across the 17 months was that governments and their scientific advisors were not satisfied with the well-documented failures of lockdowns. None!
In terms of the evidence, what do we have to offer across 17 months now to support our argument against lockdowns, school closures, and masking (mask mandates)? Well, none of these measures have worked and will work. We offer:
i) in terms of lockdowns, based on our deep study, we found out about the catastrophic harms (consequences), threat, dehumanization, and failures of lockdowns and sheltering/shielding (including prolonged lockdowns) (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88).
As an example, a very recent study in Nature by Jani looked at the effectiveness of this sheltering/shielding (lockdown), by linking family practitioner, prescribing, laboratory, hospital and death records and comparing Covid-19 outcomes among shielded and unshielded individuals in the West of Scotland. Researchers reported that of the 1.3 million population, 27,747 (2.03%) were advised to shield, and 353,085 (26.85%) were classified a priori as moderate risk. They found that by using the reference group as the low-risk group and when compared to this group, “the shielded group had higher confirmed infections (RR 8.45, 95% 7.44–9.59), case-fatality (RR 5.62, 95% CI 4.47–7.07) and population mortality (RR 57.56, 95% 44.06–75.19). The moderate-risk had intermediate confirmed infections (RR 4.11, 95% CI 3.82–4.42) and population mortality (RR 25.41, 95% CI 20.36–31.71) but, due to their higher prevalence, made the largest contribution to deaths (PAF 75.30%). Age ≥ 70 years accounted for 49.55% of deaths. In conclusion, in spite of the shielding strategy, high risk individuals were at increased risk of death.”
We found how pronounced the devastation was on the poorer in society, shifting the burden onto them. The richer among us could even tend to their gardens and walk their pets and order in meals while setting up private tutors for their children and teaching pods, etc. The less affluent had to scramble to find sources of internet, laptops and webcams for their children.
Micheal Peterson puts a face to this picture and said it best when he discussed the low savings of such underdeveloped nations and particularly the populations “in general, high domestic savings rates tend to lead to higher economic growth rates. Unfortunately, since developing countries typically have lower domestic savings, it’s much harder for those countries to weather lockdowns because individuals are unable to draw upon savings to compensate for lost income. For many developed nations, domestic savings is higher, which means that these countries will fare relatively better when income is severely reduced or altogether nonexistent,” due to the lockdowns and as such, shuttered businesses and as such, lost jobs.
A revealing statistic emerges in a World Bank working paper in which it was estimated that “approximately 1 in 5 jobs can be performed remotely in the developed world. In developing countries, this figure stands at only 1 in 26.” Here exactly is where the divide resides and where we failed to look and take into consideration. It is here that many poorer nations and settings were further ‘hollowed out’ by the often unsound and unscientific and as we argue, crushing, costly, illogical, and needless lockdowns and school closures.
ii) in terms of school closures and also based on our deep study and update of the evidence since our last Op-ed, we continue to conclude that there was and is no sound justification for school closures given the exceedingly low (statistically zero) risk to children and very low risk to schoolteachers (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56). Children do not acquire the infection readily (including Delta variant), spread it, or take it home. More particularly, children are at a near statistically zero risk of getting severely ill from Covid or dying from it; again, this includes the Delta variant. We have found no data or evidence to suggest otherwise, despite the hysteria presently running 24/7 in the daily media and by the statements of the lead public health officials. We urge them to provide the nation and us the evidence that backs up anything they report on the Delta variant, for we can find none.
iii) We also know of the ineffectiveness of masks (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41). We know of the failure of mask mandates (references 1, 2, 3, 4, 5, 6, 7, 8).
More specifically on masking evidence, a particularly important seminal research study by the CDC published in Emerging Infectious Diseases (EID) in May 2020 and looking at nonpharmaceutical measures for pandemic influenza in nonhealthcare settings (personal protective and environmental measures using 10 RCTs), found that use of masks did not reduce the rate of laboratory-proven infections with the respiratory influenza virus. “In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks”.
Similarly, a strong argument against the use of masks in the current Covid-19 pandemic gained traction when a recent CDC case-control study reported that well over 80% of cases always or often wore masks. This CDC study further called into question the utility of masks in the Covid-19 emergency. This CDC study showed that the majority of persons infected wore face masks, and still got infected.
Just look no further than the study out of Sweden by Jonas Ludvigsson on Covid transmission with no lockdowns or mask mandates in children. In terms of masking children which we are vehemently against (in school or out of school) Ludvigsson powerfully evidenced the low risk in children by publishing this seminal paper in the New England Journal of Medicine among children one to 16 years of age and their teachers in Sweden. From the nearly 2 million children that were followed in school in Sweden, it was reported that with no mask mandates, there were zero deaths from Covid and a few instances of transmission and minimal hospitalization.
What about the high-quality randomized controlled trial Danish Study published in the Annals of Internal Medicine that sought to assess whether recommending surgical mask utilization outside of the home would help reduce the wearer’s risks of acquiring SARS-CoV-2 infection in a setting where masks were uncommon and not among recommended public health measures. This can be regarded as the highest quality study on the effectiveness of Covid masks. The sample included a total of 3,030 participants who were assigned randomly to wear masks, and 2,994 who were told to not wear masks (i.e. the control arm). The authors concluded that there was no statistically or clinically significant impact of mask use in regard to the rate of infection with SARS-CoV-2.
Perhaps one of the most seminal and rigorous studies (along with the Danish study published in the Annals of Internal Medicine) emerged from a United States Marine Corps study performed in an isolated location; Parris Island. As reported in a recent NEJM publication (CHARM study), researchers studied SARS-CoV-2 transmission among Marine recruits during quarantine. Marine recruits at Parris Island (n=1,848 of 3,143 eligible recruits) who volunteered underwent a 2-week quarantine at home that was followed by a 2nd 2-week quarantine in a closed college campus setting.
iv) we even know of the harms due to mask use (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32).
Overall, the research evidence alluded to here (including a summary by Ethan Yang) suggests that lockdowns and school closures do not (and definitely did not) lead to lower mortality or case numbers and have not worked as intended. Lockdowns have not slowed or stopped the spread of SARS-CoV-2.
Some critics of our position will point to data that ostensibly shows that the implementation of lockdowns led to reduced rates of death. However, these conclusions are based on artifactual and superfluous assessments. We know that declines in death were taking place even before lockdowns came into effect. In fact, in Europe, it was shown that in most cases, mortality rates were already 50% lower than peak rates by the time lockdowns were instituted, thus making claims that lockdowns were effective in reducing mortality spurious at best. Of course, this also means that the presumptive positive effects of lockdowns were and have been exaggerated grossly. Evidence shows that nations and settings that apply less stringent social distancing measures and lockdowns experience the same evolution (e.g. deaths per million) of the epidemic as those that apply far more stringent regulations.
What does this all mean?
These misguided policies have eroded the public trust. These policies include: 1) a flawed PCR test with cycle count thresholds that only pick up noninfectious fragments of viral mRNA; a Ct of 40 means one is noninfectious and nonlethal. 2) Asymptomatic spread 3) Recurrent infection 4) Equal risk of severe outcome if infected 5) No preventative or therapeutics available 6) We were not already partially immune; maybe as high as 80% (some level of immunity against SARS 2) 7) Social distancing of 6 feet prevents spread. 8) Mass testing asymptomatic persons 9) Quarantine asymptomatic persons 10) Children spread the virus and at risk of severe illness 11) Masks are effective against viral illnesses 12) Natural immunity was inferior to vaccine-induced immunity and 13) Evolutionary pressure towards virulence is caused by unvaccinated people.
Future generations will bear the cost of these decisions. Our children and younger people are going to be burdened with the indirect but very real harms and costs of lockdowns for a generation to come. Lives are being ruined and lost and businesses are being destroyed forever. Lower-income Americans, Canadians, and other global citizens are much more likely to be compelled to work in unsafe conditions. These are employees with the least bargaining power, tending to be minority, female, and hourly paid employees. Moreover, Covid-19 has revealed itself as a disease of disparity and poverty. This means that black and minority communities are disproportionately affected by the pandemic itself and they take a double hit, being additionally and disproportionately ravaged by the effects of the restrictive policies.
We do not need to drastically alter our society, the lives of our people, our economies, or our school systems to handle Covid and any variant that emerges. We are well capable of managing this with early treatment and properly securing the elderly and high-risk among us.
It is disheartening as to why governments, whose primary role is to protect their citizens, took these punitive actions despite the compelling evidence that these policies were misdirected and very harmful, causing palpable harm to human welfare on so many levels. It’s questionable what governments did (and now threaten to redo) to their populations with no scientific basis. None! In this, we lost our civil liberties and essential rights, all based on spurious ‘science’ or worse including, opinion, speculation, supposition, and whimsy. They just refused to listen, refused to read the data and science, and were blinded to it. Their ‘academically sloppy’ thinking and actions cost lives, and thousands of lives were cut short by their nonsensical and often irrational shutdown and closure policies.
We are hearing discussions now about renewed lockdowns and masking etc. due to the Delta variant which has emerged as one of the weakest in terms of lethality while being very transmissible. This greatly concerns us. We are horrified by this prospect and we have shown you the actual data as it relates to Delta, and not the contrived drivel and unscientific nonsense spouted by the mainstream media and the public health experts. There is absolutely no good reason to reenter lockdowns and school closures or masking in response to the Delta variant. We find no evidence that this variant warrants masks in children. We leave you with the words of Donald Henderson:
“Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.”
Contributing Authors
- Paul E Alexander MSc PhD, McMaster University and GUIDE Research Methods Group, Hamilton, Ontario, Canada [email protected]
- Howard C. Tenenbaum DDS, Dip. Perio., PhD, FRCD(C) Centre for Advanced Dental Research and Care, Mount Sinai Hospital, and Faculties of Medicine and Dentistry, University of Toronto, Toronto, ON, Canada [email protected]
- Dr. Parvez Dara, MD, MBA, [email protected]
- Liesel Marie Alexander, MBA
[

![]()
Print](# "Printer Friendly, PDF & Email")
Paul E. Alexander

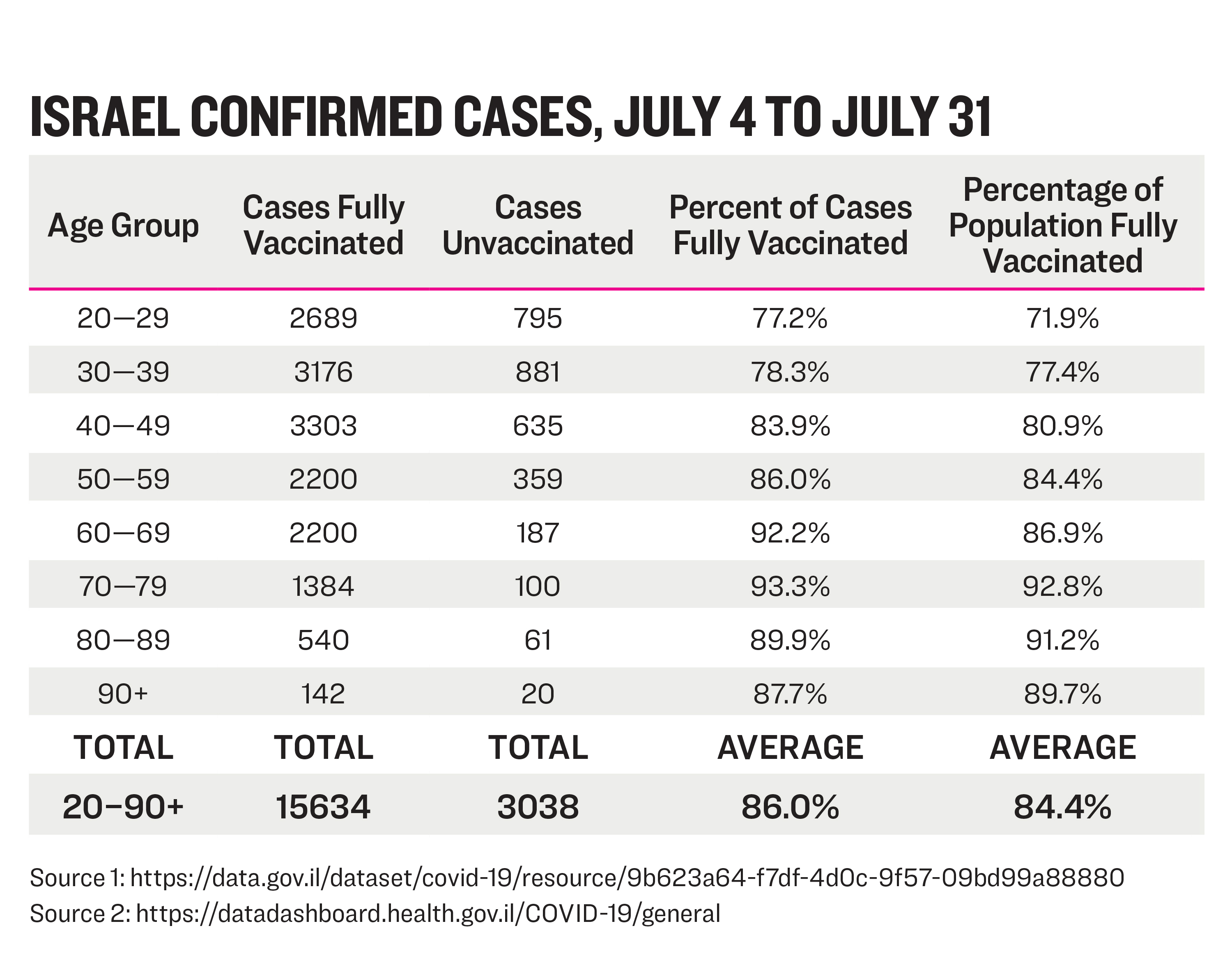{kind=link}

Paul E. Alexander received his bachelor’s degree in epidemiology from McMaster University in Hamilton, Ontario, a master’s degree from Oxford University, and a PhD from McMaster University’s Department of Health Research Methods, Evidence, and Impact.