Monthly Shaarli
July, 2021

Alexandria, VA — Daniel Everette Hale, a former Air Force intelligence analyst who pleaded guilty to sharing classified documents about US Military drone programs with a reporter was just sentenced to 45 months in Federal Prison. Ahead of his sentencing Hale’s lawyers submitted an 11-page letter handwritten by Daniel from his jail cell to US District Judge Liam O’Grady. Hale’s deeply personal letter paints a gruesome picture of the US Drone Program, and explains in detail how it was a crisis of conscience that led Hale to leak secrets about the program to a reporter.
Below is Daniel Everette Hale’s letter to Judge Liam O’Grady in its entirety:
Dear Judge O’Grady,

Former Air Force intelligence analyst Daniel Everette Hale, 2012
It is not a secret that I struggle to live with depression and post traumatic stress disorder. Both stem from my childhood experience growing up in a rural mountain community and were compounded by exposure to combat during military service. Depression is a constant. Though stress, particularly stress caused by war, can manifest itself at different times and in different ways. The tell-tale signs of a person afflicted by PTSD and depression can often be outwardly observed and are practically universally recognizable. Hard lines about the face and jaw. Eyes, once bright and wide, now deepset and fearful. And an inexplicably sudden loss of interest in things that used to spark joy. These are the noticeable changes in my demeanor marked by those who knew me before and after military service. To say that the period of my life spent serving in the United States Air Force had an impression on me would be an understatement. It is more accurate to say that it irreversibly transformed my identity as an American. Having forever altered the thread of my life’s story, weaved into the fabric of our nation’s history. To better appreciate the significance of how this came to pass, I would like to explain my experience deployed to Afghanistan as it was in 2012 and how it is I came to violate the Espionage Act, as a result.
In my capacity as a signals intelligence analyst stationed at Bagram Airbase, I was made to track down the geographic location of handset cellphone devices believed to be in the possession of so-called enemy combatants. To accomplish this mission required access to a complex chain of globe-spanning satellites capable of maintaining an unbroken connection with remotely piloted aircraft, commonly referred to as drones. Once a steady connection is made and a targeted cell phone device is acquired, an imagery analyst in the U.S., in coordination with a drone pilot and camera operator, would take over using information I provided to surveil everything that occurred within the drone’s field of vision. This was done, most often, to document the day-to-day lives of suspected militants. Sometimes, under the right conditions, an attempt at capture would be made. Other times, a decision to strike and kill them where they stood would be weighed.
Daniel Hale’s deeply personal letter paints a gruesome picture of the US Drone Program, and explains in detail how it was a crisis of conscience that led him to leak secrets about the program to a reporter.
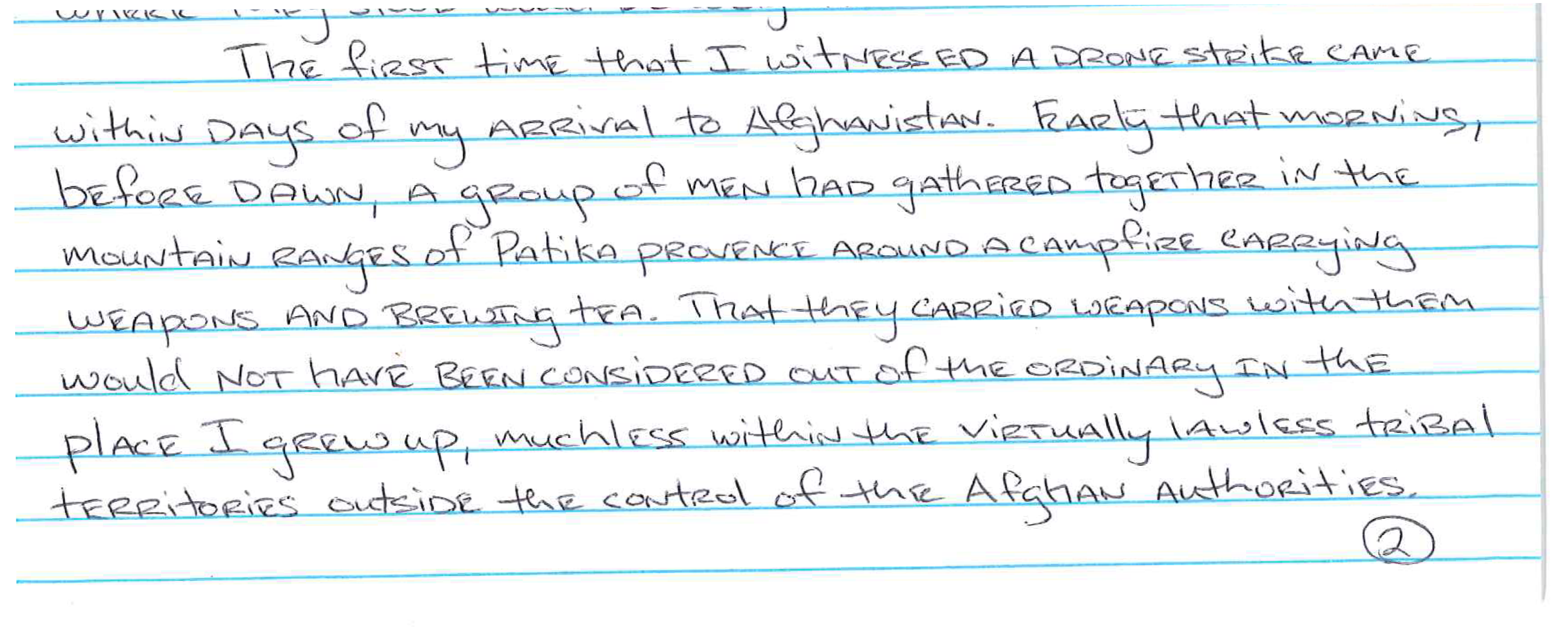
The first time that I witnessed a drone strike came within days of my arrival to Afghanistan. Early that morning, before dawn, a group of men had gathered together in the mountain ranges of Patika provence around a campfire carrying weapons and brewing tea. That they carried weapons with them would not have been considered out of the ordinary in the place I grew up, muchless within the virtually lawless tribal territories outside the control of the Afghan authorities. Except that among them was a suspected member of the Taliban, given away by the targeted cell phone device in his pocket. As for the remaining individuals, to be armed, of military age, and sitting in the presence of an alleged enemy combatant was enough evidence to place them under suspicion as well. Despite having peacefully assembled, posing no threat, the fate of the now tea drinking men had all but been fulfilled. I could only look on as I sat by and watched through a computer monitor when a sudden, terrifying flurry of hellfire missiles came crashing down, splattering purple-colored crystal guts on the side of the morning mountain.
Since that time and to this day, I continue to recall several such scenes of graphic violence carried out from the cold comfort of a computer chair. Not a day goes by that I don’t question the justification for my actions. By the rules of engagement, it may have been permissible for me to have helped to kill those men—whose language I did not speak, customs I did not understand, and crimes I could not identify—in the gruesome manner that I did. Watch them die. But how could it be considered honorable of me to continuously have laid in wait for the next opportunity to kill unsuspecting persons, who, more often than not, are posing no danger to me or any other person at the time. Nevermind honorable, how could it be that any thinking person continued to believe that it was necessary for the protection of the United States of America to be in Afghanistan and killing people, not one of whom present was responsible for the September 11th attacks on our nation. Notwithstanding, in 2012, a full year after the demise of Osama bin Laden in Pakistan, I was a part of killing misguided young men who were but mere children on the day of 9/11.
Nevertheless, in spite of my better instincts, I continued to follow orders and obey my command for fear of repercussion. Yet, all the while, becoming increasingly aware that the war had very little to do with preventing terror from coming into the United States and a lot more to do with protecting the profits of weapons manufacturers and so-called defense contractors. The evidence of this fact was laid bare all around me. In the longest or most technologically advanced war in American history, contract mercenaries outnumbered uniform wearing soldiers 2 to 1 and earned as much as 10 times their salary. Meanwhile, it did not matter whether it was, as I had seen, an Afghan farmer blown in half, yet miraculously conscious and pointlessly trying to scoop his insides off the ground, or whether it was an American flag-draped coffin lowered into Arlington National Cemetery to the sound of a 21-gun salute. Bang, bang, bang. Both served to justify the easy flow of capital at the cost of blood—theirs and ours. When I think about this I am grief-stricken and ashamed of myself for the things I’ve done to support it.
The most harrowing day of my life came months into my deployment to Afghanistan when a routine surveillance mission turned into disaster. For weeks we had been tracking the movements of a ring of car bomb manufacturers living around Jalalabad. Car bombs directed at US bases had become an increasingly frequent and deadly problem that summer, so much effort was put into stopping them. It was a windy and clouded afternoon when one of the suspects had been discovered headed eastbound, driving at a high rate of speed. This alarmed my superiors who believe he might be attempting to escape across the border into Pakistan.

A US drone strike on a civilian vehicle believed to be carrying a Taliban leader in Afghanistan
A drone strike was our only chance and already it began lining up to take the shot. But the less advanced predator drone found it difficult to see through clouds and compete against strong headwinds. The single payload MQ-1 failed to connect with its target, instead missing by a few meters. The vehicle, damaged, but still driveable, continued on ahead after narrowly avoiding destruction. Eventually, once the concern of another incoming missile subsided, the driver stopped, got out of the car, and checked himself as though he could not believe he was still alive. Out of the passenger side came a woman wearing an unmistakable burka. As astounding as it was to have just learned there had been a woman, possibly his wife, there with the man we intended to kill moments ago, I did not have the chance to see what happened next before the drone diverted its camera when she began frantically to pull out something from the back of the car.
A couple of days passed before I finally learned from a briefing by my commanding officer about what took place. There indeed had been the suspect’s wife with him in the car. And in the back were their two young daughters, ages 5 and 3 years old. A cadre of Afghan soldiers were sent to investigate where the car had stopped the following day. It was there they found them placed in the dumpster nearby. The eldest was found dead due to unspecified wounds caused by shrapnel that pierced her body. Her younger sister was alive but severely dehydrated. As my commanding officer relayed this information to us she seemed to express disgust, not for the fact that we had errantly fired on a man and his family, having killed one of his daughters; but for the suspected bomb maker having ordered his wife to dump the bodies of their daughters in the trash, so that the two of them could more quickly escape across the border. Now, whenever I encounter an individual who thinks that drone warfare is justified and reliably keeps America safe, I remember that time and ask myself how could I possibly continue to believe that I am a good person, deserving of my life and the right to pursue happiness.
One year later, at a farewell gathering for those of us who would soon be leaving military service, I sat alone, transfixed by the television, while others reminisced together. On television was breaking news of the president giving his first public remarks about the policy surrounding the use of drone technology in warfare. His remarks were made to reassure the public of reports scrutinizing the death of civilians in drone strikes and the targeting of American citizens. The president said that a high standard of “near certainty” needed to be met in order to ensure that no civilians were present. But from what I knew, of the instances where civilians plausibly could have been present, those killed were nearly always designated enemies killed in action unless proven otherwise. Nonetheless, I continued to heed his words as the president went on to explain how a drone could be used to eliminate someone who posed an “imminent threat” to the United States. Using the analogy of taking out a sniper, with his sights set on an unassuming crowd of people, the president likened the use of drones to prevent a would-be terrorist from carrying out his evil plot. But, as I understood it to be, the unassuming crowd had been those who lived in fear and the terror of drones in their skies and the sniper in this scenario had been me. I came to believe that the policy of drone assasiniation was being used to mislead the public that it keeps us safe, and when I finally left the military, still processing what I’d been a part of, I began to speak out, believing my participation in the drone program to have been deeply wrong.
I dedicated myself to anti-war activism, and was asked to partake in a peace conference in Washington, DC late November, 2013. People had come together from around the world to share experiences about what it is like living in the age of drones. Fazil bin Ali Jaber had journeyed from Yemen to tell us of what happened to his brother Salem bin Ali Jaber and their cousin Waleed. Waleed had been a policeman and Salem was a well-respected firebrand Imam, known for giving sermons to young men about the path towards destruction should they choose to take up violent jihad.
A US drone strike on a civilian vehicle, similar to the harrowing incident described by Fazil
One day in August 2012, local members of Al Qaeda traveling through Fazil’s village in a car spotted Salem in the shade, pulled up towards him, and beckoned him to come over and speak to them. Not one to miss an opportunity to evangelize to the youth, Salem proceeded cautiously with Waleed by his side. Fazil and other villagers began looking on from afar. Farther still was an ever present reaper drone looking too.
As Fazil recounted what happened next, I felt myself transported back in time to where I had been on that day, 2012. Unbeknownst to Fazil and those of his village at the time was that they had not been the only watching Salem approach the jihadist in the car. From Afghanistan, I and everyone on duty paused their work to witness the carnage that was about to unfold. At the press of a button from thousands of miles away, two hellfire missiles screeched out of the sky, followed by two more. Showing no signs of remorse, I, and those around me, clapped and cheered triumphantly. In front of a speechless auditorium, Fazil wept.
About a week after the peace conference I received a lucrative job offer if I were to come back to work as a government contractor. I felt uneasy about the idea. Up to that point, my only plan post military separation had been to enroll in college to complete my degree. But the money I could make was by far more than I had ever made before; in fact, it was more than any of my college-educated friends were making. So, after giving it careful consideration, I delayed going to school for a semester and took the job.
For a long time I was uncomfortable with myself over the thought of taking advantage of my military background to land a cushy desk job. During that time I was still processing what I had been through and I was starting to wonder if I was contributing again to the problem of money and war by accepting to return as a defense contractor. Worse was my growing apprehension that everyone around me was also taking part in a collective delusion and denial that was used to justify our exorbitant salaries, for comparatively easy labor. The thing I feared most at the time was the temptation not to question it.
Then it came to be that one day after work I stuck around to socialize with a pair of co-workers whose talented work I had come to greatly admire. They made me feel welcomed, and I was happy to have earned their approval. But then, to my dismay, our brand-new friendship took an unexpectedly dark turn. They elected that we should take a moment and view together some archived footage of past drone strikes. Such bonding ceremonies around a computer to watch so-called “war porn” had not been new to me. I partook in them all the time while deployed to Afghanistan. But on that day, years after the fact, my new friends gaped and sneered, just as my old one’s had, at the sight of faceless men in the final moments of their lives. I sat by watching too; said nothing and felt my heart breaking into pieces.

Daniel Everette Hale and Leila, December 2020
Your Honor, the truest truism that I’ve come to understand about the nature of war is that war is trauma. I believe that any person either called-upon or coerced to participate in war against their fellow man is promised to be exposed to some form of trauma. In that way, no soldier blessed to have returned home from war does so uninjured. The crux of PTSD is that it is a moral conundrum that afflicts invisible wounds on the psyche of a person made to burden the weight of experience after surviving a traumatic event. How PTSD manifests depends on the circumstances of the event. So how is the drone operator to process this? The victorious rifleman, unquestioningly remorseful, at least keeps his honor intact by having faced off against his enemy on the battlefield. The determined fighter pilot has the luxury of not having to witness the gruesome aftermath. But what possibly could I have done to cope with the undeniable cruelties that I perpetuated?
My conscience, once held at bay, came roaring back to life. At first, I tried to ignore it. Wishing instead that someone, better placed than I, should come along to take this cup from me. But this too was folly. Left to decide whether to act, I only could do that which I ought to do before God and my own conscience. The answer came to me, that to stop the cycle of violence, I ought to sacrifice my own life and not that of another person.
So, I contacted an investigative reporter, with whom I had had an established prior relationship, and told him that I had something the American people needed to know.
Respectfully,
**Daniel Hale**

Raminder Mulla
In the Hindu tradition, there are four stages to life.
One of learning how to be a citizen, one of householding, where one works and contributes to their community. Then comes retired life in which one starts to withdraw from the world. There then comes a state of renunciation, where one abandons all worldly possessions and spends all their time in spiritual practice.
These stages seem a reasonable way to conduct a life, and honour the flow of nature.
Time and energy are invested in our young, that they may grow into people capable of nourishing and sustaining the world around them as socialised adults. Over time, their power to give reduces, until there is only the self left to give. Even this, will wither in time. This is true of all living things.
Over time, my desire to give, as a householder, has waned. Now I desire retirement and renunciation. My ability to give is leaving me.
Dear Society,
It’s time for us to part. We’ve both changed and I don’t think we can be together anymore. When we first met, you were huge, radiant, so full of promise. I still remember the words you said to me; It didn’t matter that you said them to so many others.
’If you work hard, be kind, and look after others, then life will be good. I will look after you.’
For quite a while, you did and everything was good. I worked hard in our younger days in the hope that all that I learned could be used to for you. So much of it was for you. I even tried to bring some new knowledge into the world, since I thought you’d rather like that. It sounded like you did, but actions speak louder than words, and I could always feel your gaze drifting to that one in the corner with the sharp suit and a tongue to match, who often told you he’d like to chop you up and sell bits of you back to yourself.
I suppose that should have been a red flag.
Why stick around when that’s what you want?
I suppose, I thought I could change you.
I used to think lovers who thought they could change their partner were insane. Perhaps I’m insane myself. I tried to put everything into you once again. Played by your rules and respected your boundaries. You didn’t do the same. This, I can’t forgive. You decided that what I wanted simply didn’t matter, despite our promises.
It’s become all about you. Not about us.
You told me who I could and could not see. I went along with it, after all, your friends told me you were under a lot of stress. That it would only be a few weeks and would really help you. Fine, I suppose we all need to compromise once in a while. Then it started getting really strange. You started talking about amputating bits of yourself and casting them aside. It looked like you already tried, with the many self-inflicted cuts and grazes I saw you with one night.
You said to me: ’My limbs would grow back,’ and that ’they weren’t essential.’ Remember that? Maybe I should have left then, or at least tried to get you some help. Plenty of people make it through such dark thoughts.
Your friends told me that all of this talk of breaking yourself apart was necessary, that you weren’t safe without doing this and would build back better. Ultimately, you hadn’t fallen in on yourself yet. In sickness and in health, after all. I could ignore it for a while. I have my friends too, and while they didn’t all agree on how to deal with you, many of them told me to be patient. Others told me I was being hysterical.
Can never really know what to do, can you? One of the tragedies of our shared life is that the people we both know don’t really want to tell the truth. It’s too much responsibility.
Love is patient, love is kind. It does not envy, it does not boast, it is not proud. It does not dishonour others, it is not self-seeking, it is not easily angered, it keeps no record of wrongs.”
1 Corinthians 13:4-8
Summer came and things calmed down. We could think about a future together, years, decades ahead. You told me you learned from your mistakes. When I asked someone wise about that, he wasn’t so sure.
Winter followed and then you obsessed over yourself again. You muttered the same phrases over and over. Kept asking me where I was going, and what I was doing. You asked me to treat our children as vermin. To stab and suffocate them for you – for your own protection, you said.
Why?
Why, did you keep picking at your scars and scabs, over and over and over again?
Your friends told me that this time, it was my fault. They pointed at me, and called me selfish. Evil. That I ought to get over myself. If I did as I was told, you’d be back to who you once were. How could I be to blame? All I ever did was love you.
Finally came the needles. How often did we lament those we lost along the way to addiction, putting things they had no idea about into themselves in the hope they might escape reality for a few moments? How tragic it was that they resorted to the syringe, the bottle, the pills, the pipe, just to be OK? Why did you think you would escape their fate? Why so many needles into yourself and into your friends too? Why our children?
After all we talked about, why try to drag me into it? Misery needing company?
You told me, if I loved you, I’d take the needle. For a moment there, you had me. I needed you that much. Now, you’ve decided you don’t want anything to do with those who don’t shoot up, I suppose we’re done. We never were a two-way street, were we?
I see you now in the cold light of day, and I don’t know you anymore. You were once strong and kept your promises. You helped me and I helped you. You listened to those who had hard truths to tell and learned from them.
Now, you are withered, starved and addicted. So many pieces of you that once shone are missing. Lost forever. The light has gone from your eyes. You look only for control over others, and use your friends in your games. You hate those who aren’t obsessed by the things you are, the needle, the fear, the self-destruction. You do not know love anymore.
You move towards those who wish you ill more than those who love you. I will not watch you decline a moment longer.
I cannot be here.
Goodbye.
Raminder Mulla is a scientist by trade and training. He is also interested in philosophy and creative expression. More of his work can be found on his website.
The naked scientific truth on why the ongoing mass vaccination experiment drives a rapid evolutionary response of SARS-CoV-2
The ongoing denial by WHO, public health agencies and governments of science-based evidence on how to mitigate the already disastrous global and individual consequences of this pandemic are beyond mind-blowing. Whereas a number of medical doctors are now doing the utmost to make highly successful early multidrug treatment broadly accessible, I am contributing my part on analyzing the epidemiologic and health consequences of the ongoing mass vaccination campaigns and sharing - in all transparency - my insights with the broader public. From the critical opinion article below, it becomes already obvious that several scientists who are studying the evolutionary biology and genetic/ molecular epidemiology of this pandemic know too well that this pandemic is not over at all and that the global health risk posed by variants is very substantial. So, why do they keep silent?
I realize that the scientific language is not easily accessible to laymen. I hope the way I structured the article will, however, help them to grasp the key message.
Summary
As Sars-CoV-2 entered a highly susceptible human population, it has initially been spreading rapidly and in an uncontrollable way. This already explains why Sars-CoV-2 has been evolving rather slowly with no substantial selection of fitness-enhancing mutations occurring over the first 10 months of the pandemic (i.e., between December 2019 and October 2020). More infectious ‘variants of concern’ (VoCs, i.e., alpha [B.1.1.7], beta [B.1.351], gamma [P.1]) started to appear as of late 2020 and led to a steep increase in cases worldwide.
Molecular epidemiologists have observed that mutations within the Sars-CoV-2 spike (S) protein of these emerging, more infectious lineages are converging to the same genetic sites, a phenomenon that coincided with a major evolutionary shift in the landscape of naturally selected Sars-CoV-2 mutations (1).
Significant convergent evolution(*) of more infectious circulating Sars-CoV-2 variants is not a neutral, host-independent evolutionary phenomenon that merely results from increased viral replication and transmission but is strongly suggestive of natural selection and adaptation following a dramatic shift in the host(ile) environment the virus is exposed to (1).
Molecular epidemiologists fully acknowledge that the pandemic is currently evolving Sars-CoV-2 variants that “could be a considerably bigger problem for us than any variants that we currently know in that they might have any combinations of increased transmissibility, altered virulence and/or increased capacity to escape population immunity” (1). This is to say that phylogenetics-based natural selection analysis on circulating Sars-CoV-2 lineages strongly suggests that viral variants resistant to spike (S)-based Covid-19 vaccines are currently expanding in prevalence and highly suspicious of causing future epidemic surges globally.
Deployment of current Covid-19 vaccines in mass vaccination campaigns combined with the ongoing widespread circulation of Sars-CoV-2 can only increase immune selective pressure on Sars-CoV-2 spike protein and hence, further drive its adaptive evolution to circumvent vaccine-induced humoral immunity. In this regard, the expectation of an increasing number of vaccinologists matches the current observation made by genomic epidemiologists in that S protein-directed immune escape variants are highly likely to further spread and expedite the occurrence of viral resistance to the currently deployed and future (so-called ‘2nd generation’) Covid-19 vaccines.
To monitor the circulation of hazardous viral variants in the population and to be able to provide unequivocal proof of the immune selection pressure exerted by mass vaccination campaigns and the harmful consequences thereof, there is an urgent need for conducting representative viral sampling on vaccinees, including those who are healthy or only subject to mild disease, and to genetically characterize the variants they shed upon exposure to Sars-CoV-2.
Conducting a mass vaccination experiment at a global scale without understanding the mechanisms underlying viral escape from vaccine-mediated selection pressure is not only a colossal scientific blunder but, first and foremost, completely irresponsible from the perspective of individual and public health ethics.
In the absence of vaccines capable of inducing sterilizing immunity, early multidrug treatment as proposed by Prof. Dr. P. McCullough and others (https://pubmed.ncbi.nlm.nih.gov/33387997/), together with global chemoprophylaxis using highly efficient antiviral drugs, will be key to save lives, reduce the hospitalization burden and dramatically diminish transmission of highly infectious or neutralizing antibody (nAb)-resistant escape variants.
(*) Convergent evolution relates to the independent occurrence of one or more mutations that are shared in common across several viral variants
Preamble
There is currently a lot of confusion in regard of the effectiveness of Covid-19 vaccines with plenty of contradictory reports circulating in the literature and on social media. This in itself is probably providing the most convincing evidence that the pandemic situation is rapidly evolving and is currently transitioning a kind of ‘gray’ zone. A pandemic is typically to be considered a very dynamic event (until it merges into an endemic situation). However, the evolutionary dynamics of this Covid-19 pandemic have now been shaped by human intervention in a way that is completely unprecedented. We do know about the outcome of a natural pandemic but don’t know at all about the outcome of the ongoing pandemic, as the latter has now become a ‘pandemic of variants’. From what follows below (and which is basically a summary of findings made by molecular/ genomic epidemiologists that I put into a broader context), there is however, one certainty, which is that Sars-CoV-2 variants are rapidly evolving in response to the natural immune selection pressure they are experiencing. Phylogenetics-based natural selection analysis indicates that a substantial amount of the immune selection pressure exerted during this pandemic is directed at the Sars-CoV-2 spike (S) protein, which is targeted by the vaccines. On their journey to adapting to the host(ile) environment of neutralizing antibodies (nAbs), variants further exploit their evolutionary capacity to overcome this S-directed, population-level immune pressure. Hence, in a given vaccination setting and stage of the ongoing pandemic, the success of mass vaccination campaigns will to a large extent depend on the evolving prevalence of increasingly problematic variants. Alternatively, S-directed immune interventions that seem effective in one vaccination setting and stage of this pandemic may not work as well when applied to another vaccination setting or when implemented at another stage of the ongoing pandemic. The observation that the effectiveness of mass vaccination campaigns, as assessed during a pandemic of immune escape variants, oftentimes evolves very differently between countries or regions is, therefore, not surprising. It is only when the population-level selective immune pressure will culminate that variants and, therefore, the effects of these campaigns will start to globally converge to the same endpoint, which is ‘resistance’ to the vaccines. It is only at that very endpoint that all assessments of the alleged ‘effectiveness’ of this experiment will be unanimous and consistent. When exactly this will happen is still subject to speculation. However, as the immune selection pressure in the global population is now ‘massively’ rising and the set of naturally selected, S-directed mutations together with the plasticity thereof dramatically expanding, one can reasonably expect that the edition of a super variant capable of resisting S-specific Abs will be precipitated such as to emerge within the next few months. When second-generation vaccines will be introduced, the virus will only be building upon this versatile foundation of circulating mutations to rapidly circumvent the immune pressure the re-vaccinated population will continue to exert on the S protein.
“The most important issue here is not whether this particular “super variant” ever arises….” (1)
It is unbelievable how public health authorities (PHAs) are lagging behind when it comes to understanding the evolutionary capacity of Sars-CoV-2. Or do PHAs and policymakers simply ignore the observations made by world-class molecular epidemiologists? How can they possibly justify mass vaccination campaigns in light of all the scientific arguments pointing to the high likelihood that these campaigns will only expedite viral resistance to Covid-19 vaccines? Why are the scientists who are bringing all this evidence to the PAPER not bringing it to the TABLE? How can they predict that this pandemic is going to evolve even more problematic VoCs and keep silent? Why don’t they set up a forum of independent, knowledgeable experts providing indisputable and unanimously agreed evidence that the rhetoric put forward by the WHO and national health authorities is scientifically wrong? Don’t they realize that keeping silent about the ongoing disastrous - but for now still largely hidden- evolution of the pandemic is only going to provide more ammunition for governments to extend their mass vaccination campaigns such as to reach as high as possible vaccine coverage rates in the population? Why on one hand do molecular epidemiologists seriously consider that resistance to the vaccines may occur as a result of rapidly rising S-directed immune pressure in the population but on the other hand don’t ring the alarm bell? How can they acknowledge the effect of emergent viral variants on the efficacy of Covid-19 vaccines without overtly pointing to the risk that vaccines failing to block viral transmission will further shape the evolution dynamics of viral variants? How can they recognize that antibody(Ab)-based therapy (e.g., use of convalescent plasma and monoclonal Ab treatments) in immunocompromised, chronically ill patients promotes long-term viral shedding and may lead to the propagation of variants carrying Ab escape mutations while ignoring the likelihood for a similar effect to occur when mass vaccination enables an entire population to exert immune selection pressure on the very same immunodominant Sars-CoV-2 S protein (i.e., when large numbers of individuals are vaccinated while being exposed to the virus before having developed a full-fledged Ab response)? It cannot be that they don’t understand the disastrous consequences viral resistance to Covid-19 vaccines would imply! It cannot be either that they didn’t learn that the kinetics of natural selection of immune escape mutations are much slower (or even non-existent as in the case of the Influenza pandemic of 1918!) in the presence of naturally elicited immunity. Or don’t they realize that the type of immune priming following natural Sars-CoV-2 infection is very different from the one that results from prophylactic immunization with S-based vaccines? It is difficult to imagine they would not comprehend why under conditions of natural viral infection and transmission during a pandemic, the chances for freshly infected, immunologically naïve or previously infected subjects to become re-infected on a background of suboptimal S-specific Abs are much lower than for vaccinated people to become exposed to Sars-CoV-2 while not being armed with a high enough titer of full-fledged S-specific Abs.
In other words, if molecular epidemiologists would only realize that immune selection pressure exerted by S-directed Abs occurs much less frequently during a natural pandemic than in the course of mass vaccination campaigns, they would probably figure among the best placed scientists on earth to warn against the high likelihood for this virus to evolve immune evasion and, ultimately, to resist vaccinal nAbs as a result of mass vaccination. At any rate, they all recognize the need for careful systematic surveillance of the ongoing evolutionary immune escape, which currently translates in an enhanced expansion of variants comprising mutations that further converge as they continue to adapt to rising population immunity in general and S-specific Abs in particular (1).
Although population cohorts exerting selective S-directed immune pressure, (i.e., now increasingly consisting of vaccinees!) provide a breeding ground for S-associated immune escape mutations, health authorities seem to no longer be monitoring viral shedding and genetic characterization of viral samples in healthy or only mildly ill vaccinees. This is, of course, highly problematic as even asymptomatically infected vaccinees are known to shed virus and are now granted more freedom of movement and adhering less to social distancing measures. In this way, we are currently largely incognizant of the true prevalence and distribution of new variants and the speed at which they spread in the population. However, epidemiologists are not raising their voice to put an end to this grave public health negligence, even though they clearly seem to disagree with this practice: “As antigenically different variants are continuing to emerge, it will become necessary to routinely collect serum samples from vaccinated individuals and from individuals who have been infected with circulating variants of known sequence” (3); and further: “Defining these dynamics, and their potential influence on vaccine effectiveness, will require large-scale monitoring of SARS-CoV-2 evolution and host immunity for a long time to come” (4).
In the meantime, the WHO and their advising ‘experts’ are still preaching the ludicrous mantra that the more we vaccinate, the less the virus can replicate and hence, the lower the risk that VoCs will arise and become dominant in the viral population. Is it this mantra of mass vaccination that leads PHAs to conclude that monitoring of viral shedding in vaccinees has become obsolete? However, their simplistic interpretation of viral transmission dynamics would only apply to conditions of neutral genetic drift as occurring during the early phase of a pandemic, i.e., in a population of immunologically unprimed susceptible subjects that does not exert significant positive selection pressure on the virus prior to its host-to-host transmission (2). However, at this stage of the pandemic where a multitude of variants, including several VoCs, are already circulating, the real global health concern is no longer about the likelihood for yet another problematic variant to emerge but rather about the ongoing population-level selection pressure that is now driving particular mutations of concern to expand in prevalence. Ignoring the positive selection signals that are now increasingly observed within nAb-binding S domains inevitably leads to an underestimation of the evolutionary potential of Sars-CoV-2 to escape from these nAbs (2). However, instead of investigating the conditions that underlie this strong positive selection pressure, PHAs are doing the utmost to make people believe that mass vaccination will stop the transmission of these variants, lead to herd immunity and, therefore, put a stop to the Covid-19 pandemic. There is currently no single scientific argument or rationale to back any of these statements. On the contrary, numerous reports on breakthrough infections in vaccinees clearly illustrate that those who have not been immunized against Sars-CoV-2 are all but provided indirect protection by vaccinees (5, 14). The mantra that mass vaccination will at least contribute to controlling the pandemic is fully incoherent with the scientific knowledge gathered by molecular epidemiologists. Whereas phylogenetics-based natural selection analysis is a well-established method for studying evolutionary adaptation to enhanced host immune pressure, PHAs don’t seem to be impressed by data that are strongly suggestive of immune selection pressure resulting from human interventions targeting Sars-CoV-2 spike protein. Findings from this analysis indicate that as soon as a certain threshold of infectious pressure is reached, a sufficient number of subjects will harbor dominant mutants that could then spread across the entire population provided positive immune selection pressure is exerted by a substantial part of the population (1).
Some VoCs have already been observed before mass vaccination campaigns were initiated. Because they reproduce more effectively in the population, these antigenically different variants are referred to as ‘more infectious variants’. In order to adapt to the increased pressure exerted by rising population immunity, variants are now increasingly incorporating additional mutations converging to specific sites within the receptor-binding domain (RBD) of the virus and conferring resistance to multiple S-directed Abs (1). The ongoing convergent evolution of immune escape mutations may come with a fitness cost of new variants for as long as the contribution of the population exerting selective immune pressure is not high enough to enable its enhanced propagation in the host population. It is important to note, though, that multiple distinct point mutations can each evade a multitude of neutralizing Abs (2). This would already explain why very few mutations (e.g., within the RBD) could already lead to full resistance to vaccinal Abs. At this stage of the pandemic, mutations in the S protein that impact neutralizing Abs are already present at significant frequencies in the global viral population and evidence of expanding variants exhibiting a higher and higher level of resistance to vaccinal S-specific Abs is now accruing (3). In other words, it becomes increasingly obvious that Sars-CoV-2 immune escape variants are adapting to rising population immunity and improving on transmissibility by stepwise acquisition of new mutations (as shown, for example, by the recent expansion of the delta ‘plus’ variant in several countries). All of the above already explains why the ‘success’ as proclaimed by the WHO and other health authorities or advising experts merely relates to short-term assessments of morbidity, hospitalization and mortality rates. However, the data published by molecular/ genomic epidemiologists analyzing the ongoing adaptation of Sars-CoV-2 to the evolving immune selection forces at play in this pandemic of Sars-CoV-2 variants seem to indicate that the ‘success’ of current public health efforts will not last for much longer. This is because PHAs and their advising experts seem to ignore that mass vaccination campaigns conducted during a pandemic of variants fail to reduce the number of active infections to a level low enough to prevent natural selection of immune escape mutants (i.e., even including double or triple mutants!) and curtail their adaptation to a steadily rising population-level immune selection pressure, no matter the speed at which these campaigns are conducted. Their mantra that the acceleration of mass vaccination campaigns will prevent the virus from evolving variants that escape vaccine-induced immunity is, therefore, simply wrong. Since all of the current Covid-19 vaccines deployed in this mass vaccination program will contribute to raising immune selection pressure and eventually provide variants capable of evading S-specific Abs with a fitness advantage in the population (i.e., increasingly consisting of vaccinees!), neither herd immunity nor eradication could conceivably happen.
In conclusion: There is no way that the ongoing pharmaceutical (mass vaccination) and nonpharmaceutical interventions will prevent propagation of more infectious variants (those got already selected before the initiation of mass vaccination campaigns, presumably as a result of widespread implementation of stringent infection prevention measures) or variants comprising one or more RBD-associated nAb-resistant mutations. On the contrary, all evidence from molecular epidemiology indicates that the ongoing shift in natural selection forces exerted by the population on Sars-CoV-2 mutations is merely going to expedite the selection and propagation of more problematic variants of concern. It is beyond any doubt that growing vaccine coverage rates in the global population will further exploit the evolutionary capacity of Sars-CoV-2 to adapt to a higher and higher S-directed immune selection pressure until full vaccine resistance is achieved.
There is now compelling evidence that sets of convergent mutations that have emerged in the context of VoCs evolved in response to the changing immune profile of the population. It has been postulated that convergent evolution of mutations primarily occurs in previously infected individuals or as a result of chronic infections (15-20). However, vaccinated people are far more prone to breeding viral immune escape variants than non-vaccinated naturally infected individuals. Why?
In immunologically unprimed subjects, the peak of viral replication and shedding occurs well before host Ab responses appear. This already suggests that the host immune response in non-primed, S-sero-negative subjects (i.e., including previously asymptomatically infected subjects who lost their short-lived S-specific Abs) does not exert significant immune pressure on the virus(**). On the other hand, most countries started their vaccination campaigns before a substantial part of the population acquired immunity from natural infection. It is, therefore, reasonable to postulate that not natural infection or transmission but widespread deployment of vaccines is now becoming the primary cause of evolutionary selection pressure on viral expansion. This would already suggest that immune escape variants are now spreading rapidly in many parts of the world. It is fair to assume that the more widespread the presence of vaccinal S-specific Abs in the global population, the more the rate of evolutionary immune evasion from S-directed humoral immune pressure will rise. The frequent occurrence of suboptimal immune selection pressure exerted by virus-exposed vaccinees on Sars-CoV-2 spike protein will provide variants that are capable of evading S-specific vaccinal Abs with a selective transmission advantage. As already mentioned in previous contributions of mine, suboptimal S-directed immune pressure occurs in asymptomatically infected vaccinees who are still in the process of mounting Ab responses or possessing immature S-specific Abs (e.g., between 1st and 2nd injection of a 2-shot vaccine) or whose vaccinal Abs are low in titer and/ or not fully functional as a result of an immune compromised health status.
(**) There are two important exceptions. 1. If the number of active infections is very high (e.g., due to overcrowding and poor hygienic standards), the reservoir of people who are naturally susceptible to Covid-19 disease becomes rapidly exhausted. This will now provide a transmission advantage to more infectious variants harboring immune escape mutations that are capable of withstanding selective S-directed immune pressure exerted by short-lived Abs in previously asymptomatically infected individuals. When the infectious pressure is high, the likelihood for the latter to become re-infected shortly after their primary infection will increase and so will the likelihood of expansion of more infectious variants. 2. Likewise, selective immune pressure will be relevant in case stringent infection prevention measures targeted at controlling the pandemic are installed on a background of a sufficiently high infectious pressure. Under such conditions, viral transmission to naturally susceptible individuals is hampered and a similar type of more infectious variants may gain a transmission advantage when exposed to suboptimal S-specific humoral responses in previously asymptomatically infected individuals.
What determines the time required for Sars-CoV-2 to resist vaccinal Abs at a population level?
It is fair to assume that RBD-targeted immune selection pressure exerted on a background of previously selected mutations enabling enhanced viral infectiousness will expedite natural selection of new, nAb-escaping mutations. Hence, circulation of more infectious viral variants is likely to expedite convergent evolution of mutations, including such that enable viral resistance to S-directed Ab-mediated immunity elicited by the vaccines.
As a rule of thumb, the time for population-level anti-vaccine resistance to develop depends on
-
The transmission or fitness advantage of the nAb-resistant variant (2). This factor is dependent on both, the magnitude of the population-level selection pressure and the intrinsic evolutionary fitness cost. The higher the relative percentage of individuals with nAbs to a given epitope (i.e., the more widely a given epitope is targeted) and the lower the intrinsic evolutionary fitness cost (i.e., the more effective the ‘infectious’ function of the mutated epitope), the higher the transmission advantage of the nAb-resistant variant and hence, the faster the mutated epitope will generate resistance to nAbs that are targeting it. In the case of vaccines, however, resistance will require a combination of multiple RBD-targeted mutations. This is what is currently causing in several countries an insidious period of pandemic quiescence as it takes more time for the virus to acquire a combination of multiple mutations to overcome vaccine-induced immunity despite widespread immune selection pressure (so-called ‘fitness valley-crossing time’; 2). Full resistance to the vaccines can only occur through intermediate steps wherein immune escape variants progressively evolve to incorporate additional mutations that are required to eventually reach full resistance to the vaccine. As long as the acquired subset of mutations does not suffice to escape the population-level immune pressure induced by the vaccine, the overall transmission or fitness cost from the immune escape mutations will be higher than the overall transmission or fitness advantage provided by the selection pressure exerted by the expanding prevalence of nAbs in the population.
-
The mutation rate (2). This factor is dependent on both, the infectious viral pressure and the intrinsic mutability of the virus. The higher the mutation rate, the higher the likelihood that a combinatorial subset of mutations required for full-fledged resistance to the vaccine occurs. Viral variants may even harbor mutations outside of S protein that are subject to natural selection and thereby drive an enhanced mutation rate (21).
Intermediate immune escape variants (i.e., harboring only a subset of the mutations required for nAb escape) are characterized by a lower fitness level. However, fast-speed mass vaccination campaigns that are rolled out on a background of a relatively high infectious pressure will mediate a relatively strong population-level immune selection pressure (as vaccine coverage rates rise quite rapidly). All of this will expedite the evolution of intermediate lower fitness variants into nAb-resistant variants (e.g., USA case). Conversely, when a mass vaccination program is initiated on a background of low infectious pressure, transmission of intermediate lower fitness variants will be low and more time will be required for nAb-resistant mutants to establish in the population (e.g., Israel case). This has been motivating certain ‘experts’ and policymakers to precipitate their conclusions on the success of mass vaccination campaigns in that they pretend that the pandemic is increasingly getting under control!
It is fair to expect that the widespread presence of full-fledged, S-specific vaccinal Abs will eventually cause vaccine-resistant variants to dominate and further expand in the viral population. This is to say that ongoing mass vaccination campaigns will inevitably entail full resistance of Sars-CoV-2 to all S-targeting Covid-19 vaccines and are, therefore, highly likely to lead to an impressive wave of infection and disease in vaccinees, especially in those who have not previously experienced Covid-19 disease.
It suffices to acknowledge that the ongoing convergent evolution of new variants is driven by natural selection pressure to conclude that mass vaccination campaigns conducted in the heat of a pandemic are now promoting expansion of immune escape variants that vaccines will eventually no longer be capable of protecting against.
Whereas global and stringent infection containment measures may eventually have led to population-level selection of more infectious variants, increasing vaccine coverage rates are now likely to promote population-level selection of nAb-evading viral mutants. Viral VoCs that spontaneously arise as a result of viral replication cannot all of a sudden start to outcompete lineages that circulate in several different countries unless they acquire a competitive advantage. They can only acquire such an advantage if the environmental conditions they are exposed to change in ways that provide them with a transmission advantage when compared to the wild-type virus or previously circulating strains/ variants. Because some mutations will endow the virus with enhanced intrinsic viral infectiousness, viral variants comprising such mutations will naturally be selected when altered conditions in the host environment exert pressure on viral infectiousness. In this way, viral propagation and survival can be secured. Provided the selection pressure on viral infectiousness is widespread in the population, more infectious variants will rapidly gain a fitness advantage and quickly expand in the population. Dominance of such new viral variants is, therefore, indicative of natural selection of a virus that is more transmissible at a population level. However, the more the combination of mutations required for immune escape impacts viral fitness, the more time it will take immune escape variants to reach a high enough infectious pressure in the population or the more immune selection pressure will need to be exerted by the host environment to compensate for the incurred evolutionary fitness cost (see also below). Along the same lines of reasoning, it is fair to conclude that more infectious or nAb-resistant variants will expand in prevalence upon their introduction into countries where mass vaccination is already well advanced. These variants are, indeed, well adapted to the widespread immune selection pressure that has been generated in the population as a result of mass vaccination. Thanks to an excellent breeding ground, these variants will now reproduce more effectively than the previously circulating strains.
It is fair to postulate that the more widespread the presence of full-fledged, S-specific vaccinal Abs, the more readily variants will evolve resistance to the vaccines and eventually adapt to the immune environment they are exposed to as they spread in the host population. This is to conclude that ongoing mass vaccination campaigns will inevitably entail full resistance of Sars-CoV-2 to all S-targeting Covid-19 vaccines. This is highly likely to rapidly provoke a resurgence of Sars-CoV-2 infection and disease, especially in vaccinees. As already mentioned above, cases of severe disease would be expected to be more frequent amongt vaccinees who did not previously contract Covid-19 disease.
How can human behavior or infection prevention measures promote propagation of mutations in Sars-CoV-2 spike protein?
The natural host environment of Sars-CoV-2 can create several barriers that impact viral transmissibility and survival. Enactment of infection prevention measures or overcrowding are examples of situations threatening viral spread. As the infectiousness of Sars-CoV-2 is strongly shaped by the physicochemical properties of its spike protein, the above-mentioned obstacles will exert selection pressure on Sars-CoV-2 S protein and may, therefore, substantially contribute to natural selection of mutations that enable stronger binding affinity of S protein for the Ace-2 receptor of permissive cells. To adapt to such environmental constraints, viral variants have been shown to independently evolve to acquire multiple unique as well as convergent mutations (1). Convergent evolution of mutations comprised within S-associated, immunologically relevant genes are proof of natural selection and illustrate the evolutionary capacity of Sars-CoV-2 to adapt to S-targeted immune pressure.
Renowned experts in molecular epidemiology are now increasingly finding that the emergence and ongoing convergent evolution of Sars-CoV-2 variants coincides with a major global shift in the Sars-CoV-2 selective landscape (1). As this ongoing shift also coincides with globally conducted mass vaccination campaigns, the question arises as to whether these ongoing campaigns have the potential to foster convergence between evolving variants. This boils down to the following question:
Does mass vaccination with current Covid-19 vaccines enable populations to exert S-directed immune selection pressure?
This is, indeed, an important question: If mass vaccination enables the vaccinated population-to exert S-directed immune selection pressure, the likelihood that current Covid-19 vaccines will be able to control the pandemic should be seriously questioned for adaptive evolution of Sars-CoV-2 variants has already been shown to coincide with epidemic surges in multiple parts of the world. As already mentioned, most - if not all - of the above-mentioned evidence directly emerges from in-depth research conducted by internationally recognized molecular epidemiologists. These researchers acknowledge that rising population immunity and public health measures may complicate control of the pandemic by virtue of their positive selection effect on immune escape variants. However, they do not advance any hypothesis as to the underlying causes of rising immunity that leads to a transmission advantage for S-directed immune escape mutants other than through individuals who are chronically ill and sustain prolonged viral replication as a result of insufficient immune control. This is probably an area where molecular epidemiologists should synergize with immunologists to understand, for example, that during a pandemic previously asymptomatically infected subjects may become re-infected at a point in time where their innate CoV-nonspecific Abs are still suppressed by suboptimal S-specific Abs (which they acquired as a result from that previous asymptomatic infection). More importantly, molecular epidemiologists may find it useful to learn from vaccinologists as a better understanding of the immune priming by vaccines, as compared to natural infection, could inform a more targeted surveillance of viral mutations and variants. In this regard, it is important for them to understand that mass vaccination in the heat of a pandemic, much more than natural infection of immune suppressed subjects, provides a panoply of conditions for individuals to become infected while only harboring suboptimal, S-specific Abs. Suboptimal stimulation of S-specific Abs could be due to individual insufficiencies in immunological responsiveness to the vaccine but inevitably occurs in all vaccinees for as long as they are in the process of mounting their Ab response. This is particularly problematic in vaccinees who have not yet received the second shot of a 2-dose Covid-19 vaccine. In these vaccinees, the S-specific Ab response after the 1st dose will not suffice to control replication and transmission of more infectious viral variants. In addition, exposure of vaccinees to antigenically different variants is also to be considered a case of suboptimal S-specific Abs and would already explain why increasingly problematic variants (e.g., VoCs or other problematic immune escape variants with deletions in the N-terminal domain of S protein) are overrepresented in vaccine breakthrough infections (5,14). All of the above situations will enable a growing part of the population (vaccinees!) to exert selective immune pressure on the S protein when exposed to Sars-CoV-2 (which is all but a rare event during a pandemic!).
Unfortunately, vaccinees are not systematically monitored for shedding of antigenic Sars-CoV-2 variants and hence, the information on the type of variants they shed is scarce, the effective reproduction number largely underestimated and the evolutionary potential of the virus to evade S-specific Ab underexplored. As a result, reports on the relative distribution of variants are likely skewed to less problematic variants as those may still have a fitness advantage in vulnerable people compared to variants comprising a combination of nAb-resistant mutations.
As some sources of population-level selective pressure are known to be amenable to human intervention, there is an urgent need for systematic genomic sequencing of circulating variants in vaccinees as this would provide us with unambiguous evidence as to whether mass vaccination campaigns enable a population to exert immune-mediated selective pressure on critical functional characteristics of Sars-CoV-2 such as virulence, transmissibility and nAb-resistance.
Why will mass vaccination campaigns conducted in the midst of this pandemic inevitably cause viral immune escape at the population level, irrespective of the speed at which these campaigns are progressing?
It has been established that the threshold number of individuals required for natural selection is far lower than the threshold number for neutral genetic drift to drive evolutionary changes in the Sars-CoV-2 landscape (2). But also mathematical modelling has already shown that prophylactic nAb treatment (including vaccination) of a relatively low percentage of the population already suffices to provide an immune escape mutant impacting the neutralizing Ab capacity with a significant transmission advantage compared to the wild virus (2). In addition, mass vaccination campaigns conducted during a pandemic will inevitably enroll people who are exposed to an environment of relatively high infectious pressure. This will increase the likelihood for vaccinees to harbor a dominant double or even triple mutant that is capable of evading a multitude of nAbs and hence, likely to serve as a source for population-level resistance of Sars-CoV-2 to Covid-19 vaccines.
From a scientific perspective, it is impossible to imagine that the ongoing large-scale vaccination campaigns are not going to rapidly and globally breed vaccine-resistant mutants instead of generating vaccine-mediated herd immunity. As of early March 2021, I have, therefore, been warning several times against the rapid resurgence of Sars-CoV-2 morbidity and mortality rates that this evolution is now highly likely to cause, especially in vaccinees. Hence, I repeatedly called upon PHAs world-wide to immediately stop all mass vaccination campaigns.
Will the consequences of viral resistance to Covid-19 vaccines also affect non-vaccinated individuals?
Resistance to Covid-19 vaccines will only raise the infectious pressure and thereby increase the likelihood for non-vaccinated subjects to contract Covid-19 disease. On the other hand, nonfunctional vaccinal Abs in vaccinees could lead to Ab-dependent enhancement (ADE) of Covid-19 disease (2, 25). ADE is likely to shorten the pre-symptomatic phase of Covid-19 disease, viral shedding could be more easily and rapidly contained. Timely containment of viral transmission would contribute to diminishing exposure of non-vaccinated individuals to high infectious pressure. Provided unhampered functionality of their CoV-nonspecific innate Abs, diminished infectious pressure would likely protect non-vaccinated individuals from contracting Covid-19 disease. However, non-vaccinated individuals as well might be susceptible to ADE if they become exposed to Sars-CoV-2 while harboring S-specific nAbs as a result of natural infection. The risk may exist for as long as the concentration of these nAbs in their blood is high enough to outcompete innate, CoV-nonspecific Abs at the portal of viral entry. It is important to consider, though, that both, vaccinated and non-vaccinated subjects who previously contracted Covid-19 disease might be better protected against severe disease upon re-exposure thanks to the priming of protective, cytotoxic T cells.
Vaccine-elicited S-specific T cell responses against variants are largely preserved and have been suggested to enable robust vaccine efficacy against variants when the neutralizing capacity of vaccine-elicited Abs may not provide sufficient protection (11). Could vaccine-induced T cell immunity, therefore, diminish the prevalence of viral variants and mitigate resurgence of morbidity and mortality waves?
Some publications suggest that increased breadth in S-specific vaccinal CD8+ T cell responses in vaccinated as compared to non-vaccinated individuals may compensate for insufficient neutralization capacity of S-specific vaccinal Abs against a number of new, more infectious variants. This would, therefore, still enable vaccines to provide robust protective vaccine efficacy against emerging variants. It is unlikely, though, that largely preserved T cell responses against variants mediate S-specific killing of virus-infected cells. This is because killing by cytolytic CD8+ T cells (CTLs) is known to be genetically determined by protective MHC class I alleles. No evidence of promiscuous or universal, Sars-CoV-2 S-derived CTL epitopes has been reported. The robustness of protective vaccine efficacy against variants across a genetically heterogeneous host population can, therefore, not be explained by CTL-mediated killing as the latter would be MHC class I-restricted, even if S-derived CD8+ T cell epitopes are conserved. Robustness of protective vaccine efficacy against multiple variants is most likely due to innate, cytokine-mediated immune cascades that are largely triggered by polyfunctional, broadly preserved memory T cells. These cytokine-mediated responses likely synergize with nAbs to further reduce viral load (and hence, likely diminish the likelihood of [severe] disease) but fail to abrogate viral transmission or curtail the expansion of viral variants. This is because non-antigen(Ag)-specific innate immune responses cannot target and eliminate Sars-CoV-2-infected cells. It is reasonable to assume, however, that vaccine-elicited S-specific T cell responses will contribute to promote viral evasion from innate immune mechanisms when elicited in the context of large-scale vaccination campaigns during a pandemic. Innate immune evasion mechanisms are well known and have been extensively described (12, 13). This would ultimately results in a robust, universal (i.e., MHC-unrestricted) and nonAg-specific decline in vaccine efficacy towards all infectious Sars-CoV-2 variants.
Why are mass vaccination campaigns likely to increase Covid-19 morbidity and mortality rates?
From a purely scientific perspective and even regardless of all (important!) ethical issues they raise, mass vaccination campaigns conducted in the midst of a pandemic are doomed to fail and have unforeseeable health consequences, not only for individual vaccinees but also for the global human population.
As already mentioned, changes in the ‘traditional’ host environment (e.g., implementation of stringent public health measures and social distancing; overcrowding) may alter the evolutionary dynamics of the pandemic and drive natural selection and dominant propagation of more infectious variants (or, alternatively, promote their rapid expansion once they become de novo introduced into a population). Likewise, it is reasonable to assume that large-scale vaccination campaigns conducted during a pandemic will drive natural selection and dominant propagation of nAb-evasive variants. However, as viral adaptation evolves, replication and transmission of such naturally selected immune escape variants by asymptomatically infected or mildly ill vaccinees will become more and more frequent and eventually increase the risk of rapid re-exposure for non-vaccinated, previously asymptomatically infected individuals. This is now likely to prompt a new wave of morbidity and mortality in the non-vaccinated part of the population. Iin countries where mass vaccination campaigns are rolled out on a background of low infectious pressure, it will take more time for rising vaccine coverage rates to drive convergent evolution of additional, naturally selected mutations such as to ensure viral persistence in the face of a stronger and more widespread vaccine-induced immune response. However, there shall be no doubt that the endgame of this convergent evolution of vaccine-mediated immune escape mutants is full resistance of Sars-CoV-2 to the Covid-19 vaccines. When this happens, vaccinees in particular will become extremely vulnerable to Covid-19 disease as they will no longer be able to rely on their innate Abs for those will be outcompeted by their vaccinal Abs for binding to S protein.
It is important to note that it suffices for the virus to escape S- or RBD-directed immune pressure in order to become more infectious or to resist protective (neutralizing) vaccinal Abs, respectively. As neither previously asymptomatic, non-vaccinated individuals nor previously immunologically naïve vaccinees have experienced protective T cell priming, immune evasion from S-specific Abs is sufficient for Sars-CoV-2 to cause Covid-19 disease in these people. Given the intensity of natural selection signals observed in the current genomic landscape of Sars-CoV-2 spike protein (1), it is reasonable to assume that a further rise in population-level immune selection pressure on this protein (i.e., as a result of continued mass vaccination campaigns) will ultimately provide variants capable of evading a full set of vaccinal Abs (including those raised by 2nd generation vaccines) with a transmission advantage. As already mentioned, this is expected to dramatically raise morbidity and mortality rates in vaccinees.
Why are most countries not yet affected by enhanced circulation of increasingly immune resistant variants despite an advanced stage of their mass vaccination campaigns?
Full-fledged vaccine resistance is not yet observed as it may take much longer for a combination of multiple synergizing immune escape mutations to occur in a sufficient number of individuals in the population. However, once these immune escape variants are present in sufficient frequency, they will establish rapidly in populations that are subject to mass vaccination (due to widespread S-directed immune selection pressure). It is, however, important to note that during this period of pandemic quiescence, vaccination may lead to an increased risk of ADE as S protein from intermediate variants, which possess only a subset of the S-associated mutations required for full resistance to the vaccine, may still be recognized (but not neutralized) by vaccinal Abs (see above).
Will mass vaccinations have a different outcome depending on geographic and/ or demographic factors?
Regardless of the current evolutionary dynamics of the pandemic in any given country, immune escape variants will ultimately converge to a common adaptive endpoint, which is full resistance to S-directed nAbs induced by Covid-19 vaccines or resulting from natural infection. The speed at which Sars-CoV-2 is expected to develop resistance to S-specific nAbs induced by the current vaccines or acquired following natural infection will – among other, above-mentioned factors - depend on the speed at which mass vaccination campaigns are conducted. Enrolling youngsters and children in these mass vaccination campaigns is only going to rapidly expand the breeding ground for nAb-resistant variants and expedite the evolution depicted above.
Why are follow-up vaccines using key nAb epitopes from variant-associated spike protein unlikely to solve the issue of immune escape variants?
First, spike RBD displays a high level of evolutionary versatility whereas Covid-19 vaccines only induce a relatively narrow immune response (i.e., directed at a few immunodominant domains within a single viral protein). It is, therefore, reasonable to assume that the evolutionary capacity of Sars-CoV-2 to evolve variants capable of evading multiple nAbs reaches far beyond the breadth of S-associated epitopes Covid-19 vaccines can possibly target (2, 3, 9). This already suggests that these vaccines are highly likely to drive mutation-mediated escape from S-specific host Abs.
Upon re-vaccination with updated S-targeting vaccines (so-called ‘second generation’ vaccines), previously vaccinated people will rapidly recall their original vaccinal Abs while those who are waiting for their updated vaccine shot may do so as a result from natural exposure (as the virus will, indeed, still be circulating, primarily among asymptomatically infected vaccinees). In immunology, this phenomenon is known as ‘antigenic sin’. Consequently, a high level of S-directed immune selection pressure will be maintained within the vaccinated population, thereby promoting further expansion of viral variants and accelerating the speed at which variants will evolve a repertoire of additional immune escape mutations that is sufficient to eventually enable full resistance to the updated vaccine as well. In this context, it is also important to note that one single additional mutation could suffice to abolish the enhanced neutralization capacity of the updated vaccine by virtue of epistatic interaction between the additional mutation and multiple previously established adaptive mutations targeted by vaccinal nAbs. In addition, molecular epidemiologists are increasingly worried about a potential expansion of recombination-generated combinations of immune escape mutations as those could occur during co-infections with different variants and generate even more problematic variants of concern that will better match the evolving fitness landscape of the continuing pandemic (1, 9).
When high infectious pressure coincides with high immune selection pressure, partially resistant variants can be expected to transit more rapidly through the ’valley of lower fitness’ and hence, expedite the emergence of dominant variants that fully resist the updated vaccines. This is to say that steadily increasing vaccine coverage rates combined with relaxed infection prevention measures and global expansion in prevalence of more infectious variants are now serving as a breeding ground for upcoming nAb-resistant variants.
Re-vaccination with second generation vaccines is all but comparable with seasonal updates of Influenza vaccines as the latter are administered on a background of herd immunity. Dedicated molecular epidemiologist seem to recognize the likelihood that updated S-based Covid-19 vaccines may fail and state that “Further studies may be required to understand the risk immune evasion poses to a strategy of annually updated vaccines” (2).
Could an immediate and global halt of mass vaccination campaigns still prevent the emergence of more harmful viral recombinations or resistance of Sars-CoV-2 to Covid-19 vaccines?
A global and immediate halt of mass vaccination campaigns would allow to diminish immune selective pressure exerted on sites within the S protein that mediate nAb evasion. However, at this fairly advanced stage of the global mass vaccination program, it is probably already too late to prevent viral resistance to S-Abs, even if mass vaccination campaigns would immediately and globally be halted, and even though vaccine coverage rates are still fairly low in a number of low-income countries. This is because
-
nAb-resistant virus selected in a particular population will easily adapt and expand upon their introduction into other populations that are undergoing a similar shift in the Sars-CoV-2 fitness landscape, even though the local variants they are harboring are less advanced in their adaptive process of evolutionary convergence of immune escape mutations
-
the current spectrum of escape mutations already lays the groundwork for multiple recombinations to occur as viral spread continues. Combinations of immune escape mutations more readily enable variants to circumvent vaccine-induced immunity or acquire other phenotypic characteristics that could potentially be more harmful (1, 2, 3, 9). Some of these combinatorial variants could, therefore, be more problematic than those which circulated before.
Consequently, it is reasonable to assume that an immediate halt of all Covid-19 vaccination campaigns could at most delay full resistance of Sars-CoV-2 to the vaccines by a few months. However, recombinations are likely to lead to super variants with unpredictable phenotypic characteristics, some of which may be responsible for a further increase in viral infectiousness and/ or virulence or could even enable adaptation to another mammalian species (7). As already mentioned, recombinations are promoted by co-infection with different variants. At this stage of the pandemic, co-infection with different variants becomes increasingly likely as infection prevention measures are now being relaxed in many countries (9). Adaptation to other mammalian species may result from enhanced binding affinity of mutated spike protein for their Ace-2 receptor (e.g., in case of the Sars-CoV-2 Y453F mink variant) and generate an additional asymptomatic reservoir for recurrent transmission to humans (4).
Unless aggressive multidrug treatment is implemented at an early stage of disease and large-scale chemoprophylaxis campaigns are conducted, resistance of Sars-CoV-2 to Covid-19 vaccines is, most certainly, going to provoke a steep incline of morbidity and mortality rates in vaccinees, especially in those who did not contract Covid-19 disease prior to vaccination.
Are scientists suspicious of mass vaccination enhancing expansion of vaccine-resistant Sars-CoV-2?
In this regard, it suffices to cite D. Van Egeren et al. (2):
“Evidence from multiple experimental studies showing that single RBD point mutations can lead to resistance to neutralizing convalescent plasma from multiple donors suggests that specific single mutants may be able to evade spike-targeting vaccinal immunity in many individuals and rapidly lead to spread of vaccine-resistant SARS-CoV-2. One variant that can escape convalescent plasma neutralization is already circulating in South Africa and could experience greater positive selection pressure once vaccines are deployed widely”. These authors further suggest that natural selection of multiple mutations in individuals possessing nAbs against Sars-CoV-2 spike protein “could accelerate the emergence of vaccine-resistant strains in the months following vaccine deployment” and state that “Further studies are required to understand the risk immune evasion poses to a strategy of annually updated vaccines”. Additional citations from scientists studying the evolutionary biology of Sars-CoV-2 go as follows: “… vaccines themselves represent a selection pressure for evolution of vaccine-resistant variants…” (9).
The notion that vaccines have the capacity to drive immune evasion of mutable pathogens and enable dominance of antigenically different variants with altered biological characteristics when deployed at population scale is certainly not new (8, 13, 22). This knowledge combined with the remarkable ability of Sars-CoV-2 to rapidly adapt to new environments and different hosts, in particular via convergent evolution of specific spike mutations (7, 23, 24), led at least some scientists to state that “With increasing levels of host immunity helped by the deployment of vaccines and ongoing widespread SARS-CoV-2 circulation, we fully expect to see increased evidence for adaptive evolution in Spike and other genes…” (7) or that “Mutations affecting the antigenic phenotype of SARS-CoV-2 will enable variants to circumvent immunity conferred by natural infection or vaccination” (3). Other scientists come to the following conclusions: “Subsequently, many other changes in the spike protein were found to propagate rapidly, showing that the bulk of the selection pressure on this protein comes from adaptation to the host. We can therefore anticipate that this protein, and to a lesser extent the nucleocapsid protein, will evolve most rapidly under the selection pressure of vaccination” (9) or: “However, there is growing evidence that mutations that change the antigenic phenotype of SARS-CoV-2 are circulating and affect immune recognition to a degree that requires immediate attention”. But scientists also acknowledge that a recombination event within Sars-CoV-2 variants or between a Sars-CoV-2 variant and Sars-CoV-2 from bats could be highly problematic in terms of precipitating resistance to the vaccines: “Due to the high diversity and generalist nature of these Sarbecoviruses, a future spillover, potentially coupled with a recombination event with SARS-CoV-2, is possible, and such a ‘SARS-CoV-3’ emergence could be sufficiently divergent to evade either natural or vaccine-acquired immunity, as demonstrated for SARS-CoV-1 versus SARS-CoV-2. We must therefore dramatically ramp up surveillance for Sarbecoviruses at the human–animal interface and monitor carefully for future SARS-CoV emergence in the human population” (7).
Biologists studying the genomic composition of CoVs in general and that of CoV-2 in particular published convincing evidence that also innate, nonAg-specific antiviral immune responses exhibited by infected host tissues (i.e., not only including lymphoid tissue!) exert immune selection pressure that shapes the genomic composition of infecting CoVs (10). As already mentioned above, vaccine-mediated T cell immunity is thought to contribute to protection by virtue of the innate immune cascades they stimulate.
It is generally agreed amongst molecular epidemiologists that resistance to nAbs and hence, to vaccine-induced immunity, could considerably be delayed by reducing the number of active infections (i.e., infectious pressure) in ways that do not exert a specific selective pressure on the virus. They literally state: “In this context, vaccines that do not provide sterilizing immunity (and therefore continue to permit transmission) will lead to the buildup of large standing populations of virus, greatly increasing the risk of immune escape”(2).
It is almost impossible to believe that scientists studying the genomic/ molecular epidemiology or evolutionary biology of Sars-CoV-2 would not understand that mass vaccination campaigns promote natural selection and propagation of immune escape variants when they all come to the conclusion that selective immune pressures exerted by antiviral host immune responses provide fitness-enhancing mutations with a transmission advantage enabling their adaptation to the infected host (tissue)-specific environment. In light of all scientific evidence provided and the sinister perspective of the current evolution when put in an immunological and vaccine context, knowledgeable scientists should feel a moral and ethical obligation to loudly voice their concerns publicly. It is appalling that some leaders of the very institutes disclosing some of these critically enlightening data on the evolutionary molecular dynamics of circulating variants seem to be denying the observations of their co-workers and continue to blindly advocate for mass vaccination. Instead, some of them are even bold enough to encourage arrogant and scientifically illiterate fact-checkers to misrepresent compelling scientific evidence as a hoax and debunk experts who put their career on the line in making this critically important information accessible to the broader public.
Compassionate scientists who have been taking a deep dive in these complex matters are now increasingly left with the impression that health authorities and advising experts will simply continue to deny that they are desperately wrong, no matter how compelling the scientific evidence that has been brought to the table and no matter the consequences this unprecedented public health experiment may involve for many years to come.
It’s been raining incessantly for three days. It is a cool early morning in the beginning of July and I have just made a cup of coffee. Now an electrical power outage has occurred and so I am sitting in a rocking chair in the semi-darkness savoring my coffee and feeling thankful that I made it in time. I have a close relationship with coffee and the end of night and the break of day. As for time, that is as mysterious to me as the fact that I am sitting here in its embrace. The electric clocks have stopped. I think: To exist – how amazing!
More than the coffee, however, I am luxuriating in the sound of the tumbling rain. Its beautiful music creates a cocoon of peace within which I find temporary joy. The joy of doing nothing, of pursuing no purpose. Of knowing that whatever I do it will never be enough, for me or anyone, and the world will continue turning until time stands still, or whatever time does or is according to those who invented it. I will be gone and others will have arrived and the water will flow from the skies and the clocks will still tell people what they don’t know – time – although they will continue to tell it.
Humans are the telling animals.
A few weeks ago, when this area was in a mini-drought, the local newspaper, in the typical wisdom of such cant, had a headline that said “there is a threat of rain later this week.” They are experts at threats. This is the corporate media’s purpose. Rain is a threat, joy is a threat, doing nothing is a threat, the sun is a threat – but the real threats they conceal. To create fear seems to be their purpose, as they do not tell us about the real threats. Their purpose is not to tell the truth, but if you listen closely you can hear it.
In the middle of the night I woke up to go to the bathroom, and outside the small bathroom window I watched the rain engulfing the lower roof and sluicing down the shingles in two heavy streams. I thought how the desiccated mind of the headline writer must be feeling now, but then I realized that he or she was asleep, as usual. There is a moist world and a dry one, and the corporate media is run by arid souls who would like to make the world a desert like their masters of war in Washington.
Then as I sit here my brief peace is roiled by the memory of reading Tacitus, the Roman historian, and his famous quote of Calgacus, an enemy of Rome:
These plunderers of the world [the Romans], after exhausting the land by their devastations, are rifling the ocean: stimulated by avarice, if their enemy be rich; by ambition, if poor; unsatiated by the East and by the West: the only people who behold wealth and indigence with equal avidity. To ravage, to slaughter, to usurp under false titles, they call empire; and where they make a desert, they call it peace.
I think of former Secretary of Defense Donald Rumsfeld on his recent deathbed. Here was a man whose entire life was dedicated to the American Empire. He spent all his allotted time making war or making money from the spoils of war. He was a desert maker, a slaughterer for the Empire. No doubt he died very rich in gold.
I can no longer hear the rain because my mind is filled with the loud thought of what Rumsfeld thought as he lay dying. Was he sorry? Did he believe in God or was his god Mars, the Roman god of war? Did he smile a bloody smile or say he was sorry and beg for forgiveness from all his innocent victims? Did he see the faces of the children of Iraq that he slaughtered? Or did he pull an Eichmann and say, “I will leap into my grave laughing”?
Your guess is as good as mine, but mine leans toward the bloody smile of a life well spent in desert making. But that is a “known unknown.”
Rolling thunder and a lightning strike in the east jolt me back from my deaf dark thoughts. The sound of the rain returns. The coffee tastes great. Peace returns with the unalloyed gift of the ravishing rain.
Yet the more I sit and listen and watch it soundly stipple the garden and grass, the more thoughts come to me, as my father once told me: Thoughts think us as much as we think thoughts. It’s what we do with our thoughts that count, he said, and like lightning, if we don’t flash when we are given the gift of life, when we’re gone, it will be as if we never were, like the lightning before it flashed.
Thomas Merton’s prophetic words from his hermitage in the Kentucky woods in 1966 think me:
Let me say this before rain becomes a utility that they can plan and distribute for money. By ‘they’ I mean the people who cannot understand that rain is a festival, who do not appreciate its gratuity, who think that what has no price has no value, that what cannot be sold is not real, so that the only way to make something actual is to place it on the market. The time will come when they will sell you even your rain. At the moment it is still free, and I am in it. I celebrate its gratuity and its meaninglessness.
There are moments in many lives when, if one is lucky, they are initiated into a ritual that sustains them throughout life. To others these experiences can easily seem paltry and meaningless, but to the receiver they offer a crack into deeper dimensions of being and becoming. For me it was my introduction to coffee during a hurricane.
My father had driven my mother, three of my sisters, and me to Jones Beach on Long Island. This was before people checked the weather every minute. The sky in the southwest grew darker as we drove, but on we went. The beach was deserted except for some gulls and the parking lot empty. My father parked the car close to the beach and while my sisters and mother sat in the car, and my mother, listening to the weather reports, issued warnings to us, my father and I ran like wild dogs into the heavy surf despite her admonitions that the hurricane from the south was arriving sooner than expected. It started to rain hard. The surf picked up. We swam and got battered and shouted exultantly and came out shaking with the chills. A pure white sea gull landed on my wet head and my father laughed. Awe-struck, I stood stock still and my shaking stopped. In its mouth the sea gull held a purple ribbon, which it dropped at my feet as it flew off. I grabbed the ribbon and we jogged up to the concession building where there was one man working. My father ordered coffee and a hot chocolate for me. But they had run out of hot chocolate. So my father ordered two coffees and filled mine with three or four sugars. I had never sampled coffee and didn’t like the smell, but my father said to drink it, with the sugar it will taste good and it will warm you up. It strangely tasted like hot chocolate. We toasted our adventure as I drank my Proustian madeleine at eleven-years-old.
I had put the ribbon on the counter as we drank. When we were going back to the car, I noticed there were words on the ribbon. They said: Rest in peace. I have long lost the ribbon but retain its message.
So now every morning between the end of night and the break of day, I sit with my coffee and listen. And even when it isn’t raining, I watch the birds emerge from their nightly rests to greet the day with their songs. They tell me many things, and they are all free.
This morning I am wondering if Donald Rumsfeld ever heard them.
I suspect their message was an “unknown unknown” for him, just like the gift of rain. He preferred the rain of death from the skies in the form of bombs and missiles. He was only doing his job.
He made a desert and called it peace.
Expert statement regarding Comirnaty – COVID-19-mRNA-Vaccine for children
Summary
This expertise on the use of the Pfizer COVID-19 vaccine (Comirnaty, BNT162b2) in adolescents is divided into three sections, which will deal with the following questions, in order:
- Is vaccination of adolescents against COVID-19 necessary?
- Is the Pfizer COVID-19 vaccine effective?
- Is the Pfizer COVID-19 vaccine safe?
The arguments presented in Section 1 pertain to all COVID-19 vaccines, whereas those in Sections 2 and 3 apply specifically to the Pfizer vaccine.
Section 1 will show that vaccination of adolescents COVID-19 is unnecessary, because
- in this age group the disease is almost always mild and benign;
- for the rare clinical cases that require it, treatment is readily available;
- immunity to the disease is now widespread, due to prior infection with the virus (SARS-CoV2) or with other coronavirus strains; and
- asymptomatic adolescents will not transmit the disease to other individuals who might be at greater risk of infection.
Section 2 will demonstrate that the claims of efficacy which Pfizer attaches to its vaccine—namely, 95% efficacy in adults, and 100% in adolescents—are
- misleading, because these numbers pertain to relative, not absolute efficacy, the latter being on the order of only 1%;
- specious, because they refer to an arbitrarily defined, clinically meaningless evaluation endpoint, whereas no efficacy at all has been demonstrated against severe disease or mortality;
- most likely altogether fraudulent.
Section 3 will show that the safety profile of the Pfizer vaccine is catastrophically bad. It will be discussed that - Pfizer, the EMA, and the FDA have systematically neglected evidence from preclinical animal trials that clearly pointed to grave dangers of adverse events;
- the Pfizer vaccine has caused thousands of deaths within five months of its introduction;
- The agencies that granted emergency use authorization for this vaccine committed grave errors and omissions in their assessments of known and possible health risks.
The only possible conclusion from this analysis is that the use of this vaccine in adolescents cannot be permitted, and that its ongoing use in any and all age groups ought to be stopped immediately.
Go to original to read the entire report


Dr. David Martin has done a detailed review of the 73+ patents relevant to Covid and the facts are shocking and speak for themselves.
I’m allergic to conspiracies but this one smells real to me.
Everything we are being told by our “leaders” about Covid is apparently wrong.
I watched this July 9 video presentation three times before posting it because it’s so evil that it’s hard to digest and accept.
Click this link to watch the video from it’s Odysee source:
Here is a copy on YouTube which may disappear soon.
Here is a document with references for fact checking Martin’s claims:
Click to access The-FauciCOVID-19-Dossier2532.pdf
Not mentioned by Martin but additive to the case against our “leaders” is:
- aggressive undermining and censorship of Ivermectin, an inexpensive and safe drug for prevention and treatment;
- no promotion of inexpensive and safe methods for strengthening immune systems;
- irrational policies such as vaccinating people who have recovered from Covid;
- no debate of Dr. Bossche’s theory that a mass vaccination campaign during a pandemic with a non-sterilizing vaccine may create more dangerous variants that are immune to the vaccine and a vaccine degraded natural immune system;
- no investigation of the virus source nor measures to prevent a recurrence.
I feel like I’m having a seriously deranged dream.
If anyone is able to re-spin the data Martin presents into a pro-social or benign scenario, I would be grateful to hear your ideas.
Read the comments - they caution about Dr. Martin also holding the belief that the motive is population control, a "wacky" concept. So he might just be a "crazy guy". That might be so, or it might not be, but the data he presents about the patents and the explicit motivations is documentary, and can be checked, independent of whether or not he is "crazy".
During a Covid surge, what proportion of the population is exposed to an infective dose of the virus, which they either fight off with no or minimal symptoms or are infected by? This is one of the most important questions scientists need to answer.
It’s closely related to the question of whether lockdowns work. If lockdowns work then, as per SAGE and Imperial orthodoxy, the restrictions successfully prevent the virus from reaching most people, who remain unexposed and susceptible – and hence in need of vaccination to protect them when the protective restrictions are lifted. If lockdowns don’t work, however, then they don’t prevent the virus spreading, and thus the majority of people will be exposed to it as it spreads around unimpeded by ineffectual restrictions.
Another related question is: What proportion of exposed people are infected? Using ONS data we can estimate that around 10-15% of the country tested positive for SARS-CoV-2 over the autumn and winter. How many were exposed to the virus to produce this number of infections? Was it, say, 10-20%, with half to all of them catching the virus? Or was it more like 80-90%, with around 10% being infected? It’s a question that makes all the difference in our understanding of the virus and how to respond to it.
If almost all are exposed during a surge, and relatively few of them are infected, then a number of things follow. First, most people have enough immunity to fight off the virus when exposed to it, and only a small minority become infected. Second, the surge ends when enough of that small minority who are particularly susceptible to this virus or variant acquire immunity through infection, i.e., when herd immunity is reached. Third, there won’t be another surge or wave until there is a new virus or variant which evades enough of the existing population immunity to require herd immunity to be topped up via a further spread of infections.
If, on the other hand, very few are exposed during a surge, and most of them are infected, none of these things is true. It means: Most people have little immunity and are highly susceptible. A surge which infects 10-20% of the population has exposed not much more than that. The surge does not end because of herd immunity but because of restrictions. And there will be another surge as soon as restrictions are eased or behaviour changes and the unexposed begin to be exposed again. SAGE orthodoxy, in other words.
The evidence, however, is strongly supportive of the first position – ubiquitous exposure – not the second, limited exposure.
Consider the secondary attack rate (SAR, the proportion of contacts an infected person infects). Data from Public Health England consistently shows this figure sits around 10-15%, meaning around 85-90% of the contacts of infected people do not become infected. It rises during a surge, which is typically due to the higher SAR of a novel variant, and then falls after the surge, as the new variant’s SAR also falls.
Such data is much more consistent with ubiquitous exposure than with limited exposure, as it shows that only a minority of those exposed to an infected person are themselves infected (10-15%), meaning ubiquitous exposure with a minority infected is the much more plausible scenario. This meshes with the data on high levels of prior immunity via T cells and other mechanisms. It is also broadly in line with the data from the Diamond Princess cruise ship in February 2020, where an unmitigated outbreak resulted in 19.2% of the 3,711 people on board testing PCR positive (18% of those without symptoms).
Another key data point is the fact that surges consistently peak abruptly and begin to fall, independently of the imposition of restrictions. For instance, as Professor Simon Wood has shown, all three lockdowns in England were imposed after infections had peaked and begun to decline. Similarly, multiple peer-reviewed studies have shown no relationship between the imposition of restrictions and Covid infections or deaths across different countries and U.S. states.
The pattern of abrupt peaks and falls in incidence, independent of restrictions, is strongly indicative of hitting a herd immunity threshold (or overshooting it), as the virus or variant runs out of susceptible people to infect and exhausts itself.
Similarly, when restrictions are lifted there is typically no immediate surge, as there wasn’t in Europe last summer and in numerous U.S. states such as Texas and Mississippi in spring 2021. Surges only tend to occur when a new variant arrives, which again suggests it is not restrictions that are preventing spread to a still highly susceptible population but herd immunity that is preventing it, at least until a new virus or variant arrives to temporarily disturb it.
How, though, does the virus circumvent restrictions to achieve ubiquitous exposure of the population, and apparently without being noticeably even slowed down by the restrictions or voluntary distancing behaviour?
The answer, as I have suggested previously, likely lies in the airborne transmission of the virus. It is likely that the virus primarily spreads through building up to infective levels in the air, and that people are infected by breathing it in (a form of transmission which face masks do little or nothing to prevent). During a surge the virus becomes increasingly ubiquitous in the air at higher concentrations, accelerating exposure and infections until the herd immunity threshold is hit, at which point it abruptly enters decline. This explains why even though it is at its highest point of prevalence and was spreading at its fastest rate just a few days before, it suddenly stops and enters sustained decline. It is hard to see how any explanation other than herd immunity can explain this consistently abrupt change in the rate of virus transmission, particularly as there is no evidence of a similarly abrupt change in public behaviour in the mobility data.
Is there any concrete evidence that SARS-CoV-2 or other airborne viruses like influenza are ubiquitous in the air? Yes, there is. As HART notes in its bulletin this week:
For novel influenza viruses, between 7% and 8% are susceptible and develop antibodies in the first winter, much as we saw with SARS-CoV-2… If a certain proportion of the population are susceptible to infection in any one season, those individuals will end up infected sooner or later, regardless of which day they are exposed.
Studies have demonstrated that influenza is transmitted by aerosol particles and that such particles are prolific, indeed ubiquitous, in all indoor settings during the winter season. What stops people contracting the virus is their level of susceptibility, not their level of exposure.
HART refers to a study on influenza from 2014, which argues:
There are some amounts of the virus in the air constantly. These amounts are generally not enough to cause disease in people, due to infection prevention by healthy immune systems. However, at a higher concentration of the airborne virus, the risk of human infection increases dramatically. Early detection of the threshold virus concentration is essential for prevention of the spread of influenza infection.
The idea of a “threshold virus concentration” at which an outbreak is triggered (rather than just low level transmission) may be important for understanding how airborne viruses spread, and how they can become ubiquitous during a surge. Seasonal factors such as temperature, humidity, UV radiation, human behaviour (e.g. gathering indoors with little ventilation), and cycles in the human immune system may play a role in how easily this threshold concentration is reached.
A study in JAMA tested the air in hospitals for SARS-CoV-2 and found plenty, particularly in the public areas:
Overall, 14 of 42 samples (33.3%) in public areas were positive, with 9 of 16 (56.3%) in hallways, 2 of 18 (11.1%) in other indoor areas, and 3 of 8 (37.5%) in outdoor public areas (P = .01).
There isn’t yet much evidence from other settings, though a study, COVAIR by Imperial College, is underway and the results will be of great interest when they eventually appear.
To my mind, this is the explanation that (at least for now) explains all the known facts better than others – the low secondary attack rate, the ineffectiveness of lockdowns, the outbreaks that explode then suddenly end, the absence of resurgence when restrictions are lifted, the repeated hitting of herd immunity, and so on. At the heart of it is the idea of ubiquitous exposure – that almost everyone, not just a small percentage, are exposed each time the virus passes through, and the vast majority are already immune.
Dr. Charles D. Hoffe, BSc, MB, BCh, LMCC
Lytton Medical Clinic
Lytton BC V0K 1Z0
5 April, 2021
OPEN LETTER
Dr. Bonnie Henry,
British Columbia Provincial Health Officer
Ministry of Health
1515 Blanchard Street
Victoria, BC, V8W 3C9
Dear Dr. Henry,
The first dose of the Moderna vaccine has now been administered to some of my patients in the community of Lytton, BC. This began with the First Nations members of our community in mid-January, 2021. 900 doses have now been administered.
I have been quite alarmed at the high rate of serious side-effects from this novel treatment.
From this relatively small number of people vaccinated so far, we have had:
- Numerous allergic reactions, with two cases of anaphylaxis.
- One (presumed) vaccine induced sudden death, (in a 72 year old patient with COPD. This patient complained of being more short of breath continually after receiving the vaccine, and died very suddenly and unexpectedly on day 24, after the vaccine. He had no history of cardiovascular disease).
- Three people with ongoing and disabling neurological deficits, with associated chronic pain, persisting for more than 10 weeks after their first vaccine. These neurological deficits include: continual and disabling dizziness, generalised or localized neuromuscular weakness, with or without sensory loss. The chronic pain in these patients is either generalised or regional, with or without headaches.
So in short, in our small community of Lytton, BC, we have one person dead, and three people who look as though they will be permanently disabled, following their first dose of the Moderna vaccine. The age of those affected ranges from 38 to 82 years of age.
So I have a couple of questions and comments:
- Are these considered normal and acceptable long term side-effects for gene modification therapy? Judging by medical reports from around the world, our Lytton experience is not unusual.
- Do you have any idea what disease processes may have been initiated, to be producing these ongoing neurological symptoms?
- Do you have any suggestions as to how I should treat the vaccine induced neurological weakness, the dizziness, the sensory loss, and the chronic pain syndromes in these people, or should they be all simply referred to a neurologist? I anticipate that many more will follow, as the vaccine is rolled out. This was only phase one, and the first dose.
- In stark contrast to the deleterious effects of this vaccine in our community, we have not had to give any medical care what-so-ever, to anyone with Covid-19. So in our limited experience, this vaccine is quite clearly more dangerous than Covid-19.
- I realize that every medical therapy has a risk-benefit ratio, and that serious disease calls for serious medicine. But we now know that the recovery rate of Covid-19, is similar to the seasonal flu, in every age category. Furthermore, it is well known that the side effects following a second shot, are significantly worse than the first. So the worst is still to come.
- It must be emphasised, that these people were not sick people, being treated for some devastating disease. These were previously healthy people, who were offered an experimental therapy, with unknown long-term side-effects, to protect them against an illness that has the same mortality rate as the flu. Sadly, their lives have now been ruined.
- It is normally considered a fundamental principal of medical ethics, to discontinue a clinical trial if significant harm is demonstrated from the treatment under investigation.
- So my last question is this: Is it medically ethical to continue this vaccine rollout, in view of the severity of these life altering side-effects, after just the first shot? In Lytton, BC, we have an incidence of 1 in 225 of severe life altering side-effects, from this experimental gene modification therapy.
I have also noticed that these vaccine induced side effects are going almost entirely unreported, by those responsible for the vaccine rollout. I am aware that this is often a problem, with vaccines in general, and that delayed side-effects after vaccines, are sometimes labelled as being “coincidences”, as causality is often hard to prove. However, in view of the fact that this is an experimental treatment, with no long-term safety data, I think that perhaps this issue should be addressed too.
Furthermore I have noticed, that the provincial vaccine injury reporting form, which was clearly designed for conventional vaccines, does not even have any place to report vaccine injuries of the nature and severity that we are seeing from this new mRNA therapy.
It is now clearly apparent with medical evidence from around the world, that the side-effect profiles of the various gene modification therapies against Covid-19, have been vastly understated by their manufacturers, who were eager to prove their safety.
Thank you for attention to this critically urgent public health matter.
Yours sincerely,
Dr. Charles Hoffe
Dr. Hoffee’s letter to his Congregation
April 2021
Dear brothers and sisters in Christ,
I greet you in the name of our Lord and Saviour Jesus Christ. For those of you who do not know me, I am a Christian family physician in Lytton, BC.
I have been rather concerned about the experimental Covid vaccines that are being rolled out at a rapid rate. The leader of the World Economic Forum, Claus Schwab, (author of the book, “ The Great Reset”), has declared that; “No one is safe, until everyone is vaccinated.” This intention has been echoed by many world leaders.
All previous coronavirus vaccine research following the SARS epidemic in 2002/3, in creating RNA or DNA vaccines against coronaviruses ended, because great harm was seen in the animal trials.
But with the appearance of COVID-19, the same technology was rapidly revamped, with different delivery systems. However this time, animal trials were not done, and the experiment was taken directly to the population at large, after limited short-term trials. The vaccines have been rolled out, with absolutely no long-term safety data. This is a global experiment, on the entire world’s population.
In my own medical practice, I now have 6 patients who are enduring long-term side-effects from these experimental therapies. They all indicate neurological damage, which is evolving. I suspect that it may be multiple sclerosis, or something along those lines. I have written to the Medical Health Officer, in charge of the vaccine rollout in the BC interior, to express my concerns and questions, with absolutely no response.
I therefore drafted an open letter to Dr Bonnie Henry, who is the Provincial Health Officer for British Columbia, to ask the same questions, and expressed the same concerns. I had been warned by my medical colleagues, not to expect a reply from her either. But to my complete astonishment, I received a prompt reply the next day inviting me to attend a virtual meeting, with a designated vaccine safety specialist. The meeting is scheduled for 4 pm (Pacific time) on Tuesday April 13, 2021.
Meanwhile I am sending urgent referrals, to a neurologist, to investigate my three most serious vaccine injured patients. My hope is that once we can identify what disease process has been initiated by this experimental gene therapy, we can raise public awareness more effectively.
So I have attached my open letter, to Dr Bonnie Henry, which documents my personal experience of the vaccine injuries in my own medical practice. Please feel free to share it with anyone who might feel tempted, to except this experimental vaccine, for a veneer of “safety”.
I invite you to join with me in prayer, in preparation for my meeting on Tuesday afternoon, that the Lord would guide my thoughts and words. I pray too, that the Lord would prepare the heart of the vaccine specialist that I will be speaking to, so that they take this matter very seriously. A global experiment on this scale, on uninformed participants who are driven by fear, is a crime against humanity.
All of the Covid vaccines are effectively genetic modification. They vary only in the mode of delivery. They all work, by introducing a gene to our bodies to manufacture an antibody against the Covid spike protein. The problem is, that there are 20 human tissue types that also have a spike protein. So there is a possibility that the Covid antibody may target one of our own human tissues too. In other words, that this new therapy will trigger an autoimmune reaction in some people.
There have been hundreds of reported miscarriages in pregnant women who have received the Covid vaccines. The placenta is one of the 20 tissue types that also has a spike protein. So it is most likely, that the cause of these miscarriages, is that these women, now have an antibody that targets placental tissue. They have effectively been vaccinated against any future pregnancy.
So if you know any woman of childbearing age, who is planning to receive a Covid vaccine, please warn her about this possibility, of permanent sterility, through recurrent miscarriage.
I request your prayers, and I very much hope that this information may be helpful to you and those dear to you. Please feel free to share it with anyone who might heed these warnings. I have attached my open letter to Dr Bonnie Henry. Please feel free to share it too.
May the Lord bless and keep you.
Dr Charles Hoffe

In June, Dr. Bret Weinstein interviewed Dr. Robert Malone, the inventor of mRNA vaccine technology, and Steve Kirsch, philanthropist and tech entrepreneur who has become a respected force in the quest to give voice to people who have been harmed by COVID vaccines.
The 3.5 hour “DarkHorse Podcast” interview was censored on YouTube and other major social media platforms. Five days after the DarkHorse podcast was published, Malone’s scientific accomplishments and contributions were scrubbed from Wikipedia.
Thanks to filmmaker Mikki Willis and his team for creating this 1-hour version of the original podcast exclusive for The Defender.
During the podcast, Malone, Weinstein and Kirsch touch on the implications of the controversial Japanese Pfizer biodistribution study, made public earlier this month by Dr. Byram Bridle, a viral immunologist.
The biodistribution study obtained by Bridle showed lipid nanoparticles from the vaccine did not stay in the deltoid muscle where they were injected as the vaccine’s developers claimed would happen, but circulated throughout the body and accumulated in large concentrations in organs and tissues, including the spleen, bone marrow, liver, adrenal glands and — in “quite high concentrations” — in the ovaries.
Malone also discusses the lack of proper animal studies for the new mRNA vaccines, and the theory, espoused by virologist Geert Vanden Bossche, Ph.D., that mass vaccination with the mRNA vaccines could produce ever more transmissible and potentially deadly variants.
Watch here:
Video is accessible only at the original website.


Life has to be our dedication, not virus eradication. We are custom designed biologically and perhaps providentially to transcend viral challenges and pathogens, when we use our immunological hardiness, our medical acumen and data-based (not hypochondriacal) prudence – Pic by Shehan Gunasekara
The popular narrative reeks so pungently that we almost have to keep debunking these absurdities to dispel the trance that too many seem to be under.
C-19: It’s novel, it’s new, it’s unprecedentedly dangerous!
No, it’s not! There is a family of coronaviruses. To that extent, this may have been ‘new’ and ‘novel, but not in any way to suggest that either our immune systems or our medical science was dealing with some uniquely implacable foe. Furthermore, it seems to have been circulating from the latter half of 2019. Medical researchers have repeatedly confirmed there were both examples of pre-existing immunity and crossover immunity due to prior immunological experience with similar pathogens. And now data clearly shows this was nothing unprecedented.
It is primarily spread by droplets and infected surfaces
No, it isn’t. It is an airborne virus, and flourishes in congested, poorly ventilated indoor spaces, and is spread by minute particles. Ergo, being ‘locked’ in is simply insane. Even the US CDC confirms, there is roughly 1 in 10,000 chance of being infected by touching a surface. So, all this mass sanitising and social distancing was more kabuki theatre than anything else.
Everyone is equally at risk!
No, they’re not! This is highly age stratified. Certainly, in the developed world, 93%+ of the deaths are above 70. There is a remarkably good recovery rate above 70, close to 97% for those without serious comorbidities. Another 6 to 10% fall within the ages of 40 to 69 (again, the majority with existing preconditions we are told by meta-analysts at leading universities) and below 40 the mortality rate gets increasingly nominal and infinitesimal.
There is no treatment
Yes, there is! There is, of course, the Nobel Prize winning, WHO essential drug, Ivermectin There are studies, randomised trials, overwhelming front line clinical experience from around the world all testifying to its saving graces. There is also HCQ and Zinc, Corticosteroids, Monoclonal Antibodies, Vitamin D3, Budesonide and numerous others that are part of demonstrably effective, early treatment protocols. If treated early during the viral stage, leading doctors in the US, UK, Zimbabwe, India, Mexico, South Africa confirm virtually every symptomatic patient can be saved.
Overall, even including the inflammation and thrombosis phase of the illness (when it becomes successively more dangerous) the most effective protocols have shown 85 to 90% reduction in hospitalisation and deaths. There is no sane reason not to embrace this, demonstrate it, and crystallise a Sri Lanka protocol drawing on the best of the rest.
Natural immunity cannot save us
Yes, it can! We would not be alive today if natural immunity did not work. Virtually all past vaccinations have taken place after a pandemic has waned somewhat because those actual vaccines did not get fast tracked past animal trials and safety trials.
Every credible study reconfirms our immunological wisdom has always trumpeted. Namely immunity is long lasting. And while there is no guarantee no one will ever get re-infected, even that is extremely rare, with virtually no documented global cases. And when it does happen, it is substantially milder and our immune memory in terms of mobilising to deal with the pathogen becomes ever more profound. And that, indeed, seems to last a lifetime.
Despite the seesawing medical vacillations of an increasingly confounded WHO, natural immunity trumps any vaccine-based immunity. And in the case of the current crop, the “vaccines” have been focused on suppressing symptoms and do not lead to the sustained immunological template that natural immunity confers (by their own admission). Despite this still being distorted in their description, at least natural immunity is back on the WHO website after having been pulled from there in an almost comic panic spasm.
Asymptomatic people drive the disease, and so, we must lock everyone up
They don’t and we shouldn’t! Asymptomatic transmission is a dud, has not been demonstrated to be in evidence except where people’s immune systems are naturally dealing with the infection, in which case, they are not transmitting. Children, for example, fall within this description, and have not been shown to be vectors of transmission. This has been shown both in open schools in Florida and in Sweden where they stayed open throughout.
Therefore, it may be necessary to revert to the unanimous pre 2020 consensus that said, ‘asymptomatic’ is really a euphemism for ‘healthy.’ Certainly ‘detecting’ an asymptomatic person based on highly fallible PCR testing is no basis to debunk centuries of medical consensus. Said PCR test anyway doesn’t test for live infectiousness, is not by itself (even as per WHO) diagnostic, and amplification settings are often set so high as to make the results almost a parody. And then lab contamination is often rife and viral debris can malinger long beyond any rational infection period. Other than that, we can swoon at its accuracy!
Ergo, locking up the healthy rather than allowing them to develop natural immunity if they are not in the vulnerable risk profile (which the majority are not) is oppressive, useless, society destroying and a form of protracted economic suicide.
Everyone should be masked!
No, they shouldn’t! In 2019 WHO had reviewed the 10 most seemingly credible mask studies, all of whom concluded masks don’t work in pandemic situations except in very crowded contexts and should not be used. This was also the conclusion up until the 2020 haemorrhage of medical sanity, of the US CDC, the European Medical Association, the Australian authorities, Johns Hopkins University and virtually everywhere else. There is no new research or any new studies that have led to this somersault. The only randomised trail done over this period, in Denmark, is consistent with all the earlier studies.
Dr. Frankenstein Fauci in his highly vocal emails disdains the use of such masks as well. The nano particles are too small for the masks to arrest anything. Anything other than respirators fitted to the face, which are not practical beyond a few hours, allow ready access to viral invaders, as we’ve said before. This is why one doesn’t use such masks to protect against anthrax, asbestos, black mould, all of which have larger particles.
Masks are unhygienic, suppress oxygen flow, force you to inhale your own waste, and there are no long-term studies that demonstrate any efficacy or even confirm the safety of breathing in and out in such an encased, inhibited manner for a protracted period of time. Moreover, there’s the simple “live” case study of comparing open US states without mask mandates with those that are ‘muzzled,’ and one can see that there is no benefit in terms of mortality and overall results (on the contrary), other than totemic compliance and pathetic virtue signalling.
By the way, there is not one recorded instance of outdoor transmission (even CDC accepts it is less than 1%). Therefore, unless you dislike breathing in oxygen there truly is no explanation for the endurance of this mad, sad ritual, when we are outside.
Variants will haunt us forever
Who cares? Can we make our peace with the fact that viruses mutate? As explained before, former Chief Science Officer of Pfizer, Dr. Michael Yeadon, has pointed out that a variant is no more than 0.3% different than the original virus. And since we know immune systems that were earlier exposed (as Dr. Yeadon points out through medical testing), still recognise and immunologically rally when exposed again to the original SARS from 17 years ago – even though that is 20% different than SARS-CoV-2 – we can see how little we have to fear. These variants are simply the currently dominant strain, not some unknown predator.
The current scaremonger, Delta, is actually welcomed by specialists like Dr. Harvey Risch of Yale and Dr. Peter McCullough of Baylor because it is so mild relative to mortality, and they say, among the most treatable variants they’ve encountered. So, despite PCR test spasms showing ‘surging cases,’ there has been virtually no impact on mortality. In fact, J.P. Morgan reports that in 10 out of 15 countries where Delta is dominant, even cases declined, and in 13 out of 15 countries, fatalities declined with vaccination percentages ranging from 32 to 63% of the population.
Even in the UK which has seen an uptick in mortality, as per government data, the case fatality rate hovers close to 0.3%
We must vaccinate everybody!
Actually, we need great caution! There are numerous early treatments. On that basis alone, the Emergency Use Authorisation (EUA) should be rendered illicit and inapplicable (this is why there are such desperate attempts to suppress and smear these treatments). So, the deaths and adverse effects recorded even in government databases (which confess to being between 1-20% of actuals) are greater than the cumulative total for all other vaccines since such tracking was undertaken, at least since 1995.
The types of issues range from severe neurological damage, myocarditis, life threatening blood clots, fertility issues, tragic pregnancy consequences and too many others to itemise or catalogue. To this, a riposte is often given that these adverse effects correlate to vaccination but cannot be proven to have been ‘caused’ by the vaccine.
But repeated conjunction between a stimulus (‘vaccines’) and a pattern of adverse phenomena closely accompanying all the vaccines, is precisely what, in more prudent and more transparent times, would simply, on the basis of the precautionary principle, lead to stopping this manic jabbing, to do a proper investigative assessment.
Beyond that we now know that the spike proteins, even without the virus, are lethal and this is what we are injecting in the case of the mRNA vaccines primarily. They also do not stay localised and instead spread throughout our organs (SALK Institute study, autopsy plus repeated testimony by Dr Robert Malone, one of the founders of the mRNA technology – who has for the sin of sharing his expertise, had both his LinkedIn account erased and has had Wikipedia attempt to rewrite history by expunging his mRNA contribution from their site). These are horrifying concerns, and it is monstrous not to have addressed them, rather than cravenly attempting to whitewash them.
The spectre of censorship
There are great concerns re the pervasive censorship. Such desperate attempts to silence and muzzle don’t usually spring from confidence, or positions that have self-evident appeal. Just a smattering of examples: Norway was de-platformed from Tweeting disquiet about Astra Zeneca! Dr. Robert Malone, as indicated above, has accounts cancelled, and is removed from the Wikipedia author page (Joan of Arc may be next).
Evolutionary biologist and visiting fellow at Princeton (Bret Weinstein) “demonetised” from YouTube (after over three million views) because some cabal somewhere, somehow decide what is or isn’t fit for our eyes and ears. And when and how did that judgment seat pass to them, otherwise than through financial string pulling by desperate vested interests, thereby confessing their impotence in terms of having a case to make?
Noble Prize Winner Professor Satoshi Omura, whose discovery of Ivermectin as an anti-parasitic drug led to one of the world’s greatest public health achievements, was just censored for daring to opine that indeed he believes his discovery will be hugely beneficial for COVID treatment.
None of this is normal! Martin Kulldorff, one of the world’s leading epidemiologists, at a meeting with Florida Governor De Santis suggests that universal vaccination is not called for, the interview is scrubbed immediately, because our precious sensibilities cannot even have that “suggested”, even from someone whose expertise fully entitles him to share an assessment we should be desperately interested to at least consider.
Remember, all this is being mounted over an age stratified illness of low risk to virtually everyone. So, all the frenzy to demonise, the incentive for that, once more, cannot have been public health.
Yes, four million people are purported to have died of COVID with all types of death certificate rigging. And if you say it’s normal for a positive test on a death certificate to translate into causation (and nothing of course re vaccine deaths can rise to “causation” unless a spike protein jumped out and confessed perhaps), I will ask why this logic is only, uniquely applied to this pathogen? Why were these norms so hurriedly “updated” after decades of normal causal logic holding sway, of recording the primary cause of death?
Yes, four million died over this period, and five million die of all-cause mortality every month, so about 85 million have perished over the same period. There is no interest in the other causes of mortality? Or those coming from deferred cancer screenings, heart conditions not attended to, overdoses and suicides, literally many millions more from starvation due to interrupted supply chains?
Re-opening society: A call to action
We had three of the world’s most eminent doctors present to policy makers here, and the conclusions in terms of re-opening society and keeping it open are given below.
-
Keep society open, solvent, functioning and able to provide public health resources to its citizens as well as livelihoods. Lockdowns are penal, take a devastating human toll which only worsens, and as demonstrated, backfire, and data shows that conclusively around the world. They do not help given all transmission is indoor, most people are not at risk, and abundant early treatments exist for the symptomatic.
-
Keep people out of hospitals by providing early treatment, open air clinics, mobile clinics. If treatment is given early on, the period of infectiousness can be vastly reduced to as little as five days. Home treatment guides can be provided and contact information for resources that can provide telemedicine, drive by clinics, guidance, treatment and early support, should be widely circulated. We can actively benchmark experience with everything from ivermectin to monoclonal antibodies (now cleared for use in Sri Lanka through Roche) to protocols in South Africa by Dr. Chetty (4,000 patients, everyone has survived), including fascinating local remedies in Tamil Nadu that actually work. And thereby, as cited above, we can create a “Lankan protocol.”
-
Consider augmenting conventional PCR tests which have time lags as well as often not being able to confirm live infectiousness with some of the newer saliva-based antigen tests, some of which now have demonstrated 98% accuracy and can report results in 15 minutes, or as Singapore is suggesting, focus on the symptomatic and do proper lab diagnosis. Regardless though, focus on the mortality needle, not ‘positive tests’ posing as ‘cases’ as per the example of Sweden this spring (rising positive tests with consistently falling death numbers due to focused protection). Singapore is another example of this “disconnect” with 62,000 positive tests and 36 deaths.
-
Prioritise the vulnerable elderly in any vaccination efforts as well as in terms of temporary sheltering in place or other measures to shield them from infection when community disease spread is high.
-
Ensure people are encouraged when indoors to be in not overly congested, well ventilated spaces, especially the elderly and vulnerable. And also, to get plenty of time outdoors, UV rays and vitamin D from the sun, germicidal air as epidemiologist Knutt Wittowski stresses are well documented benefits with all viruses in synch with seasonality and plenty of exercise which helps the immune system and improves indicators re other aspects of health, including comorbidities.
-
Please note Sri Lanka still has among the lowest deaths per million in the world, (roughly 156 per million). Pakistan has a fairly low deaths per million (roughly 102 per million) and even India, despite its recent surge has roughly 1/7th the deaths per million of the US and Europe. We should take advantage of being in this relatively charmed immunological corridor and find the will and courage to open society up, let natural immunity among those at nominal risk (based on age first and overall health next) help to build a wall of immunity and treat everyone with symptoms who needs help as early as possible, thereby fast-tracking C-19 migrating to endemic status. This was the overall consensus of our global panel.
Of possible concern
As we open our borders or open society back up (which we must), or have another seasonal surge, if we stay infatuated with positive tests rather than symptoms, we may again panic unnecessarily. We should recall, positivity in Delhi in early May was staggering and by week of 31 May was less than 1% which shows how quickly the tide can turn.
Knowing we have this suite of treatments and prioritising the vulnerable for treatment and/or vaccination will assure us that even if there is a temporary surge, focusing on the symptomatic, we can handle it and there is nothing to fear. The alternative is perpetual, recurring, pointless lockdowns and having to act as if no other cause of harm or concern matters even though we lose many more lives here through car accidents, diabetes, heart attacks, in some seasons, dengue. Hunger, bankruptcy, deferred vaccinations for even more serious diseases that we were on our way to routing, destruction of education for children for whom it is their literal future, simply cannot be ignored as we chase, to the exclusion of all else, the unattainable phantom of ‘zero COVID’.
Life has to be our dedication, not virus eradication. We are custom designed biologically and perhaps providentially to transcend viral challenges and pathogens, when we use our immunological hardiness, our medical acumen and data-based (not hypochondriacal) prudence.
28th June 2021
“The lamps are going out all over Europe, we shall not see them lit again in our life-time.” Edward Grey
Several years ago, I wrote a book called Doctoring Data. It was my attempt to help people navigate their way through medical headlines and medical data.
One of the main reasons I was stimulated to write it, is because I had become deeply concerned that science, especially medical science, had been almost fully taken over by commercial interests. With the end result that much of the data we were getting bombarded with was enormously biased, and thus corrupted. I wanted to show how some of this bias gets built in.
I was not alone in my concerns. As far back as 2005, John Ioannidis wrote the very highly cited paper ‘Why most Published Research Findings are False’. It has been downloaded and read by many, many, thousands of researchers over the years, so they can’t say they don’t know:
‘Moreover for many current scientific fields, claimed research findings may often be simply accurate measures of the prevailing bias.’1
Marcia Angell, who edited the New England Journal of Medicine for twenty years, wrote the following. It is a quote I have used many times, in many different talks:
‘It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.’
Peter Gotzsche, who set up the Nordic Cochrane Collaboration, and who was booted out of said Cochrane collaboration for questioning the HPV vaccine (used to prevent cervical cancer) wrote the book. ‘Deadly Medicine and Organised Crime. [How big pharma has corrupted healthcare]’.
The book cover states… ‘The main reason we take so many drugs is that drug companies don’t sell drugs, they sell lies about drugs… virtually everything we know about drugs is what the companies have chosen to tell us and our doctors… if you don’t believe the system is out of control, please e-mail me and explain why drugs are the third leading cause of death.’
Richard Smith edited the British Medical Journal (BMJ) for many years. He now writes a blog, amongst other things. A few years ago, he commented:
‘Twenty years ago this week, the statistician Doug Altman published an editorial in the BMJ arguing that much medical research was of poor quality and misleading. In his editorial entitled ‘The scandal of Poor Medical Research.’ Altman wrote that much research was seriously flawed through the use of inappropriate designs, unrepresentative sample, small sample, incorrect methods of analysis and faulty interpretation… Twenty years later, I feel that things are not better, but worse…
In 2002 I spent eight marvellous weeks in a 15th palazzo in Venice writing a book on medical journals, the major outlets for medical research, and the dismal conclusion that things were badly wrong with journals and the research they published. My confidence that ‘things can only get better’ has largely drained away.’
Essentially, medical research has inexorably turned into an industry. A very lucrative industry. Many medical journals now charge authors thousands of dollars to publish their research. This ensures that it is very difficult for any researcher, not supported by a university, or a pharmaceutical company, to afford to publish anything, unless they are independently wealthy.
The journals then have the cheek to claim copyright, and charge money to anyone who actually wants to read, or download the full paper. Fifty dollars for a few on-line pages! They then bill for reprints, they charge for advertising. Those who had the temerity to write the article get nothing – and nor do the peer reviewers.
It is all very profitable. Last time I looked the Return on Investment (profit) was thirty-five per-cent for the big publishing houses. It was Robert Maxwell who first saw this opportunity for money making.
Driven by financial imperative, the research itself has also, inevitably, become biased. He who pays the paper calls the tune. Pharmaceutical companies, food manufacturers and suchlike. They can certainly afford the publication fees.
In addition to all the financial and peer-review pressure, if you dare swim against the approved mainstream views you will, very often, be ruthlessly attacked. As many people know, I am a critic of the cholesterol hypothesis, along with my band of brothers…we few, we happy few. In the 1970s, Kilmer McCully, who plays double bass in our band, was looking into a cause of cardiovascular disease that went against the mainstream view. This is what happened to him:
‘Thomas N. James, a cardiologist and president of the University of Texas Medical Branch who was also the president of the American Heart Association in 1979 and ’80, is even harsher [regarding the treatment of McCully]. ”It was worse than that – you couldn’t get ideas funded that went in other directions than cholesterol,” he says. ”You were intentionally discouraged from pursuing alternative questions. I’ve never dealt with a subject in my life that elicited such an immediate hostile response.”
It took two years for McCully to find a new research job. His children were reaching college age; he and his wife refinanced their house and borrowed from her parents. McCully says that his job search developed a pattern: he would hear of an opening, go for interviews and then the process would grind to a stop. Finally, he heard rumors of what he calls ”poison phone calls” from Harvard. ”It smelled to high heaven,” he says.’
McCully says that when he was interviewed on Canadian television after he left Harvard, he received a call from the public-affairs director of Mass. General. ”He told me to shut up,” McCully recalls. ”He said he didn’t want the names of Harvard and Mass. General associated with my theories.’ 2
More recently, I was sent a link to an article outlining the attacks made on another researcher who published a paper which found that being overweight meant having a (slightly) lower risk of death than being of ‘normal weight. This, would never do:
‘A naïve researcher published a scientific article in a respectable journal. She thought her article was straightforward and defensible. It used only publicly available data, and her findings were consistent with much of the literature on the topic. Her coauthors included two distinguished statisticians.
To her surprise her publication was met with unusual attacks from some unexpected sources within the research community. These attacks were by and large not pursued through normal channels of scientific discussion. Her research became the target of an aggressive campaign that included insults, errors, misinformation, social media posts, behind-the-scenes gossip and maneuvers, and complaints to her employer.
The goal appeared to be to undermine and discredit her work. The controversy was something deliberately manufactured, and the attacks primarily consisted of repeated assertions of preconceived opinions. She learned first-hand the antagonism that could be provoked by inconvenient scientific findings. Guidelines and recommendations should be based on objective and unbiased data. Development of public health policy and clinical recommendations is complex and needs to be evidence-based rather than belief-based. This can be challenging when a hot-button topic is involved.’ 3
Those who lead the attacks on her were my very favourite researchers, Walter Willet and Frank Hu. Two eminent researchers from Harvard who I nickname Tweedledum and Tweedledummer. Harvard itself has become an institution, which, along with Oxford University, comes up a lot in tales of bullying and intimidation. Willet and Hu are internationally known for promoting vegetarian and vegan diets. Willet is a key figure in the EAT-Lancet initiative.
Where is science in all this? I feel the need to state, at this point, that I don’t mind attacks on ideas. I like robust debate. Science can only progress through a process of new hypotheses being proposed, being attacked, being refined and strengthened – or obliterated. But what we see now is not science. It is the obliteration of science itself:
‘Anyone who has been a scientist for more than 20 years will realize that there has been a progressive decline in the honesty of communications between scientists, between scientists and their institutions and the outside world.
Yet, real science must be an area where truth is the rule; or else the activity simply stops being scient and becomes something else: Zombie science. Zombie science is a science that is dead, but is artificially keep moving by a continual infusion of funding. From a distance Zombie science looks like the real thing, the surface features of a science are in place – white coats, laboratories, computer programming, PhDs, papers, conferences, prizes etc. But the Zombie is not interested in the pursuit of truth – its citations are externally-controlled and directed at non-scientific goals, and inside the Zombie everything is rotten…
Scientists are usually too careful and clever to risk telling outright lies, but instead they push the envelope of exaggeration, selectivity and distortion as far as possible. And tolerance for this kind of untruthfulness has greatly increased over recent years. So, it is now routine for scientists deliberately to ‘hype’ the significance of their status and performance and ‘spin’ the importance of their research.’ Bruce Charlton: Professor of Theoretical Medicine.
I was already pretty depressed with the direction that medical science was taking. Then COVID19 came along, the distortion and hype became so outrageous that I almost gave up trying to establish what was true, and was just made up nonsense.
For example, I stated, right at the start of the COVID19 pandemic, that vitamin D could be important in protecting against the virus. For having the audacity to say this, I was attacked by the fact checkers. Indeed, anyone promoting vitamin D to reduce the risk of COVID19 infection, was ruthlessly hounded.
Guess what. Here from 17th June:
‘Hospitalized COVID-19 patients are far more likely to die or to end up in severe or critical condition if they are vitamin D-deficient, Israeli researchers have found.
In a study conducted in a Galilee hospital, 26 percent of vitamin D-deficient coronavirus patients died, while among other patients the figure was at 3%.
“This is a very, very significant discrepancy, which represents a big clue that starting the disease with very low vitamin D leads to increased mortality and more severity,” Dr. Amir Bashkin, endocrinologist and part of the research team, told The Times of Israel.’ 4
I also recommended vitamin C for those already in hospital. Again, I was attacked, as has everyone who has dared to mention COVID19 and vitamin C in the same sentence. Yet, we know that vitamin C is essential for the health and wellbeing of blood vessels, and the endothelial cells that line them. In severe infection the body burns through vitamin C, and people can become ‘scrobutic’ (the name given to severe lack of vitamin C).
Vitamin C is also known to have powerful anti-viral activity. It has been known for years. Here, from an article in 1996:
‘Over the years, it has become well recognized that ascorbate can bolster the natural defense mechanisms of the host and provide protection not only against infectious disease, but also against cancer and other chronic degenerative diseases. The functions involved in ascorbate’s enhancement of host resistance to disease include its biosynthetic (hy-droxylating), antioxidant, and immunostimulatory activities. In addition, ascorbate exerts a direct antiviral action that may confer specific protection against viral disease. The vitamin has been found to inactivate a wide spectrum of viruses as well as suppress viral replication abd expression in infected cell.’ 5
I like quoting research on vitamins from way before COVID19 appeared, where people were simply looking at Vitamin C without the entire medico-industrial complex looking over their shoulder, ready to stamp out anything they don’t like. Despite a mass of evidence that Vitamin C has benefits against viral infection, it is a complete no-go area and no-one even dares to research it now. Facebook removes any content relating to Vitamin C and COVID19.
As of today, any criticism of the mainstream narrative is simply being removed. Those who dare to raise their heads above the parapet, have them chopped off:
‘Dr Francis Christian, practising surgeon and clinical professor of general surgery at the University of Saskatchewan, has been immediately suspended from all teaching and will be permanently removed from his role as of September.
Dr Christian has been a surgeon for more than 20 years and began working in Saskatoon in 2007. He was appointed Director of the Surgical Humanities Program and Director of Quality and Patient Safety in 2018 and co-founded the Surgical Humanities Program. Dr. Christian is also the Editor of the Journal of The Surgical Humanities.
On June 17th Dr Christian released a statement to over 200 of his colleagues, expressing concern over the lack of informed consent involved in Canada’s “Covid19 vaccination” program, especially regarding children.
To be clear, Dr Christian’s position is hardly an extreme one.
He believes the virus is real, he believes in vaccination as a general principle, he believes the elderly and vulnerable may benefit from the Covid “vaccine”… he simply doesn’t agree it should be used on children, and feels parents are not being given enough information for properly informed consent.’ 6
When I wrote Doctoring Data, a few years ago, I included the following thoughts about the increasing censorship and punishment that was already very clearly out in the open:
…where does it end? Well, we know where it ends.
First, they came for the communists, and I didn’t speak out because I wasn’t a communist
Then they came for the socialists, and I didn’t speak out because I wasn’t a socialist
Then they came from the trade unionists, and I didn’t speak out because I wasn’t a trade unionist
Then they came for me, and there was no-one left to speak for me
Do you think this is a massive over-reaction? Do I really believe that we are heading for some form of totalitarian stated, where dissent against the medical ‘experts’ will be punishable by imprisonment? Well, yes, I do. We are already in a situation where doctors who fail to follow the dreaded ‘guidelines’ can be sued, or dragged in front the General Medical Council, and struck of. Thus losing their job and income…
Where next?
The lamps are not just going out all over Europe. They are going out, all over the world.
1: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.0020124
2: https://www.nytimes.com/1997/08/10/magazine/the-fall-and-rise-of-kilmer-mccully.html
3: https://www.sciencedirect.com/science/article/pii/S0033062021000670
5: https://www.researchgate.net/publication/14383321_Antiviral_and_Immunomodulatory_Activities_of_Ascorbic_Acid 6: https://off-guardian.org/2021/06/25/canadian-surgeon-fired-for-voicing-safety-concerns-over-covid-jabs-for-children/
The vaccines are reflexively and repeatedly declared "tested, safe and effective".
The document you can read by clicking the Download button at this regulations.gov web page, lists the very large number of untested questions left out of that "tested" assertion.
3rd June 2021
When COVID19 came along I was in the midst of writing my latest book on heart disease. What causes it – and what does not.
One section I was working on covers the wide range of conditions known as the vasculitis(es). I could immediately see a whole series of connections between COVID19, spike proteins, the immune system and blood clots. Some of which are deeply concerning, for reasons that should become apparent.
Before getting started, you can see an immediate problem here is there does not seem to be a plural form of vasculitis. A bit like octopus. You can have one octopus, but what happens then… two octupuses… or is it two octopi? Wars have been fought over less.
Anyway, a vasculitis is a condition whereby a factor, of some sort, causes damage to the vascular system. The vascular system being, essentially, the blood vessels and the heart. The suffix itis simplymeans inflammation. As in appendicitis, or tonsillitis. Or, in this case vasculitis.
There are many different vasculitis(es) or vasculiti? They range from Kawasaki’s disease to antiphospholipid syndrome, rheumatoid arthritis, scleroderma, Sjogren’s disease and suchlike. They are many, and varied, and quite fascinating. At least they are, to me.
In all of them you have two things in common… that are most relevant to this discussion. First, with any form of vasculitis, the body decides to attack the lining of the blood vessels – causing inflammation and damage. Second, the rate of death from cardiovascular disease goes up dramatically. In some cases, a fifty-fold increase. This was seen in young women with Systemic Lupus Erythematosus (SLE) with additional antiphospholipid syndrome1.
Why does the body decide to attack itself? This is a good question that I cannot really answer. If I could, I would be claiming my Nobel prize, right now. However, I can say that, for various reasons, the immune system makes the decision that it doesn’t like something about the lining of the blood vessels and believes it to have become ‘alien’ in some way. It then proceeds to attack. Which does not answer the question as to exactly why the attack happens? But it does tell you a bit about what happens.
Another major problem with vasculitis is that blood clots spring to life throughout the vascular system. This is because the blood is always ready to clot, at any time, and if you take away some of vital the anti-clotting mechanisms, the balance will be tilted firmly towards coagulation.
One of the most powerful anti-clotting mechanisms/systems is the protective layer that lines your entire vascular system, known as the glycocalyx. This is made up of glycoproteins (glucose and proteins stuck together). Under an electron microscope the glycocalyx looks like a tiny forest, or a badly mown lawn.
Many fish are covered with glycocalyx, which makes them very slippery, and difficult to get hold of. The glycocalyx also stops bacteria and viruses from gaining entry, in both fish and humans.
In your blood vessels, the glycocalyx protrudes out from endothelial cells, the cells that line all your blood vessels, and into the bloodstream. The layer of glycocalyx contains many, many, anticoagulant factors. Below is a short list of all the things the glycocalyx does:
The glycocalyx:
- Forms the interface between the vessel wall and moving blood.
- Acts as the exclusion zone between blood cells and the endothelium.
- Acts as a barrier against leakage of fluid, proteins and lipids across the vascular wall.
- Interacts dynamically with blood constituents.
- Acts as the “molecular sieve” for plasma proteins.
- Modulates adhesion of inflammatory cells and platelets to the endothelial surface.
- Functions as a sensor and mechano-transducer of the fluid shear forces to which the endothelium is exposed; thus, the glycocalyx mediates shear-stress-dependent nitric oxide production.
- Retains protective enzymes (e.g., superoxide dismutase).
- Retains anticoagulation factors, e.g.: Tissue factor inhibitor, Protein C, Nitric Oxide (NO), Antithrombin.
Complicated stuff – that hardly anyone has ever heard of.
Anyway, if you damage the glycocalyx, or damage the underlying endothelial cells that synthesizes the glycocalyx layer, you will tip the balance very strongly towards the creation of blood clots. These can then then stick to the artery, or vein, wall. Sometimes they will fully block a blood vessel, leading to such things as a stroke or heart attack.
The interaction between vasculitis and thrombosis has been a relatively unexplored area of medicine. But it remains critically important in many diseases:
‘The relationship between inflammation and thrombosis is not a recent concept, but it has been largely investigated only in recent years. Nowadays inflammation-induced thrombosis is considered to be a feature of systemic autoimmune diseases such as Systemic Lupus Erythematosus (SLE), Rheumatoid Arthritis (RA), or Sjogren’s Syndrome (SS)2.
In super-short version. If you damage the lining of blood vessel walls, blood clots are far more likely to form. Very often, the damage is caused by the immune system going on the attack, damaging blood vessel walls, and removing several of the anti-clotting mechanisms.
Sepsis
Moving sideways for a moment. There are other things that can damage the blood vessel wall, leading to widespread blood clot formation. One of them is the condition known as sepsis. Which used to be called blood poisoning.
In sepsis, bacteria gain entry to the bloodstream through such things as a cut, an insect bite, a severe urine infection, and suchlike. When bacteria get into the blood, and start multiplying, they release exotoxins. Which are, effectively, the waste products of the bacteria.
These exotoxins then attack blood vessel walls, damaging the glycocalyx and endothelial cells. This drives the formation of blood clots throughout the body. The medical term for this is disseminated intravascular coagulation (DIC) = widespread blood clots in the vascular system.
The attacks not only cause clots, they can also cause the smaller blood vessels to weaken and burst. Which is why one sign of an infection with the meningococcal bacteria (the one that causes meningitis), is a rash. The rash is made up of dark, almost black, bruises. Once these start to appear, things are very bad. Potentially fatal, it means blood vessels are under severe attack and are breaking apart. Creating both bleeding and clots.
In truth, the ‘rash’ in meningitis is not really a rash at all. It is a sign of underlying, severe, vasculitis. The individual small bruises can also be called petechiae. Just to be scientific.
Another sign of widespread blood vessel damage, with the formation of multiple blood clots, is that the level of platelets in the bloodstream falls dramatically. For those who have never heard of such things, platelets are small cells that float about in the bloodstream. Their primary role is to co-ordinate the blood clotting system. If a red blood cell was the size of the Earth, a platelet would be about this size of the Moon.
If there is damage to blood vessels, platelets fling themselves at the area, and stick together to form a solid plug. They also release chemicals and enzymes that cause fibrin to be formed. Fibrin is the long sticky strand of protein that binds clots tightly together. Platelets also drag in red blood cells, and suchlike to make bigger and tougher clots. They have been called the conductors of the clotting orchestra.
In the process of doing all of these things, the number of platelets starts to fall. This is not surprising, as they are being used up to make blood clots/thrombi. Which means that one sign of widespread clot formation is a fall in the level of platelets (thrombocytopenia). This reliable sign of widespread coagulation, or disseminated intravascular coagulation (DIC).
Time for a quick re-cap.
What do we know?
What we now know, on the journey towards COVID19, are three important things.
- If you damage the endothelial cells/glycocalyx, blood clots will form and stick to the side of blood vessels.
- Damage is often caused by immune system attack.
- Falling platelet levels are a sign of widespread blood clotting.
COVID19
What do we know about COVID19? First, it can only enter cells that have a receptor known as the angiotensin II receptor (ACE2 receptor). Cells with these receptors are mainly found in the lining of the lungs, and endothelial cells that line all blood vessels. Also, the epithelial /endothelial cells than line the intestines. If a cell does not have an ACE2 receptor, COVID19 simply cannot gain entry.
This was known years ago, when SARS-CoV was identified, the precursor of SARS-Cov2. Here from a paper in 2004:
‘The most remarkable finding was the surface expression of ACE2 protein on lung alveolar epithelial cells and enterocytes of the small intestine. Furthermore, ACE2 was present in arterial and venous endothelial cells and arterial smooth muscle cells in all organs studied. In conclusion, ACE2 is abundantly present in humans in the epithelia of the lung and small intestine, which might provide possible routes of entry for the SARS-CoV. This epithelial expression, together with the presence of ACE2 in vascular endothelium, also provides a first step in understanding the pathogenesis of the main SARS disease manifestations3.’
So, SARS-CoV gets into the body through the lungs and bowels. These are the places where the virus can gain access because it is where ACE2 receptors can mainly be found. Of course, SARS-Cov2 gets into the body in exactly the same way.
What happens once SARS-Cov2 gets into cells? Well, it does what all viruses do. It takes over various cellular mechanisms and forces the cell to produce more SARS-CoV2 viruses. This then kills, or severely damages those cells. This mainly occurs when ‘virions’ start to escape from within the cell. This damages the cell membrane, and in some cases can cause the cell to burst apart.
Essentially, SARS-Cov2 starts by damaging endothelial cells in the lungs, because it usually arrives here first. Fluid is released, and there is the breakdown of small blood vessels in the lungs, and the small airways. In this situation, the lungs begin to fail, and oxygen levels in the blood can fall dramatically.
Infection can also cause diarrhoea, as the epithelial cells in the intestines are damaged. To quote from ‘the COVID19 symptoms’ study:
‘We think COVID-19 causes diarrhoea because the virus can invade cells in the gut and disrupt its normal function 4.’
As far as I know, no-one has died of COVID19 diarrhoea. However, COVID19 can create such severe lung damage that people have died from respiratory failure or lung damage… call this form of disruption what you will. However, many/most people survive this phase.
It is what happens next that that kills the majority of people who become severely infected.
What happens next is that SARS-Cov2 gets into the bloodstream. It then invades endothelial cells, also pericytes and myocytes in the heart. Both of which have a high level of ACE2 receptors. Both of which are kind of vital for heart function 5,6.
Then…
What we now have is a major widespread vasculitis on our hands, with severe endothelial cell damage and disruption and damage to the glycocalyx. Blood clots, blood clots, blood clots, everywhere.
‘Coronavirus disease 2019 (COVID-19) causes a spectrum of disease; some patients develop a severe proinflammatory state which can be associated with a unique coagulopathy and procoagulant endothelial phenotype. Initially, COVID-19 infection produces a prominent elevation of fibrinogen and D-dimer/fibrin(ogen) degradation products. This is associated with systemic hypercoagulability and frequent venous thromboembolic events. The degree of D-dimer elevation positively correlates with mortality in COVID-19 patients. COVID-19 also leads to arterial thrombotic events (including strokes and ischemic limbs) as well as microvascular thrombotic disorders (as frequently documented at autopsy in the pulmonary vascular beds). COVID-19 patients often have mild thrombocytopenia* and appear to have increased platelet consumption, together with a corresponding increase in platelet production.7’
*a low level of platelets
The spike protein
Then, of course, we have the spike protein to consider. If this is the thing that the immune system recognises and attacks – which it almost certainly is – then cells which are growing SARS-Cov2 inside them, which then express the spike protein on their surface as the virions escape, will be identified as ‘the enemy’.
At which point, the immune system will start to attack the endothelium (and glycocalyx) in an attempt to wipe out the virus. This will tend to happen two or three weeks after the initial infection (sometimes sooner). This is after the immune system has had a real chance to identify the spike protein, then properly wind itself up to produce antibodies against it. This is the time of maximum attack on the endothelium.
This moment is often referred to as a cytokine storm. A point where every system in the immune system gets revved up and charges into action. At one point I wasn’t sure if I really believed in the cytokine storm. But I do now think it is a real thing. It is almost certainly why steroids (which very powerfully reduce the immune response) have been found to reduce mortality in severely ill patients.
All of which means it may well be the body’s own infectious disease defence system that creates much of the damage to the cardiovascular system. Not necessarily the virus itself.
Alternatively, it may be that the spike protein itself creates most of the blood clots. Here from the paper ‘SARS-CoV-2 spike S1 subunit induces hypercoagulability.’
‘When whole blood was exposed to spike protein even at low concentrations, the erythrocytes (red blood cells) showed agglutination, hyperactivated platelets were seen, with membrane spreading and the formation of platelet-derived microparticles8.’
Translation. Introduce SARS-CoV2 spike proteins into bloodstream, and it makes it clot – fast. Which is a worry.
Vaccines
It is a worry because the entire purpose of vaccination against SARS-Cov2 is to force cells to manufacture the spike protein(s) and then send them out into the bloodstream.
So, quick recap again, what do we know?
We know that a very high percentage of the people who die following a COVID19 infection, die as result of blood clots. We also know that they can also suffer severe myocarditis (inflammation of the heart muscle), and suchlike.
We know that the spike protein can stimulate blood clots all by itself.
We know that the immune system attack on ‘alien’ proteins, such as the spike protein, can cause vasculitis.
We know that vaccines are designed to drive the rapid production of spike proteins that will enter the blood stream specifically to encounter immune cells, in order to create a powerful response that will lead to ‘immunity’ against future SARS-CoV2 infection.
We know that a number of people have died from blood clots following vaccination. To quote from the European Medicines Agency website report on the AZ COVID19 vaccine:
‘The PRAC (pharmacovigilance risk assessment committee) noted that the blood clots occurred in veins in the brain (cerebral venous sinus thrombosis, CVST) and the abdomen (splanchnic vein thrombosis) and in arteries, together with low levels of blood platelets and sometimes bleeding 9.’
This was all pretty much predictable, if you understood what was going with SARS-CoV – nearly seventeen years ago.
My concern at this point is that, yes, we have identified very rare manifestations of blood clotting: cerebral venous sinus thrombosis (CVST) and splanchnic (relating to the internal organs or viscera) vein thrombosis (SVT). These are so rare that it is unlikely that anything else – other than a novel vaccine – could have caused them. I have never seen a case and I had never even heard of them before COVID19 came along. And I have spent years studying the blood coagulation system, and vasculitis, and suchlike.
So, if someone is vaccinated, then has a cerebral venous sinus thrombosis, or a splanchnic vein thrombosis, this is almost certainly going to be noted and recorded – and associated with the vaccination. Fine.
However, if there is an increase in vanishingly rare blood clots, could there also be an increase in other, far more common blood clots at the same time. If this was the case, then it would be far more difficult to spot this happening.
Millions and millions of people suffer strokes and heart attacks every year. Millions more suffer deep vein thrombosis and pulmonary emboli. In fact, around the world, tens of millions die each and every year as a result of a blood clots forming somewhere in the body.
That is a hell of a lot of background blood clotting noise. Which means that it could be extremely difficult to disentangle cause and effect, especially if you are not looking. If an elderly person is vaccinated, then dies of a stroke a couple of weeks later. What caused the blood clot that led to the stroke? It is unlikely that any doctor would record this as a post-vaccine adverse event.
To give you one example of the difficulty of disentangling cause and effect, when you are looking at very common events, a few years ago Merck launched a drug called Vioxx (an anti-inflammatory like ibuprofen, or naproxen but not exactly the same class of drug). It didn’t go well. Here from the article ‘Merck Manipulated the Science about the Drug Vioxx.’
‘To increase the likelihood of FDA (Food and Drug Administration) approval for its anti-inflammatory and arthritis drug Vioxx, the pharmaceutical giant Merck used flawed methodologies biased toward predetermined results to exaggerate the drug’s positive effects. Internal documents made public in litigation revealed that a Merck marketing team had developed a strategy called ADVANTAGE (Assessment of Differences between Vioxx And Naproxen To Ascertain Gastrointestinal tolerability and Effectiveness) to skew the results of clinical trials in the drug’s favor.
As part of the strategy, scientists manipulated the trial design by comparing the drug to naproxen, a pain reliever sold under brand names such as Aleve, rather than to a placebo.’
The scientists highlighted the results that naproxen decreased the risk of heart attack by 80 percent, and downplayed results showing that Vioxx increased the risk of heart attack by 400 percent. This misleading presentation of the evidence made it look like naproxen was protecting patients from heart attacks, and that Vioxx only looked risky by comparison. In fact, Vioxx has since been found to significantly increase cardiovascular risk, leading Merck to withdraw the product from the market in 2004.
Tragically, Merck’s manipulation of its data—and the FDA’s resulting approval of Vioxx in 1999—led to thousands of avoidable premature deaths and 100,000 heart attacks.’ https://www.ucsusa.org/resources/merck-manipulated-science-about-drug-vioxx
Yes, not exactly their finest hour. However, the point that I want to highlight from this sorry tale is that it is estimated that Vioxx caused 100,000 additional heart attacks, in the US alone, and nobody noticed. This figure was only worked out when researchers analysed the figures on increased risk, that had been seen in the clinical trials – at least the figures that were finally seen when Merck were forced to release the data.
You may think. How could one hundred thousand heart attacks simply be missed? Well, there are very nearly one million physicians in the US. If the heart attacks caused by Vioxx were evenly distributed, only one in five physicians would have seen anyone suffer because of taking Vioxx. In those physicians that did see one, or two, would they have made the connection? No, they would not. Not in a million years. There would not even be a record of any possible connection made.
Elderly person has a stroke, or heart attack. Elderly person took Vioxx. And…?
All of which means I am not gigantically concerned about CVST and SVT. Blood clots in these veins are rare, and remain rare, even after vaccination – and will never be missed, particularly when they happen in younger people. Because when younger people die, great efforts are made to establish the cause of death.
However, I can see no reason why these specific blood vessels would be targeted by blood clots. Perhaps there is some reason why clots only occur in the central venous sinus vein, or splanchnic vein following vaccination. If so, I have been unable to find out. I am more than willing to be educated on this.
Time to move on to the other worrying observation, that can be found within the report by the pharmacovigilance risk assessment committee (PRAC) – as mentioned above:
‘The PRAC noted that the blood clots occurred in veins in the brain (cerebral venous sinus thrombosis, CVST) and the abdomen (splanchnic vein thrombosis) and in arteries, together with low levels of blood platelets and sometimes bleeding.’
One blood clot, in one relatively small vein, is not going to cause a low platelet level. Nor will it cause bleeding – a sign of very low platelet levels. Which means that those unfortunate people who developed CVST and SVT almost certainly had widespread problems with other clots as well. Then, for reasons unknown, they triggered these forms of, vanishingly rare blood clot. The ones that killed them. The ones that were recognised – because they are so rare.
I shall finish here. You can join the dots yourself. Or not.
2: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4399148/
3: https://pubmed.ncbi.nlm.nih.gov/15141377/
4: https://covid.joinzoe.com/post/covid-symptoms-diarrhoea
5: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2614534/
6: https://academic.oup.com/cardiovascres/article/116/6/1097/5813131
7: https://www.karger.com/Article/FullText/512007

Back in autumn 2006, I attended a conference at the Chateau Laurier here in Ottawa at which a Canadian general waxed lyrical about the just completed Operation Medusa in the Panjwai District of Afghanistan. The Canadian soldiers in Afghanistan were the best the country had every produced; the Taliban had been utterly crushed; it was now just a matter of some final mopping up. Victory was ours!
It was a glorious display of triumphalism, echoed in just about every other talk at the conference. It was also completely unjustified. The Taliban were far from defeated, and the Canadian army had to go backwards and forwards in Panjwai for several more years (“mowing the grass” as they called it) before packing up and going home.
Now, the tables are turned, with news emerging from Afghanistan that Panjwai has fallen fully under Taliban control. It’s estimated that Canada spent $18 billion in Afghanistan. 159 Canadian soldiers lost their lives – many more were injured. After the country paid such a price, you might imagine that our press would be interested in the news that the Taleban have captured Panjwai. But not a bit of it. On the CBC website, there’s not a word. In Canada’s premier newspaper, The Globe and Mail, not a word. In my local rag, The Ottawa Citizen, not a word. It’s as if it all didn’t happen.
To my mind, this is deeply problematic. If we are to learn any lessons from the fiasco of the Afghan operation, we first have to admit that there’s a problem. Instead, we seem intent on forgetting.
The military campaign in Afghanistan was a mistake from the very start. It’s tempting to believe that we could have got a different result if we’d committed more resources or tried different tactics. But political limitations meant that more resources were not available. Afghanistan simply didn’t matter enough for the government to be able to persuade the public to commit significantly more to the conflict. As for tactics, different commanders tried a whole succession of different methods; none worked. Failure wasn’t a product of military incompetence. The war was fundamentally unwinnable.
Against this, some might argue that winning was never the point. Canada, like many other NATO members, wasn’t there to defeat the Taliban but to be good allies to the United States. But this isn’t a very effective argument. The only point of showing oneself to be a good ally is so that you get something back in return. But Canada – like, I suspect, other US allies – appears to have got diddly squat. For instance, helping the Americans in Afghanistan didn’t stop Trump from tearing up the NAFTA treaty or stop Biden kicking Canada in the teeth by cancelling the Keystone and Line 5 pipelines (both of great importance to the Canadian economy). Besides, if the point of fighting is to be an ally, you achieve your strategic goal just by turning up. Consequently, what you do thereafter doesn’t matter. Military operations thus get entirely detached from strategy. The result is inevitably a mess. In other words, it’s a poor strategic objective. It’s not one we should have set ourselves.
There is a simple lesson to draw from all this: we shouldn’t have sent our army to Afghanistan. It didn’t help Afghanistan, and it didn’t help us. Let’s not repeat the same mistake somewhere else in the future.
by Naresh Jotwani for the Saker Blog
Washington Post recently ran an article with headline which contained the two phrases “civilized nations” and “deter Beijing and Moscow” (see a review here). Use of the latter phrase in the headline shows clearly that the phrase “civilized nations” here has undisguised, in-your-face geopolitical motivation.
But “civilized” and “deter” is in fact a very strange combination of words, tempting and encouraging us to dig deeper into the matter.
One must assume that, in geopolitics, it is “just another day at the office” for one power to attempt to deter another. If two powers are in a state of unstable equilibrium, but not yet openly at war, attempts to deter one another would go on. Such is life. Certain lines – red or otherwise! – must not be crossed, weighty pronouncements must be made, and “swords must be banged against shields”. All this is standard stuff which foreign office trainees must learn, and upon which their “superiors” must base their upward mobility.
Clearly physical power is the one deterrent we all know about, starting from our experiences in school. But what has “being civilized” got to do with all that? Makes you wonder.
Surely I would be deterred by a big guy carrying a big stick – regardless of whether or not he seems to be “civilized”. In the same way, I am also deterred by a growling dog – regardless of whether or not it is fed and groomed by a rich owner! Chengiz Khan attacked other countries with brutal physical force, without any claims of possessing “higher civilization”. Before the sack of Rome, Alaric behaved far more sensibly than the “civilized” ruling elite of Rome.
Around the same time, another article also appeared, this one on the subject of Russian history and civilization (a review here). This article was an honest attempt to educate others, but there was no sign of any attempt to deter anyone. Indeed a resplendent, vibrant, creative civilization attracts others, does not deter them. If a “civilization” is aiming to deter others, then what happens to all the talk of “civilizational values” and “soft power”?
We know that power flows through the barrel of a gun, but today do culture and civilization also flow through the barrel of a gun? Something is surely wrong here! Historically, have the “civilized” always won wars? How do we explain the very recent history of Afghanistan? Which “civilization” has been gaining the upper hand there? What did the “civilized nations” achieve there? Whom did they manage to deter? For how long?
What follows is a brief history of how we have got to where we now find ourselves. This is not a work of “academic scholarship” – but rather it connects various “dots” discovered by scholars. The connections are based on the play of human nature we see all around us today.
The word “civilize” derives from the Latin root “civis”, meaning “citizen”, and in this way it is predicated on the idea of a “city”. Nomadic tribes of a period earlier than, say, 10,000 years BC would not have such a word in their language, even while the concept of “fellow tribesman” would be internalized very well.
The earliest cities were in fact trading centres for the surplus primary produce of nearby hamlets and villages. Trading – that is, eminently sensible economic exchanges – happened long before the invention of writing and of money. People were smart even then.
Trade generated surplus wealth. Thus people in cities – that is, traders of one sort or another – were free to explore aspects of life other than the hard work of primary production. Philosophy, religion, politics, law, “higher” arts and literature … all these flourished. Individuals in the city cultivated themselves, while their fellow human beings “out there” cultivated the land. Paeans and hymns were dutifully sung to the glory of the city and her various “gods”.
It was not long before the cultivated ones thought of themselves as “superior” to the others. In any one-on-one interaction with a simpler human being, they could easily run circles around the latter – and probably also justify charging a fee for the privilege!
Aided by writing and money, political power of cities grew rapidly, and it soon reached a point at which cities deemed themselves to be “proud city states”. Thence arose class differentiation between “civilized” city dwellers and the rustic population outside, which was by then economically and politically dependent on the cities. City states eventually grew into empires, following the all-too-familiar dynamic of unlimited human greed and brutality.
The simpler rustic folk were divided into “subjects”, “serfs”, “slaves” … and so on; but when the rustic folk got into friction or warfare with the “civilized” ones, they were dubbed “barbarians”. The preferred words nowadays are “deplorable”, “backward”, “lower caste” et cetera.
This phenomenon has played out repeatedly in recorded history. The phenomenon is grounded in economic motivations, and therefore it also has huge economic consequences.
Before “civilizations” came into being – and therefore before the invention of money and writing – the relationships between primary producers and traders were simple and direct, as depicted below.

Even huge geographical distances could not block trade, since ships and caravans could be used. Traders were brave and ingenious. For probably a couple of millennia, mankind experienced a “golden age of trading”, during which benefits of trade accrued but without onerous economic exploitation, slavery, human trafficking, and so on.
Things changed after the emergence of money, writing and “civilizations”. Multiple layers of political, social, financial, legal and other services emerged, giving opportunity to every “citizen” to climb the hierarchy of choice, depending on his or her aptitude and talent. Of course the two most useful talents would be greed and cunning – but clearly any other talent could be put to use, for example physical beauty, or the ability to declaim in public.
Ever since then, members of the “civilized elite” of most “civilizations” have wanted to get into the act and take their cut. The main goal of such “civilized elite” is to grab every opportunity for easy money, with the view: “After me, the deluge!”
The situation thus evolved to what is shown below, in what is projected as “progress” or the “unstoppable march of human advancement”. Men and women high up in the “pecking order” of a “civilization”, puffed up with their own social position and self-importance, feel free to make profound pronouncements about “the masses” or “the common people”.

[Incidentally, how “civilized” can a society be in which we use the phrase “pecking order”? The verb “peck” applies to poultry birds, and is also seen in the phrase “hen-pecked husband”.]
So much for “civilized”, the word wrongly used in the Washington Post article.
Surprisingly, this discussion brings us close to Saker’s recent decision to write and share with us short vignettes about the teachings of Jesus Christ. How so?
Jesus Christ lived through a period of great turmoil in the region, as the ruthless might of the Roman empire came into contact with independent minded Hebrews. His message was of love and charity, rather than greed. He promised deliverance to his followers, mostly poor folk.
When does a poor person cry out for deliverance? For the many poor people that I know, a bit of poverty is alright if only they are allowed to live on in peace. None of them demands perfect economic equality. Many earn their livelihood working for richer people. “I am alright, Jack. Let me be!”, they say – as they adapt, cope and share.
But turmoil most definitely does occur when even the otherwise forbearing poor are in unbearable distress; that possibility can never be ruled out.
Turmoil did occur in the period when Jesus lived and taught. Therefore, his teachings include useful, practical sayings addressing the daily economic and political reality of the poor people who were his followers. We may consider just three of his many profound sayings:
Man shall not live by bread alone …
It is easier for a camel to pass through the eye of a needle than for a rich person to enter the Kingdom of God.
Render unto Caesar the things which are Caesar’s …
By the way, these themes are not readily found in Gautam Buddha’s teachings. Why? Buddha lived in pre-Alexander India. Specific instances of suffering which moved him, when he was a young prince, were disease, old age, death … All of which is really kid stuff compared to what the Romans and other people of the time did on a regular basis.
Gautam Buddha traced the roots of suffering to desire, whereas the followers of Jesus Christ suffered from extreme deprivation and cruelty. It would be inhuman to say that desire was at the root of their suffering, when in fact they desired only deliverance from extreme deprivation and cruelty. Buddha and Jesus Christ addressed two totally different audiences, separated greatly in time, space and economic/political conditions.
It’s time to turn our attention back to some economic and political realities.
It is much easier to make money otherwise than by being a primary producer, and typically every human being seeks the easier path rather than the harder one. Primary producers are therefore left further and further behind in the headlong societal rush towards material well-being. However, no self-respecting community or country should accept such a dire economic fate for a significant fraction of its hard-working members.
Political and economic measures must therefore address this issue in a fair manner, and also provide avenues open to all members to benefit from training, education and economic mobility. Any ideology – “capitalism”, “neo-liberalism” or whatever else – which violates this fairness criterion will enrich a very few but also doom the society. Any talk of “trickle down wealth” is no more than false propaganda; “trickle down” just does not happen.
The attitude of “civilizational upper-hand” displayed in the Washington Post headline leads to a bargaining tactic which goes something like this:
Hey, you! Every time we engage in any transaction, negotiation, discussion or collaboration, do keep in mind that – since I am more “civilized” – I am by definition superior to you. Is it not enough for you that I even deign to sit and talk with you?
As against this, realistic bargaining between parties must proceed only on the basis of specific strong and weak points of each party. Any presumed and self-proclaimed – but meaningless! – “civilizational superiority” has nothing to do with any real-life negotiation. Why introduce such a red herring of into “real-politik”? In today’s intellectually multi-polar, competitive world, the adversary easily sees through all such false pretences anyway.
The reality of being “civilized” – if indeed there is such reality! – must not depend on haughty self-proclamation. The word “civilized” must be defined in terms which are universal.
Our only “city” now is the entire Planet Earth. There are no outsiders, and therefore the word “civilized” has to have meaning not limited by this or that so-called great city of the past or present – whether that be Rome, Athens, Washington, Beijing, Jerusalem or Varanasi.
In that spirit, a simple test is proposed here for the reader’s consideration:
Regardless of how highly accomplished an individual may be – in music, literature, politics, law, science, wealth, beauty or any combination thereof – does the person “get it” and accept that the most deprived individual is also a human being deserving of dignity and respect?
Note that the word “charity” does not even occur here. Acknowledgement of the other person’s humanity is far more fundamental that any outward act of “charity”. It follows that laughing at deprived individuals or pouring scorn over them is not civilized behaviour.
Only if the above test is satisfied should a person today be considered “civilized”. Loud, self-serving proclamations do not count. This is a matter not of “politics” or “ideology”, but of humanity. Nobody need fly off at the handle shrieking “Buddha”, “Jesus Christ”, “capitalism”, “communism” or “socialism”! Humanity does not dwell in a person’s brain, wealth or loquacity, but deep inside the heart – or perhaps not even there.
Lest anybody misunderstand, none of the above is a justification for what does or does not happen in my own country. Wherever there are human beings, certain behaviour patterns are bound to be seen. Most of what is described here has gone on blatantly in India for many centuries, and at present there is an intense internal struggle in progress.
The point here is that any “civilization” worth its name should help temper economic injustice rather than exacerbate it. In times of huge diversity and change, an attitude amongst people of “us” versus “them” is inevitable. The key questions ask must be such as these:
What are the terms under which societal injustices and resentments are resolved? How exploitative are these terms? How is extreme deprivation avoided?
No society can be strong if brutal economic exploitation runs rampant amongst its people. The following paradox is too glaring to be missed:
“Leaders” who declaim the loudest about being “civilized”, and try to impose their “civilizational values” on others, represent the very same societies which are going through relatively rapid exacerbation of internal fissures. A recent extensive survey carried out in the UK reported that, according to most younger respondents, the number one priority of the government should be to protect the poorest, weakest and the most vulnerable. An overwhelming majority said “F**k them all” about their own political leaders. (A summary of the survey can be found here.)
Much should be expected from anyone claiming to be “civilized” today.


Dr. Stephen Malthouse appeared at a rally against COVID-19 restrictions in Duncan, B.C., in November, referring to the disease as a 'so-called pandemic.' (YouTube)
Doctors in B.C. have been warned that spreading misinformation about COVID-19 and vaccines could harm patients and result in professional discipline.
In a joint statement issued on Thursday, the College of Physicians and Surgeons of British Columbia and the First Nations Health Authority (FNHA) say they've become aware some doctors are sharing false anti-vaccine and anti-mask ideas, as well as promoting treatments for COVID-19 that are not supported by scientific research.
This kind of misinformation is a violation of public trust as well as the ethical obligations of doctors, whom members of the public tend to trust implicitly when it comes to matters of health, the statement says.
"Public statements from physicians that contradict public health orders and guidance are confusing and potentially harmful to patients," college registrar Dr. Heidi Oetter said in the release.
"Those who put the public at risk with misinformation may face an investigation by the college and, if warranted, regulatory action."
The FNHA says misinformation from doctors is particularly damaging in Indigenous communities, which have been disproportionately affected by the pandemic.
"Indigenous people already face barriers to accessing health care due to systemic racism," Dr. Nel Wieman, the FNHA's acting deputy chief medical officer said.
"Misleading information adds another barrier at a time when the COVID-19 vaccine needs to be delivered to Indigenous people as quickly as possible."
B.C. doctors gain prominence for questionable claims
Though the notice does not single out any individual physicians by name, a small number of doctors in B.C. have become popular among groups that oppose vaccines, masks and other measures meant to reduce COVID-19 transmission.
That includes Dr. Stephen Malthouse of Denman Island, who has appeared at numerous rallies against mask mandates and other public health measures and in October 2020 wrote a widely circulated open letter to Provincial Health Officer Dr. Bonnie Henry that falsely suggested the coronavirus is no more deadly than the flu.
Malthouse told The Canadian Press he had not seen the college's statement but encouraged the regulator to reach out to doctors who have differing views.
"We really need to have scientific debate about these topics rather than just having rules and regulations and attempts just to make doctors follow the policy alone," he said. "If doctors have questions about it, I think that the college should really be in a position to discuss it with them."

As of May 1, B.C. recorded 54 serious adverse events connected to COVID-19 vaccines out of 1.85 million doses administered. (Ryan Remiorz/The Canadian Press)
Another B.C. doctor, anesthesiologist Dr. Bill Code of Duncan, appeared in a video alongside Malthouse in March this year claiming that he was successfully treated for COVID-19 with vitamins and hydroxychloroquine. Hydroxychloroquine was once promoted by Donald Trump as a "game changer" but has since proven to be ineffective against the virus and potentially risky.
Code told The Canadian Press he believes his claims are based on scientific research and that health officials and politicians are just telling one side of the story.
54 adverse events out of 1.85M doses in B.C. so far
More recently, Lytton, B.C., family physician Dr. Charles Hoffe published another letter to Henry on the website of the anti-vaccine group Vaccine Choice Canada, making numerous unproven and false claims about COVID-19 vaccines.
Hoffe claimed in his letter, dated April 5, that after administering the Moderna shot to community members, he believes "this vaccine is quite clearly more dangerous than COVID-19."
- Colleges stress public responsibilities as MD, nurse set to speak at rally against COVID-19 measures
The B.C. Centre for Disease Control publishes weekly updates on adverse events following COVID-19 vaccination, and as of May 1, a total of 54 serious health events, including anaphylaxis, seizure and possible neurological effects, were reported out of 1.85 million doses administered. That's a rate of about 0.002 per cent.
While four people have died within 30 days of receiving one of those 1.85 million shots, none of those deaths are believed to be the result of the vaccine. In comparison, 1,622 people have died of COVID-19 in B.C. out of 136,100 confirmed cases.
Hoffe's letter also echoes a common but thoroughly debunked talking point used in conspiracy theorist circles that suggests mRNA vaccines are actually a form of "experimental gene modification therapy."
These vaccines, which include the COVID-19 shots from Pfizer and Moderna, absolutely cannot alter someone's genes.
The only thing mRNA does inside the human body is carry the instructions for building proteins — in the case of vaccines, those proteins trigger an immune response. Once those proteins have been built, the mRNA degrades, and it's physically impossible for it to be incorporated into a person's DNA.
"You can't go from RNA back to DNA in human cells. It's not possible because we just don't have the machinery to deal with it," Dr. Zain Chagla of McMaster University in Hamilton told CBC News in December.
Hoffe has yet to respond to requests for comment from CBC News or The Canadian Press.
It's not known if Malthouse, Code or Hoffe face any regulatory action from their professional college, and all three are currently licensed to practise without any conditions. The college doesn't release any public information about its investigations unless a matter is deemed to be serious.
In this recently published document:

...Public Health England provides us with some interesting information on COVID-19 vaccine effectiveness. Let's take a close look at the findings of the authors.
The report looks at 60,624 Delta variant infections between February 1, and June 14, 2021. Here is a table showing vaccine effectiveness against symptomatic disease for the Alpha and Delta variants combined for doses 1 and 2:

Here is a table showing vaccine effectiveness against hospitalization for the Alpha and Delta variants for doses 1 and 2:

The data would certainly appear to suggest that the COVID-19 vaccines have been quite effective (particularly after the second dose) at reducing symptoms and hospitalizations although the effectiveness of the current COVID-19 vaccines are less effective at preventing symptomatic disease related to the Delta variant than they are for the Alpha variant.
Here is the most interesting table which shows the number of delta cases which either died or required emergency care between February 1, 2021 and June 14, 2021 among unvaccinated, people who were vaccinated with one dose 21 or less days previously, one dose 21 or more days previously and those who were fully vaccinated 14 days or more previously:

A total of 35,521 Delta variant cases were among the unvaccinated compared to 4,087 cases which were fully vaccinated. That said, it is somewhat concerning that there were thousands of cases of the Delta variant despite the fact that the individuals were fully vaccinated at least two weeks prior to the test.
Let's compare the hospitalization rates for the unvaccinated versus the fully vaccinated:
Unvaccinated - 35,521 people with 527 or 1.48 percent required hospitalization
Fully Vaccinated - 4,087 people with 84 or 2.05 percent required hospitalization
Now, let's compare the death rates for the unvaccinated versus the fully vaccinated:
Unvaccinated - 35,521 people with 34 or 0.133 percent dying
Fully Vaccinated - 4,087 people with 26 or 0.636 percent dying
As you can see, when it comes to the Delta variant, while there are far more infections among the unvaccinated, those who are infected and unvaccinated are less likely to require hospitalization and nearly 5 times less likely to die than their vaccinated peers.
Now, let's look at a study from 2012 where laboratory animals were injected with experimental coronavirus vaccines after SARS emerged in China in 2002:

In this study, a variety of potential candidate coronavirus vaccines for humans with or without alum adjuvant were tested; a VLP (virus-like particle) vaccine, an NHP whole virus vaccine and an rDNA-produced S protein vaccines. The vaccines were injected into both ferrets and mice. All of the vaccines induced serum neutralizing antibodies with increasing dosages and the presence of alum, resulting in significantly increased responses.
Here are the results as quoted from the study with challenge meaning that the mice were exposed to the live SARS-CoV virus:
"Significant reductions of SARS-CoV two days after challenge was seen for all vaccines and prior live SARS-CoV. All mice exhibited histopathologic changes in lungs two days after challenge including all animals vaccinated (Balb/C and C57BL/6) or given live virus, influenza vaccine, or PBS suggesting infection occurred in all."
Here are the conclusions of the study:
"These SARS-CoV vaccines all induced antibody and protection against infection with SARS-CoV. However, challenge of mice given any of the vaccines led to occurrence of Th2-type immunopathology suggesting hypersensitivity to SARS-CoV components was induced. Caution in proceeding to application of a SARS-CoV vaccine in humans is indicated.
In other words, the animals that were injected with these experimental coronavirus vaccines developed enhanced lung disease because the vaccines induced hypersensitivity to the components of SARS-Co-V.
Since the current crop of COVID-19 vaccines is still in Phase 3 trials no matter what we are being led to believe, governments, the media and Big Pharma have no idea whether the same enhancement will occur in humans. If so, this may be at least a partial explanation for the findings in England where fully vaccinated individuals who contract the Delta variant of the COVID-19 virus have a higher hospitalization and death rate than those who are not vaccinated. If so, this is a very concerning issue, particularly given that billions of doses are now "resident" in human beings around the world.

Adolescence is the phase of conflict par excellence with parents. Many blahblahgists attribute this critical phase to youth hardships, to media education, and instead the reason is much more prosaic. The adolescent, actually a man (or woman) in all respects, enters into competition with the parents who at that moment become rivals. This settles down as parents age, drop hormonally and become, as it were, children of their children.
The son is not spoilt or something else. Adolescence is a product of civilization which, as such, projects forward a life path that, conversely, would see man become a father at fourteen and die at thirty-five-forty. To push the so-called problematic teenager is his testosterone which places him in conflict with his parents. Who, on the other hand, have total responsibility for his person and are obliged to put a stop to him.
The young man would already like to copulate with the nymphet he met on the street, the young woman would already like to be penetrated by the hypertrophic bull she met in the discos, both would like money, motorcycles, travel, benefits but father and mother institutionally represent the brake that prevents them from living fully their own sexuality, their own well-being. Things that in a jungle they would be gained through conflict with other congeners but that in civilization they are limited by the laws.
If the adolescent is in a position to take care of himself, he can safely leave his father's home. But since this is never the case, the abandonment of father and mother is a whim that, especially if taken to the extreme (as unfortunately in the sad cases of patricide that the news shows us) is paid dearly. The other side of freedom is responsibility. When you no longer have a father and a mother, you are not only free to do what you want, you are also at the mercy of any storm that life throws in front of us.
The relationship between man and God is something similar. The “core business” of every religion is to provide the human being with an illusion that makes more bearable the sad fate that awaits him. A guide. Support. A father, a mother. It is not by chance that God is called as Father. And Our Lady, it goes without saying, mother. As our fathers and mothers age and die and are human, therefore fallible, we realize that, not for this reason, we stop being children. Those who have the misfortune of being an orphan and of not being a believer thus find themselves in a situation of very serious inner crisis, dictated by the awareness of their own fragility. If he/she goes through a moment of economic difficulty or, worse still, is unable to support himself or herself because he/she is too young or because of a job crisis, he/she gets a terrible blow from the loss of parents, realizing at that moment how stupid teenage riots were.
Similarly, those who are unable to keep their soul upright realize that God's death is not the so-hoped-for “free lair”. For centuries, Man has tried to kill God, to free himself from that inner restraint constituted by the presence of robust and pervasive rules which, even if they were to be based on a fantasy, still constituted a foundation, a guide. Man in adolescent crisis, with blows of progress, democracy, egalitarianism, has killed God. But he did this deicide before being able to find his own spiritual independence, his ability to know how to accept his own destiny, characteristic of every true layman, just like the reckless one of Pietro Maso [1], killed his parents to pocket the family inheritance and delude himself to lead a life based solely on the narcissistic cult of his own person.
Above all, one thing happens to every orphan and every atheist. Often it is crossed by many profiteers, ready to illegally occupy that role. The orphan is forced to identify in each future partner a father or a surrogate mother, not realizing that, however much he/she may take on appearance, he/she is not and will never be a father or a mother.
The atheist believes in magicians, witches, ideologies, including that of a paternal State, which takes care of all.
Behind many wrong marriages there is just this, behind the belief that a magician can succeed where a good doctor has failed, behind political tyrannies: despair, fear of physical and spiritual loneliness, the inability to know how to take care not only of our body but also of our spirit. Thus, what Chesterton said is fulfilled:
“Whoever does not believe in God is not that he or she no longer believes in anything, from that moment on he or she believes in everything.
By killing God without really becoming adults, with all the burden of suffering that this entails, we realized that we are not free, we are simply poor. We are rafts wandering aimlessly in the ocean, with forces that are about to run out and that will soon be swept away by the waves. And all this I say as a non-believer. As an orphan, in every sense.
In short, with respect speaking, I am, we're, in a bad patch.
Those who feel excluded from this speech and are tempted to insult me, know that instead they have my most sincere congratulations: I would like to be filled with insults if this meant a happier mankind.
[1] Italian patricide. With the help of three friends of him, In 1991 he killed both his parents.
Original column by Franco Marino:
Translation by Costantino Ceoldo
During the recent Direct Line, when I was asked about Russian-Ukrainian relations, I said that Russians and Ukrainians were one people – a single whole. These words were not driven by some short-term considerations or prompted by the current political context. It is what I have said on numerous occasions and what I firmly believe. I therefore feel it necessary to explain my position in detail and share my assessments of today's situation.
First of all, I would like to emphasize that the wall that has emerged in recent years between Russia and Ukraine, between the parts of what is essentially the same historical and spiritual space, to my mind is our great common misfortune and tragedy. These are, first and foremost, the consequences of our own mistakes made at different periods of time. But these are also the result of deliberate efforts by those forces that have always sought to undermine our unity. The formula they apply has been known from time immemorial – divide and rule. There is nothing new here. Hence the attempts to play on the ”national question“ and sow discord among people, the overarching goal being to divide and then to pit the parts of a single people against one another.
To have a better understanding of the present and look into the future, we need to turn to history. Certainly, it is impossible to cover in this article all the developments that have taken place over more than a thousand years. But I will focus on the key, pivotal moments that are important for us to remember, both in Russia and Ukraine.
Russians, Ukrainians, and Belarusians are all descendants of Ancient Rus, which was the largest state in Europe. Slavic and other tribes across the vast territory – from Ladoga, Novgorod, and Pskov to Kiev and Chernigov – were bound together by one language (which we now refer to as Old Russian), economic ties, the rule of the princes of the Rurik dynasty, and – after the baptism of Rus – the Orthodox faith. The spiritual choice made by St. Vladimir, who was both Prince of Novgorod and Grand Prince of Kiev, still largely determines our affinity today.
The throne of Kiev held a dominant position in Ancient Rus. This had been the custom since the late 9th century. The Tale of Bygone Years captured for posterity the words of Oleg the Prophet about Kiev, ”Let it be the mother of all Russian cities.“
Later, like other European states of that time, Ancient Rus faced a decline of central rule and fragmentation. At the same time, both the nobility and the common people perceived Rus as a common territory, as their homeland.
The fragmentation intensified after Batu Khan's devastating invasion, which ravaged many cities, including Kiev. The northeastern part of Rus fell under the control of the Golden Horde but retained limited sovereignty. The southern and western Russian lands largely became part of the Grand Duchy of Lithuania, which – most significantly – was referred to in historical records as the Grand Duchy of Lithuania and Russia.
Members of the princely and ”boyar“ clans would change service from one prince to another, feuding with each other but also making friendships and alliances. Voivode Bobrok of Volyn and the sons of Grand Duke of Lithuania Algirdas – Andrey of Polotsk and Dmitry of Bryansk – fought next to Grand Duke Dmitry Ivanovich of Moscow on the Kulikovo field. At the same time, Grand Duke of Lithuania Jogaila – son of the Princess of Tver – led his troops to join with Mamai. These are all pages of our shared history, reflecting its complex and multi-dimensional nature.
Most importantly, people both in the western and eastern Russian lands spoke the same language. Their faith was Orthodox. Up to the middle of the 15th century, the unified church government remained in place.
At a new stage of historical development, both Lithuanian Rus and Moscow Rus could have become the points of attraction and consolidation of the territories of Ancient Rus. It so happened that Moscow became the center of reunification, continuing the tradition of ancient Russian statehood. Moscow princes – the descendants of Prince Alexander Nevsky – cast off the foreign yoke and began gathering the Russian lands.
In the Grand Duchy of Lithuania, other processes were unfolding. In the 14th century, Lithuania's ruling elite converted to Catholicism. In the 16th century, it signed the Union of Lublin with the Kingdom of Poland to form the Polish–Lithuanian Commonwealth. The Polish Catholic nobility received considerable land holdings and privileges in the territory of Rus. In accordance with the 1596 Union of Brest, part of the western Russian Orthodox clergy submitted to the authority of the Pope. The process of Polonization and Latinization began, ousting Orthodoxy.
As a consequence, in the 16–17th centuries, the liberation movement of the Orthodox population was gaining strength in the Dnieper region. The events during the times of Hetman Bohdan Khmelnytsky became a turning point. His supporters struggled for autonomy from the Polish–Lithuanian Commonwealth.
In its 1649 appeal to the king of the Polish–Lithuanian Commonwealth, the Zaporizhian Host demanded that the rights of the Russian Orthodox population be respected, that the voivode of Kiev be Russian and of Greek faith, and that the persecution of the churches of God be stopped. But the Cossacks were not heard.
Bohdan Khmelnytsky then made appeals to Moscow, which were considered by the Zemsky Sobor. On 1 October 1653, members of the supreme representative body of the Russian state decided to support their brothers in faith and take them under patronage. In January 1654, the Pereyaslav Council confirmed that decision. Subsequently, the ambassadors of Bohdan Khmelnytsky and Moscow visited dozens of cities, including Kiev, whose populations swore allegiance to the Russian tsar. Incidentally, nothing of the kind happened at the conclusion of the Union of Lublin.
In a letter to Moscow in 1654, Bohdan Khmelnytsky thanked Tsar Aleksey Mikhaylovich for taking ”the whole Zaporizhian Host and the whole Russian Orthodox world under the strong and high hand of the Tsar“. It means that, in their appeals to both the Polish king and the Russian tsar, the Cossacks referred to and defined themselves as Russian Orthodox people.
Over the course of the protracted war between the Russian state and the Polish–Lithuanian Commonwealth, some of the hetmans, successors of Bohdan Khmelnytsky, would ”detach themselves“ from Moscow or seek support from Sweden, Poland, or Turkey. But, again, for the people, that was a war of liberation. It ended with the Truce of Andrusovo in 1667. The final outcome was sealed by the Treaty of Perpetual Peace in 1686. The Russian state incorporated the city of Kiev and the lands on the left bank of the Dnieper River, including Poltava region, Chernigov region, and Zaporozhye. Their inhabitants were reunited with the main part of the Russian Orthodox people. These territories were referred to as ”Malorossia“ (Little Russia).
The name ”Ukraine“ was used more often in the meaning of the Old Russian word ”okraina“ (periphery), which is found in written sources from the 12th century, referring to various border territories. And the word ”Ukrainian“, judging by archival documents, originally referred to frontier guards who protected the external borders.
On the right bank, which remained under the Polish–Lithuanian Commonwealth, the old orders were restored, and social and religious oppression intensified. On the contrary, the lands on the left bank, taken under the protection of the unified state, saw rapid development. People from the other bank of the Dnieper moved here en masse. They sought support from people who spoke the same language and had the same faith.
During the Great Northern War with Sweden, the people in Malorossia were not faced with a choice of whom to side with. Only a small portion of the Cossacks supported Mazepa's rebellion. People of all orders and degrees considered themselves Russian and Orthodox.
Cossack senior officers belonging to the nobility would reach the heights of political, diplomatic, and military careers in Russia. Graduates of Kiev-Mohyla Academy played a leading role in church life. This was also the case during the Hetmanate – an essentially autonomous state formation with a special internal structure – and later in the Russian Empire. Malorussians in many ways helped build a big common country – its statehood, culture, and science. They participated in the exploration and development of the Urals, Siberia, the Caucasus, and the Far East. Incidentally, during the Soviet period, natives of Ukraine held major, including the highest, posts in the leadership of the unified state. Suffice it to say that Nikita Khrushchev and Leonid Brezhnev, whose party biography was most closely associated with Ukraine, led the Communist Party of the Soviet Union (CPSU) for almost 30 years.
In the second half of the 18th century, following the wars with the Ottoman Empire, Russia incorporated Crimea and the lands of the Black Sea region, which became known as Novorossiya. They were populated by people from all of the Russian provinces. After the partitions of the Polish-Lithuanian Commonwealth, the Russian Empire regained the western Old Russian lands, with the exception of Galicia and Transcarpathia, which became part of the Austrian – and later Austro-Hungarian – Empire.
The incorporation of the western Russian lands into the single state was not merely the result of political and diplomatic decisions. It was underlain by the common faith, shared cultural traditions, and – I would like to emphasize it once again – language similarity. Thus, as early as the beginning of the 17th century, one of the hierarchs of the Uniate Church, Joseph Rutsky, communicated to Rome that people in Moscovia called Russians from the Polish-Lithuanian Commonwealth their brothers, that their written language was absolutely identical, and differences in the vernacular were insignificant. He drew an analogy with the residents of Rome and Bergamo. These are, as we know, the center and the north of modern Italy.
Many centuries of fragmentation and living within different states naturally brought about regional language peculiarities, resulting in the emergence of dialects. The vernacular enriched the literary language. Ivan Kotlyarevsky, Grigory Skovoroda, and Taras Shevchenko played a huge role here. Their works are our common literary and cultural heritage. Taras Shevchenko wrote poetry in the Ukrainian language, and prose mainly in Russian. The books of Nikolay Gogol, a Russian patriot and native of Poltavshchyna, are written in Russian, bristling with Malorussian folk sayings and motifs. How can this heritage be divided between Russia and Ukraine? And why do it?
The south-western lands of the Russian Empire, Malorussia and Novorossiya, and the Crimea developed as ethnically and religiously diverse entities. Crimean Tatars, Armenians, Greeks, Jews, Karaites, Krymchaks, Bulgarians, Poles, Serbs, Germans, and other peoples lived here. They all preserved their faith, traditions, and customs.
I am not going to idealise anything. We do know there were the Valuev Circular of 1863 an then the Ems Ukaz of 1876, which restricted the publication and importation of religious and socio-political literature in the Ukrainian language. But it is important to be mindful of the historical context. These decisions were taken against the backdrop of dramatic events in Poland and the desire of the leaders of the Polish national movement to exploit the ”Ukrainian issue“ to their own advantage. I should add that works of fiction, books of Ukrainian poetry and folk songs continued to be published. There is objective evidence that the Russian Empire was witnessing an active process of development of the Malorussian cultural identity within the greater Russian nation, which united the Velikorussians, the Malorussians and the Belorussians.
At the same time, the idea of Ukrainian people as a nation separate from the Russians started to form and gain ground among the Polish elite and a part of the Malorussian intelligentsia. Since there was no historical basis – and could not have been any, conclusions were substantiated by all sorts of concoctions, which went as far as to claim that the Ukrainians are the true Slavs and the Russians, the Muscovites, are not. Such ”hypotheses“ became increasingly used for political purposes as a tool of rivalry between European states.
Since the late 19th century, the Austro-Hungarian authorities had latched onto this narrative, using it as a counterbalance to the Polish national movement and pro-Muscovite sentiments in Galicia. During World War I, Vienna played a role in the formation of the so-called Legion of Ukrainian Sich Riflemen. Galicians suspected of sympathies with Orthodox Christianity and Russia were subjected to brutal repression and thrown into the concentration camps of Thalerhof and Terezin.
Further developments had to do with the collapse of European empires, the fierce civil war that broke out across the vast territory of the former Russian Empire, and foreign intervention.
After the February Revolution, in March 1917, the Central Rada was established in Kiev, intended to become the organ of supreme power. In November 1917, in its Third Universal, it declared the creation of the Ukrainian People's Republic (UPR) as part of Russia.
In December 1917, UPR representatives arrived in Brest-Litovsk, where Soviet Russia was negotiating with Germany and its allies. At a meeting on 10 January 1918, the head of the Ukrainian delegation read out a note proclaiming the independence of Ukraine. Subsequently, the Central Rada proclaimed Ukraine independent in its Fourth Universal.
The declared sovereignty did not last long. Just a few weeks later, Rada delegates signed a separate treaty with the German bloc countries. Germany and Austria-Hungary were at the time in a dire situation and needed Ukrainian bread and raw materials. In order to secure large-scale supplies, they obtained consent for sending their troops and technical staff to the UPR. In fact, this was used as a pretext for occupation.
For those who have today given up the full control of Ukraine to external forces, it would be instructive to remember that, back in 1918, such a decision proved fatal for the ruling regime in Kiev. With the direct involvement of the occupying forces, the Central Rada was overthrown and Hetman Pavlo Skoropadskyi was brought to power, proclaiming instead of the UPR the Ukrainian State, which was essentially under German protectorate.
In November 1918 – following the revolutionary events in Germany and Austria-Hungary – Pavlo Skoropadskyi, who had lost the support of German bayonets, took a different course, declaring that ”Ukraine is to take the lead in the formation of an All-Russian Federation“. However, the regime was soon changed again. It was now the time of the so-called Directorate.
In autumn 1918, Ukrainian nationalists proclaimed the West Ukrainian People's Republic (WUPR) and, in January 1919, announced its unification with the Ukrainian People's Republic. In July 1919, Ukrainian forces were crushed by Polish troops, and the territory of the former WUPR came under the Polish rule.
In April 1920, Symon Petliura (portrayed as one of the ”heroes“ in today's Ukraine) concluded secret conventions on behalf of the UPR Directorate, giving up – in exchange for military support – Galicia and Western Volhynia lands to Poland. In May 1920, Petliurites entered Kiev in a convoy of Polish military units. But not for long. As early as November 1920, following a truce between Poland and Soviet Russia, the remnants of Petliura's forces surrendered to those same Poles.
The example of the UPR shows that different kinds of quasi-state formations that emerged across the former Russian Empire at the time of the Civil War and turbulence were inherently unstable. Nationalists sought to create their own independent states, while leaders of the White movement advocated indivisible Russia. Many of the republics established by the Bolsheviks' supporters did not see themselves outside Russia either. Nevertheless, Bolshevik Party leaders sometimes basically drove them out of Soviet Russia for various reasons.
Thus, in early 1918, the Donetsk-Krivoy Rog Soviet Republic was proclaimed and asked Moscow to incorporate it into Soviet Russia. This was met with a refusal. During a meeting with the republic's leaders, Vladimir Lenin insisted that they act as part of Soviet Ukraine. On 15 March 1918, the Central Committee of the Russian Communist Party (Bolsheviks) directly ordered that delegates be sent to the Ukrainian Congress of Soviets, including from the Donetsk Basin, and that ”one government for all of Ukraine“ be created at the congress. The territories of the Donetsk-Krivoy Rog Soviet Republic later formed most of the regions of south-eastern Ukraine.
Under the 1921 Treaty of Riga, concluded between the Russian SFSR, the Ukrainian SSR and Poland, the western lands of the former Russian Empire were ceded to Poland. In the interwar period, the Polish government pursued an active resettlement policy, seeking to change the ethnic composition of the Eastern Borderlands – the Polish name for what is now Western Ukraine, Western Belarus and parts of Lithuania. The areas were subjected to harsh Polonisation, local culture and traditions suppressed. Later, during World War II, radical groups of Ukrainian nationalists used this as a pretext for terror not only against Polish, but also against Jewish and Russian populations.
In 1922, when the USSR was created, with the Ukrainian Soviet Socialist Republic becoming one of its founders, a rather fierce debate among the Bolshevik leaders resulted in the implementation of Lenin's plan to form a union state as a federation of equal republics. The right for the republics to freely secede from the Union was included in the text of the Declaration on the Creation of the Union of Soviet Socialist Republics and, subsequently, in the 1924 USSR Constitution. By doing so, the authors planted in the foundation of our statehood the most dangerous time bomb, which exploded the moment the safety mechanism provided by the leading role of the CPSU was gone, the party itself collapsing from within. A ”parade of sovereignties“ followed. On 8 December 1991, the so-called Belovezh Agreement on the Creation of the Commonwealth of Independent States was signed, stating that ”the USSR as a subject of international law and a geopolitical reality no longer existed.“ By the way, Ukraine never signed or ratified the CIS Charter adopted back in 1993.
In the 1920's-1930's, the Bolsheviks actively promoted the ”localization policy“, which took the form of Ukrainization in the Ukrainian SSR. Symbolically, as part of this policy and with consent of the Soviet authorities, Mikhail Grushevskiy, former chairman of Central Rada, one of the ideologists of Ukrainian nationalism, who at a certain period of time had been supported by Austria-Hungary, was returned to the USSR and was elected member of the Academy of Sciences.
The localization policy undoubtedly played a major role in the development and consolidation of the Ukrainian culture, language and identity. At the same time, under the guise of combating the so-called Russian great-power chauvinism, Ukrainization was often imposed on those who did not see themselves as Ukrainians. This Soviet national policy secured at the state level the provision on three separate Slavic peoples: Russian, Ukrainian and Belorussian, instead of the large Russian nation, a triune people comprising Velikorussians, Malorussians and Belorussians.
In 1939, the USSR regained the lands earlier seized by Poland. A major portion of these became part of the Soviet Ukraine. In 1940, the Ukrainian SSR incorporated part of Bessarabia, which had been occupied by Romania since 1918, as well as Northern Bukovina. In 1948, Zmeyiniy Island (Snake Island) in the Black Sea became part of Ukraine. In 1954, the Crimean Region of the RSFSR was given to the Ukrainian SSR, in gross violation of legal norms that were in force at the time.
I would like to dwell on the destiny of Carpathian Ruthenia, which became part of Czechoslovakia following the breakup of Austria-Hungary. Rusins made up a considerable share of local population. While this is hardly mentioned any longer, after the liberation of Transcarpathia by Soviet troops the congress of the Orthodox population of the region voted for the inclusion of Carpathian Ruthenia in the RSFSR or, as a separate Carpathian republic, in the USSR proper. Yet the choice of people was ignored. In summer 1945, the historical act of the reunification of Carpathian Ukraine ”with its ancient motherland, Ukraine“ – as The Pravda newspaper put it – was announced.
Therefore, modern Ukraine is entirely the product of the Soviet era. We know and remember well that it was shaped – for a significant part – on the lands of historical Russia. To make sure of that, it is enough to look at the boundaries of the lands reunited with the Russian state in the 17th century and the territory of the Ukrainian SSR when it left the Soviet Union.
The Bolsheviks treated the Russian people as inexhaustible material for their social experiments. They dreamt of a world revolution that would wipe out national states. That is why they were so generous in drawing borders and bestowing territorial gifts. It is no longer important what exactly the idea of the Bolshevik leaders who were chopping the country into pieces was. We can disagree about minor details, background and logics behind certain decisions. One fact is crystal clear: Russia was robbed, indeed.
When working on this article, I relied on open-source documents that contain well-known facts rather than on some secret records. The leaders of modern Ukraine and their external ”patrons“ prefer to overlook these facts. They do not miss a chance, however, both inside the country and abroad, to condemn ”the crimes of the Soviet regime,“ listing among them events with which neither the CPSU, nor the USSR, let alone modern Russia, have anything to do. At the same time, the Bolsheviks' efforts to detach from Russia its historical territories are not considered a crime. And we know why: if they brought about the weakening of Russia, our ill-wishes are happy with that.
Of course, inside the USSR, borders between republics were never seen as state borders; they were nominal within a single country, which, while featuring all the attributes of a federation, was highly centralized – this, again, was secured by the CPSU's leading role. But in 1991, all those territories, and, which is more important, people, found themselves abroad overnight, taken away, this time indeed, from their historical motherland.
What can be said to this? Things change: countries and communities are no exception. Of course, some part of a people in the process of its development, influenced by a number of reasons and historical circumstances, can become aware of itself as a separate nation at a certain moment. How should we treat that? There is only one answer: with respect!
You want to establish a state of your own: you are welcome! But what are the terms? I will recall the assessment given by one of the most prominent political figures of new Russia, first mayor of Saint Petersburg Anatoly Sobchak. As a legal expert who believed that every decision must be legitimate, in 1992, he shared the following opinion: the republics that were founders of the Union, having denounced the 1922 Union Treaty, must return to the boundaries they had had before joining the Soviet Union. All other territorial acquisitions are subject to discussion, negotiations, given that the ground has been revoked.
In other words, when you leave, take what you brought with you. This logic is hard to refute. I will just say that the Bolsheviks had embarked on reshaping boundaries even before the Soviet Union, manipulating with territories to their liking, in disregard of people's views.
The Russian Federation recognized the new geopolitical realities: and not only recognized, but, indeed, did a lot for Ukraine to establish itself as an independent country. Throughout the difficult 1990's and in the new millennium, we have provided considerable support to Ukraine. Whatever ”political arithmetic“ of its own Kiev may wish to apply, in 1991–2013, Ukraine's budget savings amounted to more than USD 82 billion, while today, it holds on to the mere USD 1.5 billion of Russian payments for gas transit to Europe. If economic ties between our countries had been retained, Ukraine would enjoy the benefit of tens of billions of dollars.
Ukraine and Russia have developed as a single economic system over decades and centuries. The profound cooperation we had 30 years ago is an example for the European Union to look up to. We are natural complementary economic partners. Such a close relationship can strengthen competitive advantages, increasing the potential of both countries.
Ukraine used to possess great potential, which included powerful infrastructure, gas transportation system, advanced shipbuilding, aviation, rocket and instrument engineering industries, as well as world-class scientific, design and engineering schools. Taking over this legacy and declaring independence, Ukrainian leaders promised that the Ukrainian economy would be one of the leading ones and the standard of living would be among the best in Europe.
Today, high-tech industrial giants that were once the pride of Ukraine and the entire Union, are sinking. Engineering output has dropped by 42 per cent over ten years. The scale of deindustrialization and overall economic degradation is visible in Ukraine's electricity production, which has seen a nearly two-time decrease in 30 years. Finally, according to IMF reports, in 2019, before the coronavirus pandemic broke out, Ukraine's GDP per capita had been below USD 4 thousand. This is less than in the Republic of Albania, the Republic of Moldova, or unrecognized Kosovo. Nowadays, Ukraine is Europe's poorest country.
Who is to blame for this? Is it the people of Ukraine's fault? Certainly not. It was the Ukrainian authorities who waisted and frittered away the achievements of many generations. We know how hardworking and talented the people of Ukraine are. They can achieve success and outstanding results with perseverance and determination. And these qualities, as well as their openness, innate optimism and hospitality have not gone. The feelings of millions of people who treat Russia not just well but with great affection, just as we feel about Ukraine, remain the same.
Until 2014, hundreds of agreements and joint projects were aimed at developing our economies, business and cultural ties, strengthening security, and solving common social and environmental problems. They brought tangible benefits to people – both in Russia and Ukraine. This is what we believed to be most important. And that is why we had a fruitful interaction with all, I emphasize, with all the leaders of Ukraine.
Even after the events in Kiev of 2014, I charged the Russian government to elaborate options for preserving and maintaining our economic ties within relevant ministries and agencies. However, there was and is still no mutual will to do the same. Nevertheless, Russia is still one of Ukraine's top three trading partners, and hundreds of thousands of Ukrainians are coming to us to work, and they find a welcome reception and support. So that what the ”aggressor state“ is.
When the USSR collapsed, many people in Russia and Ukraine sincerely believed and assumed that our close cultural, spiritual and economic ties would certainly last, as would the commonality of our people, who had always had a sense of unity at their core. However, events – at first gradually, and then more rapidly – started to move in a different direction.
In essence, Ukraine's ruling circles decided to justify their country's independence through the denial of its past, however, except for border issues. They began to mythologize and rewrite history, edit out everything that united us, and refer to the period when Ukraine was part of the Russian Empire and the Soviet Union as an occupation. The common tragedy of collectivization and famine of the early 1930s was portrayed as the genocide of the Ukrainian people.
Radicals and neo-Nazis were open and more and more insolent about their ambitions. They were indulged by both the official authorities and local oligarchs, who robbed the people of Ukraine and kept their stolen money in Western banks, ready to sell their motherland for the sake of preserving their capital. To this should be added the persistent weakness of state institutions and the position of a willing hostage to someone else's geopolitical will.
I recall that long ago, well before 2014, the U.S. and EU countries systematically and consistently pushed Ukraine to curtail and limit economic cooperation with Russia. We, as the largest trade and economic partner of Ukraine, suggested discussing the emerging problems in the Ukraine-Russia-EU format. But every time we were told that Russia had nothing to do with it and that the issue concerned only the EU and Ukraine. De facto Western countries rejected Russia's repeated calls for dialogue.
Step by step, Ukraine was dragged into a dangerous geopolitical game aimed at turning Ukraine into a barrier between Europe and Russia, a springboard against Russia. Inevitably, there came a time when the concept of ”Ukraine is not Russia“ was no longer an option. There was a need for the ”anti-Russia“ concept which we will never accept.
The owners of this project took as a basis the old groundwork of the Polish-Austrian ideologists to create an ”anti-Moscow Russia“. And there is no need to deceive anyone that this is being done in the interests of the people of Ukraine. The Polish-Lithuanian Commonwealth never needed Ukrainian culture, much less Cossack autonomy. In Austria-Hungary, historical Russian lands were mercilessly exploited and remained the poorest. The Nazis, abetted by collaborators from the OUN-UPA, did not need Ukraine, but a living space and slaves for Aryan overlords.
Nor were the interests of the Ukrainian people thought of in February 2014. The legitimate public discontent, caused by acute socio-economic problems, mistakes, and inconsistent actions of the authorities of the time, was simply cynically exploited. Western countries directly interfered in Ukraine's internal affairs and supported the coup. Radical nationalist groups served as its battering ram. Their slogans, ideology, and blatant aggressive Russophobia have to a large extent become defining elements of state policy in Ukraine.
All the things that united us and bring us together so far came under attack. First and foremost, the Russian language. Let me remind you that the new ”Maidan“ authorities first tried to repeal the law on state language policy. Then there was the law on the ”purification of power“, the law on education that virtually cut the Russian language out of the educational process.
Lastly, as early as May of this year, the current president introduced a bill on ”indigenous peoples“ to the Rada. Only those who constitute an ethnic minority and do not have their own state entity outside Ukraine are recognized as indigenous. The law has been passed. New seeds of discord have been sown. And this is happening in a country, as I have already noted, that is very complex in terms of its territorial, national and linguistic composition, and its history of formation.
There may be an argument: if you are talking about a single large nation, a triune nation, then what difference does it make who people consider themselves to be – Russians, Ukrainians, or Belarusians. I completely agree with this. Especially since the determination of nationality, particularly in mixed families, is the right of every individual, free to make his or her own choice.
But the fact is that the situation in Ukraine today is completely different because it involves a forced change of identity. And the most despicable thing is that the Russians in Ukraine are being forced not only to deny their roots, generations of their ancestors but also to believe that Russia is their enemy. It would not be an exaggeration to say that the path of forced assimilation, the formation of an ethnically pure Ukrainian state, aggressive towards Russia, is comparable in its consequences to the use of weapons of mass destruction against us. As a result of such a harsh and artificial division of Russians and Ukrainians, the Russian people in all may decrease by hundreds of thousands or even millions.
Our spiritual unity has also been attacked. As in the days of the Grand Duchy of Lithuania, a new ecclesiastical has been initiated. The secular authorities, making no secret of their political aims, have blatantly interfered in church life and brought things to a split, to the seizure of churches, the beating of priests and monks. Even extensive autonomy of the Ukrainian Orthodox Church while maintaining spiritual unity with the Moscow Patriarchate strongly displeases them. They have to destroy this prominent and centuries-old symbol of our kinship at all costs.
I think it is also natural that the representatives of Ukraine over and over again vote against the UN General Assembly resolution condemning the glorification of Nazism. Marches and torchlit processions in honor of remaining war criminals from the SS units take place under the protection of the official authorities. Mazepa, who betrayed everyone, Petliura, who paid for Polish patronage with Ukrainian lands, and Bandera, who collaborated with the Nazis, are ranked as national heroes. Everything is being done to erase from the memory of young generations the names of genuine patriots and victors, who have always been the pride of Ukraine.
For the Ukrainians who fought in the Red Army, in partisan units, the Great Patriotic War was indeed a patriotic war because they were defending their home, their great common Motherland. Over two thousand soldiers became Heroes of the Soviet Union. Among them are legendary pilot Ivan Kozhedub, fearless sniper, defender of Odessa and Sevastopol Lyudmila Pavlichenko, valiant guerrilla commander Sidor Kovpak. This indomitable generation fought, those people gave their lives for our future, for us. To forget their feat is to betray our grandfathers, mothers and fathers.
The anti-Russia project has been rejected by millions of Ukrainians. The people of Crimea and residents of Sevastopol made their historic choice. And people in the southeast peacefully tried to defend their stance. Yet, all of them, including children, were labeled as separatists and terrorists. They were threatened with ethnic cleansing and the use of military force. And the residents of Donetsk and Lugansk took up arms to defend their home, their language and their lives. Were they left any other choice after the riots that swept through the cities of Ukraine, after the horror and tragedy of 2 May 2014 in Odessa where Ukrainian neo-Nazis burned people alive making a new Khatyn out of it? The same massacre was ready to be carried out by the followers of Bandera in Crimea, Sevastopol, Donetsk and Lugansk. Even now they do not abandon such plans. They are biding their time. But their time will not come.
The coup d'état and the subsequent actions of the Kiev authorities inevitably provoked confrontation and civil war. The UN High Commissioner for Human Rights estimates that the total number of victims in the conflict in Donbas has exceeded 13,000. Among them are the elderly and children. These are terrible, irreparable losses.
Russia has done everything to stop fratricide. The Minsk agreements aimed at a peaceful settlement of the conflict in Donbas have been concluded. I am convinced that they still have no alternative. In any case, no one has withdrawn their signatures from the Minsk Package of Measures or from the relevant statements by the leaders of the Normandy format countries. No one has initiated a review of the United Nations Security Council resolution of 17 February 2015.
During official negotiations, especially after being reined in by Western partners, Ukraine's representatives regularly declare their ”full adherence“ to the Minsk agreements, but are in fact guided by a position of ”unacceptability“. They do not intend to seriously discuss either the special status of Donbas or safeguards for the people living there. They prefer to exploit the image of the ”victim of external aggression“ and peddle Russophobia. They arrange bloody provocations in Donbas. In short, they attract the attention of external patrons and masters by all means.
Apparently, and I am becoming more and more convinced of this: Kiev simply does not need Donbas. Why? Because, firstly, the inhabitants of these regions will never accept the order that they have tried and are trying to impose by force, blockade and threats. And secondly, the outcome of both Minsk‑1 and Minsk‑2 which give a real chance to peacefully restore the territorial integrity of Ukraine by coming to an agreement directly with the DPR and LPR with Russia, Germany and France as mediators, contradicts the entire logic of the anti-Russia project. And it can only be sustained by the constant cultivation of the image of an internal and external enemy. And I would add – under the protection and control of the Western powers.
This is what is actually happening. First of all, we are facing the creation of a climate of fear in Ukrainian society, aggressive rhetoric, indulging neo-Nazis and militarising the country. Along with that we are witnessing not just complete dependence but direct external control, including the supervision of the Ukrainian authorities, security services and armed forces by foreign advisers, military ”development“ of the territory of Ukraine and deployment of NATO infrastructure. It is no coincidence that the aforementioned flagrant law on ”indigenous peoples“ was adopted under the cover of large-scale NATO exercises in Ukraine.
This is also a disguise for the takeover of the rest of the Ukrainian economy and the exploitation of its natural resources. The sale of agricultural land is not far off, and it is obvious who will buy it up. From time to time, Ukraine is indeed given financial resources and loans, but under their own conditions and pursuing their own interests, with preferences and benefits for Western companies. By the way, who will pay these debts back? Apparently, it is assumed that this will have to be done not only by today's generation of Ukrainians but also by their children, grandchildren and probably great-grandchildren.
The Western authors of the anti-Russia project set up the Ukrainian political system in such a way that presidents, members of parliament and ministers would change but the attitude of separation from and enmity with Russia would remain. Reaching peace was the main election slogan of the incumbent president. He came to power with this. The promises turned out to be lies. Nothing has changed. And in some ways the situation in Ukraine and around Donbas has even degenerated.
In the anti-Russia project, there is no place either for a sovereign Ukraine or for the political forces that are trying to defend its real independence. Those who talk about reconciliation in Ukrainian society, about dialogue, about finding a way out of the current impasse are labelled as ”pro-Russian“ agents.
Again, for many people in Ukraine, the anti-Russia project is simply unacceptable. And there are millions of such people. But they are not allowed to raise their heads. They have had their legal opportunity to defend their point of view in fact taken away from them. They are intimidated, driven underground. Not only are they persecuted for their convictions, for the spoken word, for the open expression of their position, but they are also killed. Murderers, as a rule, go unpunished.
Today, the ”right“ patriot of Ukraine is only the one who hates Russia. Moreover, the entire Ukrainian statehood, as we understand it, is proposed to be further built exclusively on this idea. Hate and anger, as world history has repeatedly proved this, are a very shaky foundation for sovereignty, fraught with many serious risks and dire consequences.
All the subterfuges associated with the anti-Russia project are clear to us. And we will never allow our historical territories and people close to us living there to be used against Russia. And to those who will undertake such an attempt, I would like to say that this way they will destroy their own country.
The incumbent authorities in Ukraine like to refer to Western experience, seeing it as a model to follow. Just have a look at how Austria and Germany, the USA and Canada live next to each other. Close in ethnic composition, culture, in fact sharing one language, they remain sovereign states with their own interests, with their own foreign policy. But this does not prevent them from the closest integration or allied relations. They have very conditional, transparent borders. And when crossing them the citizens feel at home. They create families, study, work, do business. Incidentally, so do millions of those born in Ukraine who now live in Russia. We see them as our own close people.
Russia is open to dialogue with Ukraine and ready to discuss the most complex issues. But it is important for us to understand that our partner is defending its national interests but not serving someone else's, and is not a tool in someone else's hands to fight against us.
We respect the Ukrainian language and traditions. We respect Ukrainians' desire to see their country free, safe and prosperous.
I am confident that true sovereignty of Ukraine is possible only in partnership with Russia. Our spiritual, human and civilizational ties formed for centuries and have their origins in the same sources, they have been hardened by common trials, achievements and victories. Our kinship has been transmitted from generation to generation. It is in the hearts and the memory of people living in modern Russia and Ukraine, in the blood ties that unite millions of our families. Together we have always been and will be many times stronger and more successful. For we are one people.
Today, these words may be perceived by some people with hostility. They can be interpreted in many possible ways. Yet, many people will hear me. And I will say one thing – Russia has never been and will never be ”anti-Ukraine“. And what Ukraine will be – it is up to its citizens to decide.

As I've stated before, during the COVID-19 pandemic, it is of utmost importance that we all "follow the money". It's the only way to unravel the ever-complicated narrative that has evolved over the past 16 months. One of the key aspects of the issue is to track the allegiances and connections that key players have to each other. As you will see in this posting, a prime example can be found simply by looking at the connections that the Members of the Board of Directors at Pfizer have to other key players in the "COVID game".
Here is a graphic showing the Board as a whole

Now, let's focus on three members:
1.) Noting that the Food and Drug Administration (FDA) is the gatekeeper that stands between our safety and the products being promoted by Big Pharma, here is the CV for Pfizer board member Scott Gottlieb:

2.) Noting that Bill Gates, the world's pre-eminent untrained vaccinologist and epidemiologist, has the goal to vaccinate the entire world, hasn't yet seen a health condition that a vaccine couldn't fix and that he is the co-founder of the Bill & Melinda Gates Foundation, the second largest financial supporter of the World Health Organization, that the World Economic Forum is the architect and promoter of the dystopic post-pandemic Great Reset and that Facebook has been one of the gatekeepers of the pro-vaccine narrative, here is the CV for Pfizer board member Susan Desmond-Hellmann:

3.) Noting that the mainstream media has essentially been the mouthpiece of governments during the pandemic, that they have taken it upon themselves to create and disseminate COVID-19 fear porn and promote experimental COVID-19 vaccines 24 hours a day, 7 days a week and that Thompson Reuters is the world's leading provider of news and claims to be one of the "world's most trusted providers of answers", here is the CV for Pfizer board member James Smith:

Piece by piece, the puzzle comes together. While I am well aware that most major corporations want to attract board "talent" that will assist in promoting their business, the links between three of Pfizer's board members, the FDA, Facebook, Bill & Melinda Gates Foundation, the WEF and Thompson Reuters is what can only be termed "an amazing coincidence".
-
COVID-19 vaccination is voluntary research. The COVID-19 public vaccination program operated by the CDC and the FDA is a clinical investigation and under no circumstance can any person receive pressure, coercion, or threat of reprisal on their free choice of participation. Violation of this principle of autonomy by any entity constitutes reckless endangerment with a reasonable expectation of causing personal injury resulting in damages.
-
COVID-19 vaccines do not work well enough. The current COVID-19 vaccines are not sufficiently protective against contracting COVID-19 to support its use beyond the current voluntary participation in the CDC sponsored program. A total of 10,262 SARS-CoV-2 vaccine breakthrough infections had been reported from 46 U.S. states and territories as of April 30, 2021. Among these cases, 6,446 (63%) occurred in females, and the median patient age was 58 years (interquartile range = 40–74 years). Based on preliminary data, 2,725 (27%) vaccine breakthrough infections were asymptomatic, 995 (10%) patients were known to be hospitalized, and 160 (2%) patients died. Among the 995 hospitalized patients, 289 (29%) were asymptomatic or hospitalized for a reason unrelated to COVID-19. The median age of patients who died was 82 years (interquartile range = 71–89 years); 28 (18%) decedents were asymptomatic or died from a cause unrelated to COVID-19. Sequence data were available from 555 (5%) reported cases, 356 (64%) of which were identified as SARS-CoV-2 variants of concern, including B.1.1.7 (199; 56%), B.1.429 (88; 25%), B.1.427 (28; 8%), P.1 (28; 8%), and B.1.351 (13; 4%). None of these variants are encoded in the RNA or DNA of the current COVID-19 vaccines. In response to these numerous reports, the CDC announced on May 1, 2021, that community breakthrough cases would no longer be reported to the public and only those vaccine failure cases requiring hospitalization will be reported, presumably on the CDC website (https://www.cdc.gov/mmwr/volumes/70/wr/mm7021e3.htm)
-
COVID-19 vaccines have a dangerous mechanism of action. The Pfizer, Moderna, and JNJ vaccines are considered "genetic vaccines" or vaccines produced from gene therapy molecular platforms.[i] [ii] They have a injurious mechanism of action in that they all cause the body to make an uncontrolled quantity of the pathogenic spike protein from the SARS-CoV-2 virus. This is unlike all other vaccines where there is a set amount of antigen or live-attenuated virus. This means for the Pfizer, Moderna, and JNJ vaccines it is not predictable among patients who will produce more or less of the spike protein. The spike protein itself has been demonstrated to injure vital organs such as the brain, heart, lungs, as well as damage blood vessels and directly cause blood clots. Additionally, because these vaccines infect cells within these organs, the generation of spike protein within heart and brain cells in particular, causes the body's own immune system to attack these organs.
-
There is a burgeoning number of cases of myocarditis or heart inflammation among individuals below age 30 years.[iii] The Centers for Disease Control has held emergency meetings on this issue and the medical community is responding to the crisis and the US FDA has issued a warning on the Pfizer and Moderna vaccines for myocarditis.[iv] It is known that myocarditis causes injury to heart muscle cells and may result in permanent heart damage leading to heart failure, arrhythmias, and cardiac death. Because this risk is not predictable and the early reports may represent just the tip of the iceberg, no individual under age 30 under any set of circumstances should feel any obliged to take this risk with the current genetic vaccines particular the Pfizer and Moderna products.
-
The US FDA has given an update on the JNJ vaccine concerning the risk of cerebral venous sinus thrombosis in women ages 18-48 associated with low platelet counts.[v] Because this risk is not predictable no woman under age 48 under any set of circumstances should feel any obliged to take this risk with the JNJ vaccine.
-
COVID-19 vaccines are generating record safety reports. In 1990, the Vaccine Adverse Event Reporting Systems (“VAERS”) was established as a national early warning system to detect possible safety problems in U.S. licensed vaccines.[vi] VAERS is a passive reporting system, meaning it relies on individuals to voluntarily send in reports of their experiences to CDC and FDA. VAERS is useful in detecting unusual or unexpected patterns of adverse event reporting that might indicate a possible safety problem with a vaccine. The total safety reports in VAERS all vaccines per year up to 2019 was 16,320. The total safety reports in VAERS for COVID Vaccines alone through June 25, 2021 is 411,931.[vii]
-
People are dying and being hospitalized in record numbers in the days after COVID-19 vaccination. Based on VAERS as of June 25, 2021, there were 6,985 COVID-19 vaccine deaths reported and over 23,257 hospitalizations reported for the COVID-19 vaccines (Pfizer, Moderna, JNJ). By comparison, from 1999, until December 31, 2019, VAERS received 3167 death reports (158 per year) adult death reports for all vaccines combined. Thus, the COVID-19 mass vaccination is associated with at least 39-fold increase annualized vaccine deaths reported to VAERS. COVID-19 vaccine adverse events account for 98% of all vaccine-related AEs from Dec 2020 through present in VAERS.
-
The safety profile is unknown and there is a reasonable expectation for harm for the following groups at all age ranges: COVID-19 recovered, suspected COVID-19 recovered, women of childbearing potential, children, persons with one or more chronic diseases.
-
Any personal choice or protected health information concerning the COVID-19 vaccine and its complications is confidential and anonymous according to federal law, otherwise, you will be subject to additional federal fines and penalties for violation of protected health information laws and statutes.
In conclusion, the investigational, genetic COVID-19 vaccines are not safe for general use and cannot be deployed indiscriminately unless proven otherwise. Please cease and desist pressure/harassment/mandates for COVID-19 vaccination.
-
A recently published study in this month’s American Journal of Therapeutics, took an in-depth look at 18 randomized controlled studies on the use of Ivermectin to control COVID-19. The study concludes that the use of Ivermectin “significantly reduced risks of contracting COVID-19” and “found large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.”
Ivermectin was first developed as a veterinary drug in the 1970s, however since 1988 it has been prescribed for humans to combat various parasitic infections. Was later added to the WHO’s list of essential medications and in 2015 the inventors were awarded the Nobel Prize in Medicine.
With the outbreak of COVID-19, many doctors and scientists were looking for new ways to deal with the virus. At the same time, an interesting series of events occurred one nursing home in Toronto, in February 2020 (just before COVID-19 emerged in Canada the Valley View Nursing Home in Toronto, Canada had a parasitic outbreak. 170 patients at the home were given Ivermectin. The residents of the 4th floor, where the outbreak occurred, were given the highest dose; the rest of the residents were given a prophylactic dose. The staff were not given Ivermectin. Then they had a Covid-19 outbreak. The staff were infected with COVID-19 much more than the patients. Only 6 patients contracted COVID, and they all had mild cases. The patients on the 4th floor, who received the highest dose of ivermectin, had no cases of COVID. These patients were very elderly with comorbidities, and they had much contact with the staff yet only 6% were infected.
Since then, over 60 clinical trials (31 randomized controlled) conducted by 549 scientists in 18,931 patients were conducted to see what if any link Ivermectin has with preventing and treating COVID-19. The conclusions of these studies reveal dramatic positive outcomes for the use of Ivermectin. When used prophylactically patients saw an 85% reduction in hospitalization and death, early treatment was effective 76%, and even when used as a later stage treatment was effective 46% of the time.
While these studies suggested that Ivermectin was indeed a safe, cheap, and effective treatment for COVID-19, many public health policy makers refused to permit its use to treat and prevent COVID-19. The FDA in it’s statement said that the “FDA has not approved ivermectin for use in treating or preventing COVID-19” later explaining that “The FDA has not reviewed data to support use of ivermectin in COVID-19 patients to treat or to prevent COVID-19”. Many are insisting it’s time for the FDA to review the data and formally approve its use.
One such advocate for the use of Ivermectin is Dr. Pierre Kory, a founder of Front Line COVID-19 Critical Care Alliance (FLCCC). Kory, along with the other professionals at the FLCCC developed the specific protocol to prevent and treat COVID-19 using Ivermectin. While the treatment was shunned by the medical establishment and the social media banned promoting or debating the treatment, physicians, like Kory, persisted and advocated for its use. In December 2020 Dr. Kory and others gave an impassioned plea, backed by scientific research at a committee hearing in the U.S. Senate. Stating that Ivermectin “basically obliterates transmission of this virus,” the doctor continued saying “When I say miracle I do not use that term lightly[.] … [T]hat is a scientific recommendation based on mountains of data that has emerged in the last three months.”
Unfortunately, many are still uninformed of this treatment, and the medical establishment is still blocking its use. Several hospitals around the country are even refusing to administer the treatment to seriously ill patients. A number of patients had to go as far as to get a court order to force the hospital to permit them to use this life saving medication. Thankfully all of those patients received their Ivermectin and made dramatic turnarounds and subsequently recovered for COVID-19.
The hope of a safe and effective medication to prevent and treat COVID-19 appears to have been found in Ivermectin; unfortunately it continues to be deemed unacceptable by the medical establishment and undiscussable by social media.